4343
Improving Outcomes in Deep Brain Stimulation: A Comparative Study of 7T versus 3T Targeting1Mayo Clinic, Jacksonville, FL, United States
Synopsis
Keywords: Other Neurodegeneration, High-Field MRI, Surgical Planning, Essential Tremor, Deep Brain Stimulation, Neuromodulation
Motivation: 7T MRI offers improved image quality for deep brain stimulation (DBS) targeting, but greater distortion and artifacts that could lead to inaccurate targeting.
Goal(s): Our goal was to compare outcomes in DBS for essential tremor between patients targeted using 3T versus 7T MRI.
Approach: Retrospective comparison of DBS patients with ET was performed with patients targeted using 3T versus 7T MRI. We assessed differences in tremor improvement, adverse events, and electrode positioning.
Results: ET DBS patients targeted with 7T had significantly greater tremor control compared to 3T, as well as lower stimulation currents and improved electrode precision.
Impact: Despite challenges of 7T MRI in surgical planning, outcomes in DBS for ET were improved by use of 7T MRI versus 3T MRI, including better tremor control, reduced stimulation currents, and greater precision.
Introduction
Deep brain stimulation (DBS) is an established treatment for various neurological disorders, but outcomes are variable, largely influenced by precision in surgical targeting. Despite growing interest in MRI visualization for direct targeting, there's a recognized variability between results from 1.5T, 3T, and 7T MRI.1-3 While 7T MRI offers superior target visualization,4 concerns about geometric distortions potentially leading to inaccurate electrode placement have limited its widespread adoption for DBS.5 This study compares patient outcomes targeted with 7T MRI versus 3T MRI for essential tremor (ET).Methods
