4368
Hippocampal volume, DTI parameters, and relaxation time T1 in postmortem patients with amyotrophic lateral sclerosis and healthy controls1Institute of Forensic Medicine, Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 2Institute of Forensic Medicine, Health-Department Basel-Stadt, Basel, Switzerland, 3Neurology Clinic and Policlinic, Department of Clinical Research, University Hospital Basel, Basel, Switzerland, 4Translational Imaging in Neurology (ThINk), Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 5Division of Radiological Physics, Department of Radiology and Nuclear Medicine, University Hospital Basel, Basel, Switzerland
Synopsis
Keywords: Other Neurodegeneration, Brain
Motivation: MRI parameters of the hippocampus could serve as an imaging biomarker for amyotrophic lateral sclerosis (ALS).
Goal(s): To compare hippocampal volume, fractional anisotropy (FA), mean diffusivity (MD), and T1 between ALS and healthy controls (HC).
Approach: Postmortem in situ MRI scans at 3 Tesla were performed on five deceased ALS patients and seven deceased neurologically healthy controls (HC). MP2RAGE and DTI sequences were employed.
Results: A potentially significant difference between ALS and HC was found for T1 in the right hippocampus and for MD in the left, right, and total hippocampus. Further research is needed to confirm this outcome.
Impact: The potential effect of amyotrophic lateral sclerosis on the hippocampal mean diffusivity and T1 might lead to the development of new MRI biomarkers. This could improve diagnosis, prognosis, and treatment strategies. Larger sample sizes are needed to validate the results.
INTRODUCTION
Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disease1. Some studies found a potential influence on the hippocampus2–6. However, the relation between ALS and hippocampus has not yet been extensively investigated. Moreover, several studies used postmortem (PM) formalin-fixed brain samples or employed equipment not routinely used in the clinics, which limits a translation of the findings.The goal of this study was to compare the hippocampal volume, fractional anisotropy (FA), mean diffusivity (MD), and T1 between deceased patients with ALS and healthy PM controls (HC). The objective was to determine if any of these parameters could serve as an imaging biomarker for ALS.
METHODS
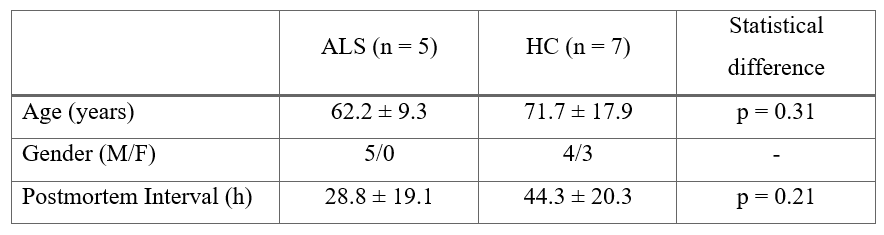
Five deceased patients with a clinical diagnosis of definite ALS according to the revised El Escorial criteria7 were included in this study (ethical approval: BASEC-Nr. 2020-02179). One patient showed no pathological aggregation of phosphorylated 43 kDa TAR DNA-binding protein (pTDP-43) in PM histological evaluation and was infected with COVID-19 before death. The HC group consisted of seven deceased people with no known neurological diseases. Table 1 provides an overview of the groups.All deceased were stored at 4°C. PM in situ MRI scans (3 Tesla Siemens MAGNETOM Prisma) were performed, i.e., the un-fixed brain remained within the skull, using the following sequences:
- Magnetization-prepared two rapid acquisition gradient echo (MP2RAGE)8 with 176 slices per slab, FoV = 240 × 256 mm, TR = 5000 ms, TE = 2.98 ms, TI = 700 and 2500 ms, flip angle = 4° and 5°, echo spacing: 7.1 ms, GRAPPA acceleration factor 3, isotropic resolution of 1x1x1 mm3: hippocampal masks and volume, T1 maps
- Diffusion-weighted single-shot echo-planar imaging DTI with b = 2000 s/mm2, 64 isotropically distributed diffusion directions, 3 b = 0 s/mm2, echo time (TE) = 109 ms, repetition time (TR) = 18700 ms, 100 slices, isotropic resolution of 1.8 mm3: FA and MD maps
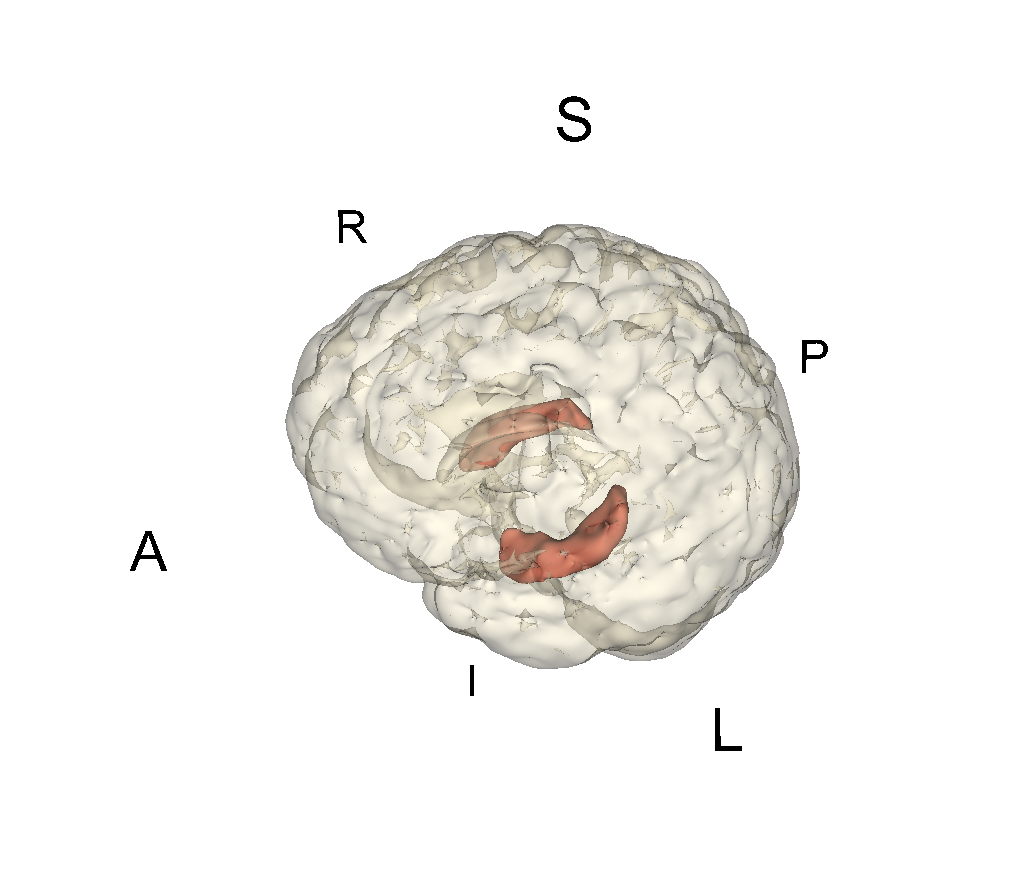
The brain was segmented using FSL (FMRIB Software Library10) BET11 and the hippocampus (left, right, and total) via FSL FIRST12. The hippocampal volume was calculated using the retrieved masks and fslstats. The DTI data was corrected for eddy currents (FSL’s eddy_correct13) and the FA and MD maps were retrieved via FSL’s dtifit. After registration of the maps to the MP2RAGE data and multiplication with the hippocampal masks, the mean hippocampal MD and FA values were calculated. The masks were further multiplied with the MP2RAGE data. A publicly available python package14,15 was adapted to compute the corresponding T1 mean values.
Each parameter was statistically compared between ALS and HC using a two-tailed independent t-test with Bonferroni correction (implemented in python). The significance level was 0.05.