A retrospective study was conducted for patients undergoing unilateral thalamic DBS for essential tremor between 2021 and 2023. Two matched cohorts were assessed, one using 7T MRI and the other using 3T MRI for surgical planning. The primary endpoint was percentage improvement in Fahn-Tolosa-Marin Tremor Rating Scale (TRS). Additionally, we assessed optimized programming settings and variance in electrode position on post-operative imaging. Demographic and clinical data were compared using a nonparametric Mann-Whitney test. The squared Euclidean distance of each individual contact from the group mean centroid was calculated and averaged across the entire cohort to provide the variance (i.e., the mean squared distance) of electrode contact position.Results
A total of 34 patients were analyzed, with 17 in each cohort. There were no significant differences in demographic information or surgical dates between groups. There were no differences in intraoperative target repositioning or adverse events. The 7T group had a significantly greater TRS improvement compared with 3T (64.9% ± 11.4 versus 50.9% ± 16.4; p=0.004). Patients in the 7T cohort also had a lower mean stimulation current compared with 3T patients (2.0 ± 0.8 mA versus 2.7 ± 0.9 mA ; p=0.01). Image evaluation revealed that although the mean electrode position was comparable between 7T and 3T, the 7T electrode positioning was more clustered, indicating a lower variance in final electrode location. For the electrode tip, the variance in contact position was 3.8 mm at 7T and 8.2 mm at 3T.Discussion
Our study highlights the advantages of using 7T MRI for DBS targeting for ET, with improved outcomes in patients targeted with 7T. Electrode positions reveal greater precision with 7T imaging than 3T. Patients in the 7T cohort also required lower stimulation currents, suggesting more accurate targeting. Additionally, despite similar average electrode locations between both groups, there was reduced variance in final electrode positioning with 7T MRI. While concerns have been raised about geometric distortions at 7T, with careful imaging parameter selection and registration processes, these potential distortions can be mitigated, as reflected in the superior outcomes of the 7T cohort.Conclusion