RESULTS
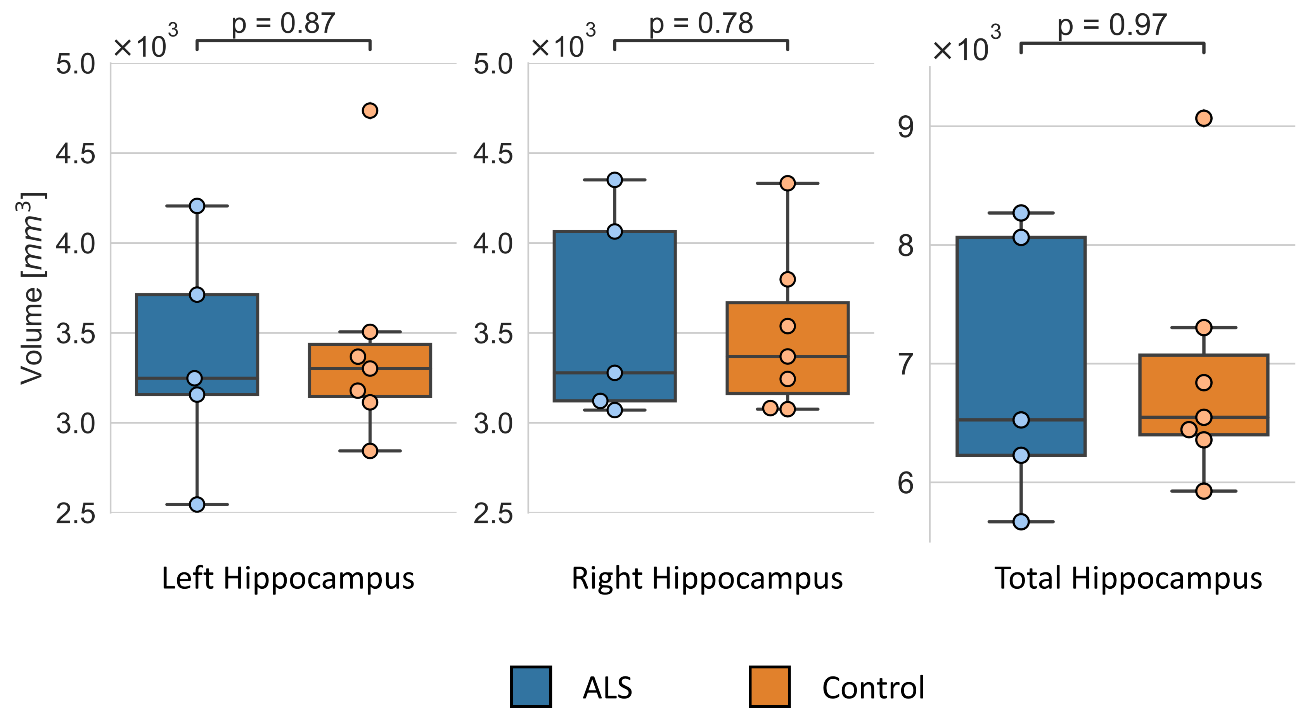
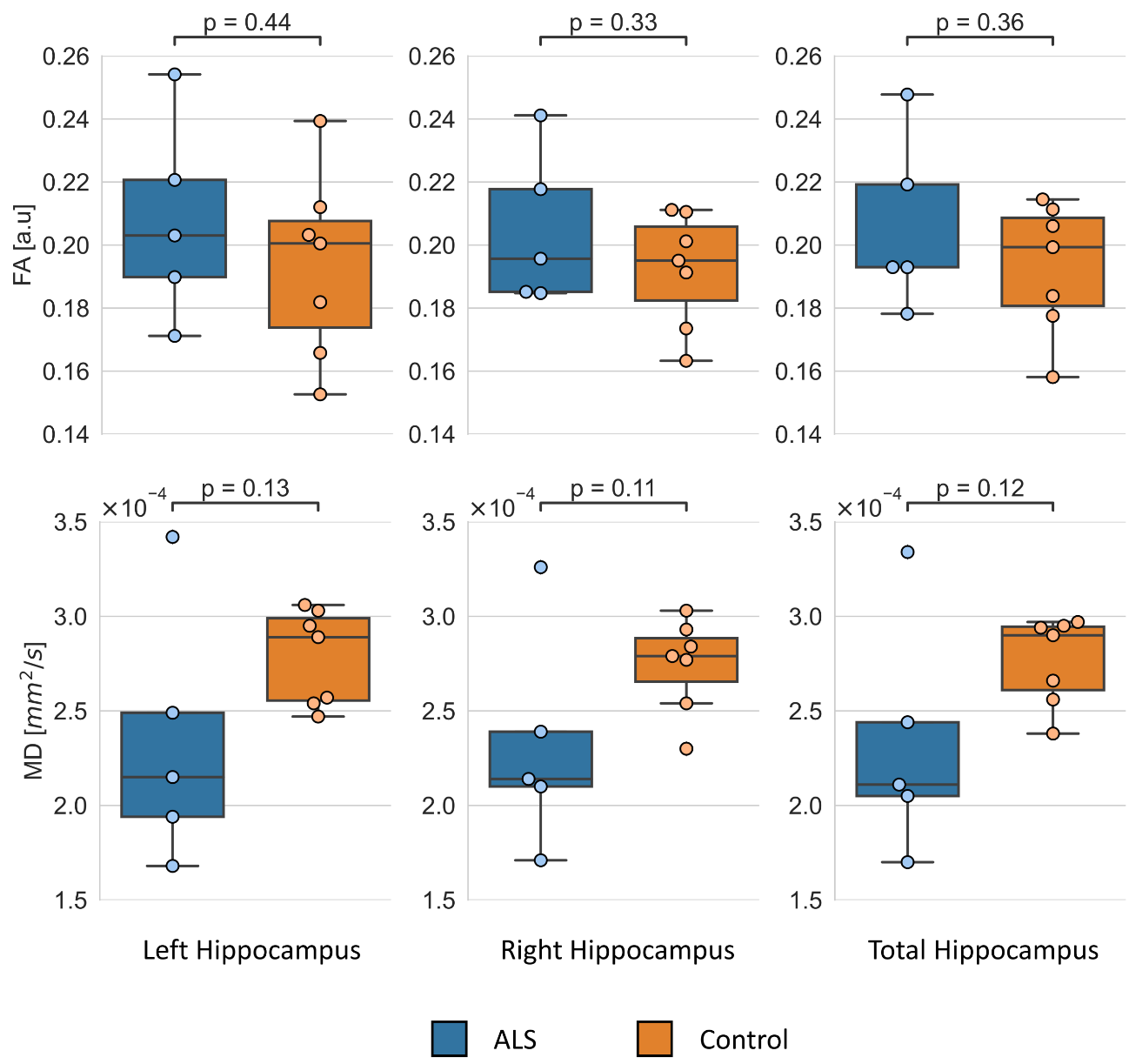
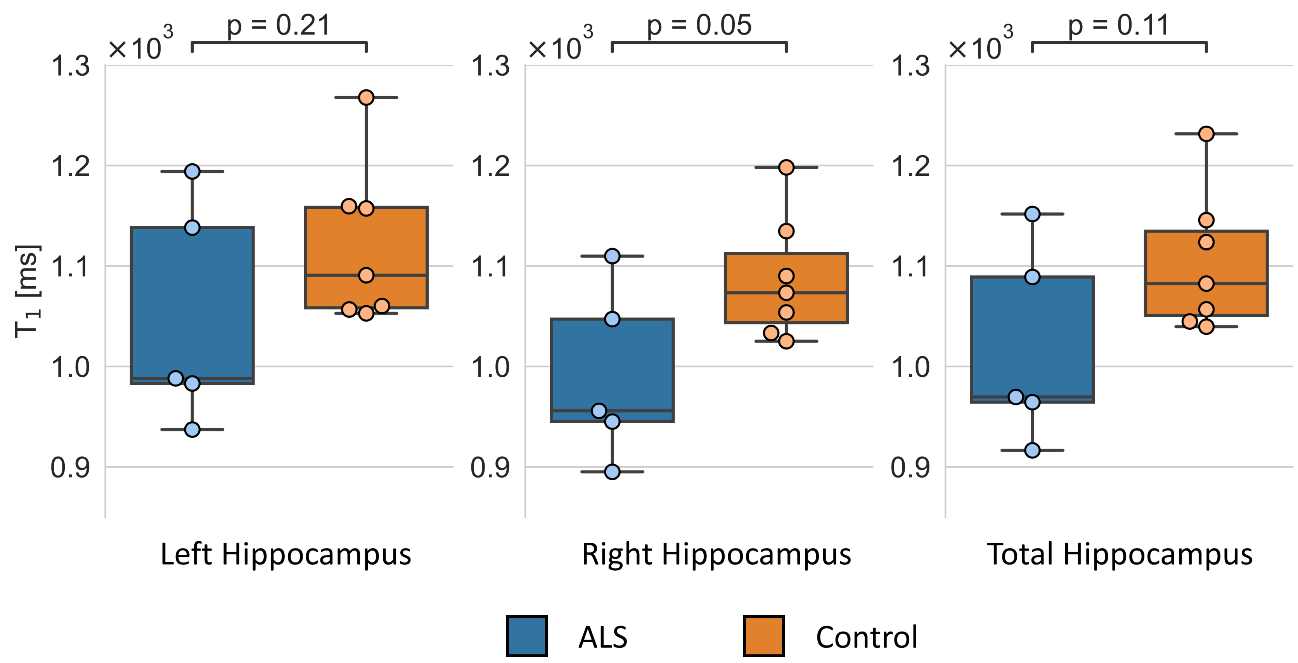
An exemplary hippocampus segmentation is shown in Figure 1. The volume comparisons are presented in Figure 2. No significant volume difference was found. The results of the FA and MD comparison are illustrated in Figure 3. No significant DTI difference was found. However, the patient with ALS who additionally had COVID-19 and showed no pTDP-43 pathology can be identified as an outlier in the MD results. Exclusion of this patient resulted in a significant MD difference for left (p = 0.003), right (p = 0.003), and total hippocampus (p = 0.002). The results of the longitudinal relaxation time T1 are shown in Figure 4. A significant difference was found for the right hippocampus.DISCUSSION
The volumes, FA, MD, and T1 of the left, right, and total hippocampus were compared PM between ALS and HC. A just significant difference was found for T1 in the right hippocampus. However, one patient with ALS was infected with COVID-19 before death influencing the diffusivities in the brain16,17. Moreover, this patient showed no pTDP-43 pathology, potentially indicating a different molecular expression of ALS. Excluding this patient, led to a significant MD difference for left, right, and total hippocampus. Further studies with larger sample sizes and histological evaluations are needed to confirm the significant differences between ALS and HC.CONCLUSION
The results suggest that hippocampal MD and right hippocampal T1 might be significantly different in ALS compared to HC. Further research is required to confirm this outcome and to better understand the underlying mechanisms. A significant difference observed via MRI would allow to define a new clinically useful biomarker for ALS.Acknowledgements
This study was funded in part by grants of the Neuromuscular Research Association Basel (NeRAB, to RS), and the Stiftung zur Förderung der gastroenterologischen und der allgemeinen klinischen Forschung sowie der medizinischen Bildauswertung (RS). The funders did not play any role in study conceptualization, design, acquisition, analysis and interpretation of the study.References
1. Goutman SA, Hardiman O, Al-Chalabi A, et al. Recent advances in the diagnosis and prognosis of amyotrophic lateral sclerosis. Lancet Neurol. 2022;21(5):480-493. doi:10.1016/S1474-4422(21)00465-8
2. Reuck JD, Auger F, Durieux N, et al. Post-mortem 7.0-Tesla Magnetic Resonance Imaging of the Hippocampus in Amyotrophic Lateral Sclerosis. OBM Geriatr. 2020;4(4):1-7. doi:10.21926/obm.geriatr.2004143
3. Mollink J, Hiemstra M, Miller KL, et al. White matter changes in the perforant path area in patients with amyotrophic lateral sclerosis. Neuropathol Appl Neurobiol. 2019;45(6):570-585. doi:10.1111/nan.12555