The study supports the efficacy of 7T MRI for preoperative targeting in DBS for ET treatment. It demonstrates improved tremor outcomes, reduced stimulation current, and greater precision in electrode positioning. The concerns regarding geometric distortions at 7T MRI seem to be outweighed by the advantages of improved image quality and resultant precision in DBS targeting. Future studies can further explore the full potential of 7T MRI in various neurological conditions.Acknowledgements
No acknowledgement found.References
1. van Laar PJ, Oterdoom DL, Ter Horst GJ, et al. Surgical Accuracy of 3-Tesla Versus 7-Tesla Magnetic Resonance Imaging in Deep Brain Stimulation for Parkinson Disease. World Neurosurg. Sep 2016;93:410-2. doi:10.1016/j.wneu.2016.06.084
2. Bot M, Verhagen O, Caan M, et al. Defining the Dorsal STN Border Using 7.0-T MRI: A Comparison to Microelectrode Recordings and Lower Field Strength MRI. Stereotact Funct Neurosurg. 2019;97(3):153-159. doi:10.1159/000500109
3. Isaacs BR, Heijmans M, Kuijf ML, et al. Variability in subthalamic nucleus targeting for deep brain stimulation with 3 and 7 Tesla magnetic resonance imaging. Neuroimage Clin. 2021;32:102829. doi:10.1016/j.nicl.2021.102829
4. Tao S, Zhou X, Westerhold EM, Middlebrooks EH, Lin C. Optimization of fast gray matter acquisition T1 inversion recovery (FGATIR) on 7T MRI for deep brain stimulation targeting. Neuroimage. May 15 2022;252:119043. doi:10.1016/j.neuroimage.2022.119043
5. Dammann P, Kraff O, Wrede KH, et al. Evaluation of hardware-related geometrical distortion in structural MRI at 7 Tesla for image-guided applications in neurosurgery. Acad Radiol. Jul 2011;18(7):910-6. doi:10.1016/j.acra.2011.02.011
Figures
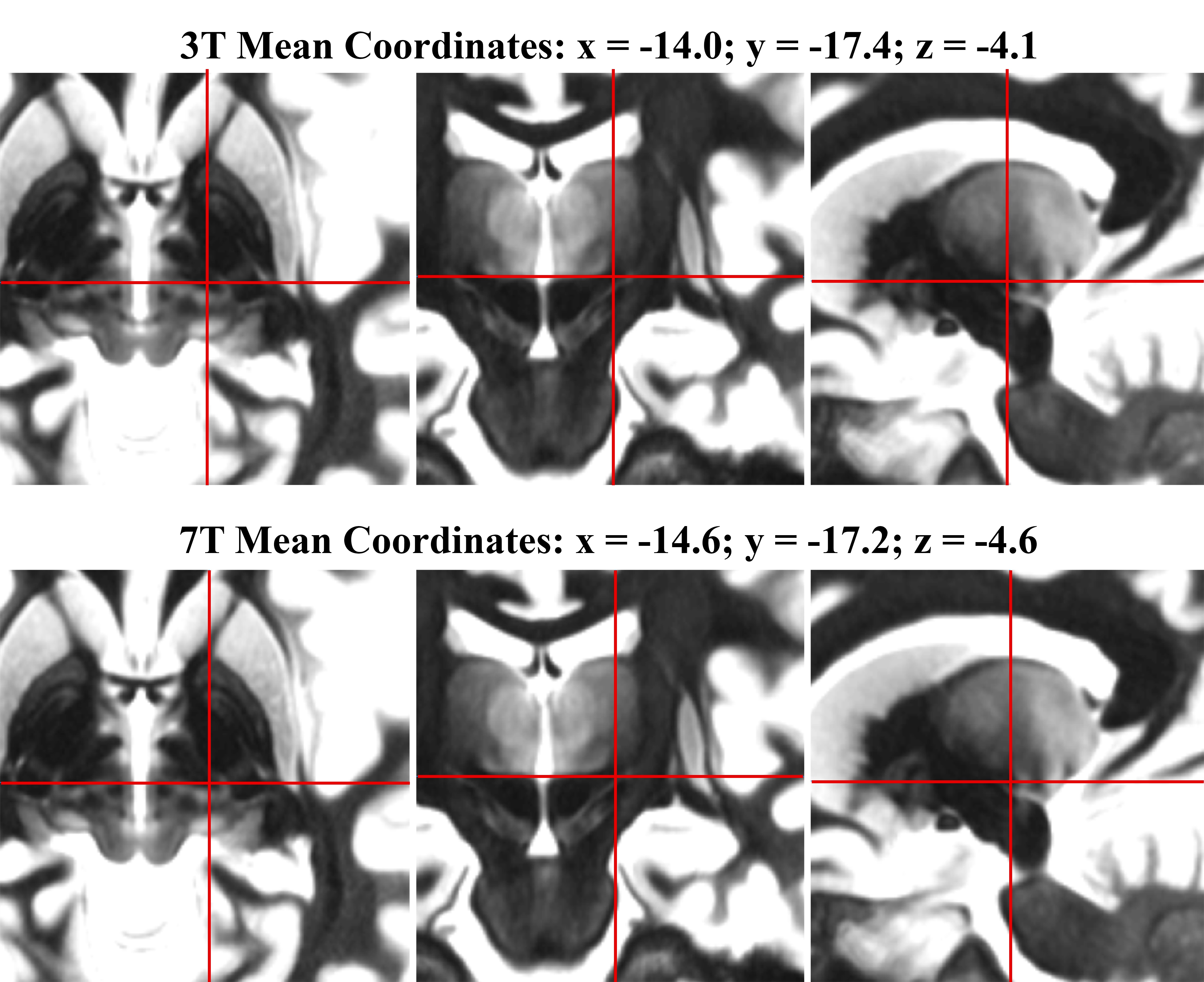
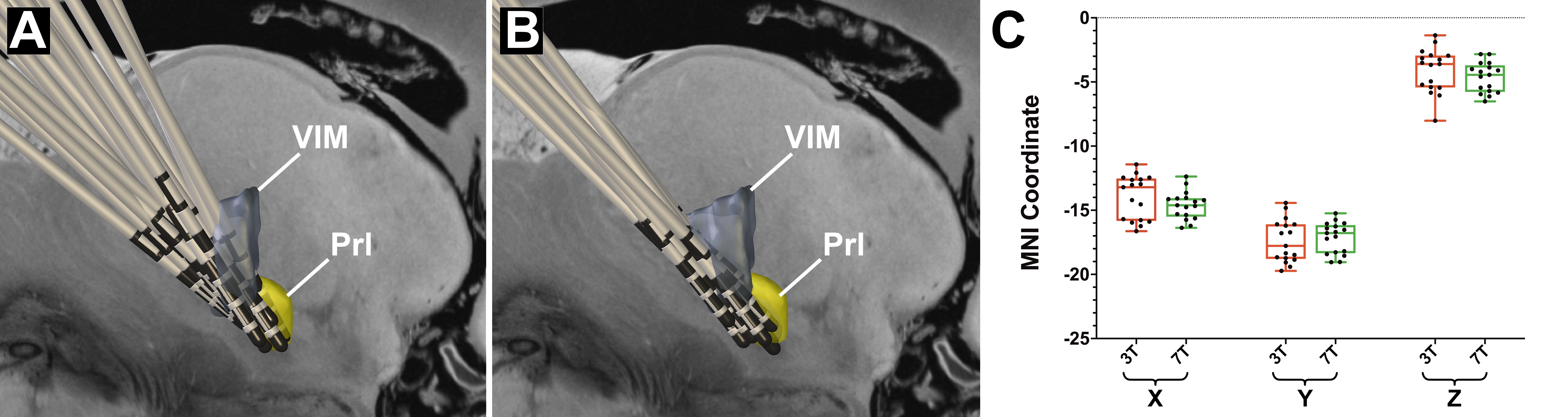
Figure 3. Normalized electrode locations for (A) 3T and (B) 7T groups relative to the ventral intermediate nucleus (VIM; gray region) and the prelemniscal radiations (Prl; yellow region). (C) Montreal Neurological Institute (MNI) template space coordinates for the electrode tip in the 3T and 7T cohorts (all p>0.2). Box plot illustrates median and 25th/75th percentile, and whiskers represents minimum and maximum values.