4. Christidi F, Karavasilis E, Rentzos M, et al. Hippocampal pathology in amyotrophic lateral sclerosis: selective vulnerability of subfields and their associated projections. Neurobiol Aging. 2019;84:178-188. doi:10.1016/j.neurobiolaging.2019.07.019
5. Takeda T, Uchihara T, Arai N, Mizutani T, Iwata M. Progression of hippocampal degeneration in amyotrophic lateral sclerosis with or without memory impairment: distinction from Alzheimer disease. Acta Neuropathol (Berl). 2009;117(1):35-44. doi:10.1007/s00401-008-0447-2
6. Raaphorst J, van Tol MJ, de Visser M, et al. Prose memory impairment in amyotrophic lateral sclerosis patients is related to hippocampus volume. Eur J Neurol. 2015;22(3):547-554. doi:10.1111/ene.12615
7. Ludolph A, Drory V, Hardiman O, et al. A revision of the El Escorial criteria - 2015. Amyotroph Lateral Scler Front Degener. 2015;16(5-6):291-292. doi:10.3109/21678421.2015.1049183
8. Marques JP, Kober T, Krueger G, van der Zwaag W, Van de Moortele PF, Gruetter R. MP2RAGE, a self bias-field corrected sequence for improved segmentation and T1-mapping at high field. NeuroImage. 2010;49(2):1271-1281. doi:10.1016/j.neuroimage.2009.10.002
9. Berger C, Bauer M, Scheurer E, Lenz C. Temperature correction of post mortem quantitative magnetic resonance imaging using real-time forehead temperature acquisitions. Forensic Sci Int. 2023;348:111738. doi:10.1016/j.forsciint.2023.111738
10. Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SM. FSL. NeuroImage. 2012;62(2):782-790. doi:10.1016/j.neuroimage.2011.09.015
11. Smith SM. Fast robust automated brain extraction. Hum Brain Mapp. 2002;17(3):143-155. doi:10.1002/hbm.10062
12. Patenaude B, Smith SM, Kennedy DN, Jenkinson M. A Bayesian model of shape and appearance for subcortical brain segmentation. NeuroImage. 2011;56(3):907-922. doi:10.1016/j.neuroimage.2011.02.046
13. Andersson JLR, Sotiropoulos SN. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. NeuroImage. 2016;125:1063-1078. doi:10.1016/j.neuroimage.2015.10.019
14. Hollander G de. PyMP2RAGE. February 2023. https://github.com/Gilles86/pymp2rage. Accessed August 2, 2023.
15. GitHub - JosePMarques/MP2RAGE-related-scripts: MP2RAGE Scripts - T1 map correction & Background noise removal. https://github.com/JosePMarques/MP2RAGE-related-scripts. Accessed August 2, 2023.
16. Caroli A, Capelli S, Napolitano A, et al. Brain diffusion alterations in patients with COVID-19 pathology and neurological manifestations. NeuroImage Clin. 2023;37:103338. doi:10.1016/j.nicl.2023.103338
17. Liang H, Ernst T, Oishi K, et al. Abnormal brain diffusivity in participants with persistent neuropsychiatric symptoms after COVID-19. NeuroImmune Pharmacol Ther. 2023;2(1):37-48. doi:10.1515/nipt-2022-0016Figures