4335
Exploring latent space representations of T1/T2 relaxation, cardiac motion, and respiratory motion for multidimensional quantitative CMR1Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 2Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 3Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Signal Representations, Cardiovascular, Cardiac binning, respiratory binning, motion identification, variational autoencoder (VAE), multidimensional quantitative imaging
Motivation: Respiratory and cardiac motion identification is challenging with changing contrast weightings for self-gated multidimensional techniques like MR multitasking.
Goal(s): To guide VAE latent vector constraints design for representing relaxation and motion.
Approach: We evaluated VAE representational fidelity for 16 combinations of constraints on T1/T2 relaxation, cardiac, and respiratory latent dimensions.
Results: The results demonstrate that nonlinear T1/T2 relaxation representations and cardiac phase representations improve VAE performance.
Impact: Latent space design is important for VAE learning in multidimensional cardiac imaging, suggesting avenues for better self-gated cardiac and respiratory binning.
Introduction
Quantitative cardiovascular magnetic resonance (CMR) imaging evaluates and quantifies various aspects of the cardiovascular system but is prone to cardiac and respiratory motion artifacts. Multidimensional techniques such as MR multitasking1capture cardiac and/or respiratory motion throughout the NMR relaxation process to facilitate motion-resolved quantitative CMR. For self-gated techniques, this brings the added challenge of respiratory and/or cardiac motion identification from (k,t)-space data with fast-changing contrast weightings. MR Multitasking uses Bloch-subspace k-means clustering to assign cardiac and respiratory motion bins, but even more robust methods are sought. Deep learning approaches have been explored2including work to identify motion in T1-recovery using a variational autoencoder (VAE) with latent vector constraints3. Here, we investigate several VAE latent vector constraint designs for representing cardiac and respiratory motion in T2prepared-inversion recovery (T2IR) experiments with known sequence timing (inversion times and T2 prep durations), using a numerical phantom.Methods
Numerical phantomThe XCAT numerical phantom was modified to simulate a pulse sequence that cycles through five T2IR preparation durations and gradient echo readouts during T1 recovery. The image signal has four independent variables: inversion time (T1 recovery), T2prep index, cardiac phase, and respiratory state. A self-gating signal was simulated, and its SVD was used to define an input for the VAE.
VAE structure
We sought a VAE capable of learning a latent space whose dimensions are direct representations of the four underlying independent variables, implementing an encoder and decoder with dense multilayer perceptrons and ReLU activation. The encoder includes four layers with 25, 50, 100, and 70 features, while the decoder consists of corresponding layers with 70, 100, 50, and 25 features. The general network structure is shown in Fig. 1.
Latent vector constraints
In practice, such a VAE would be used to learn the cardiac and respiratory latent vectors but enforce “known” (fixed) latent vectors for sequence timings3. We investigated two key questions:
1. How much prior knowledge should be incorporated into the design of the fixed sequence timing latent vectors—timings only, or also the physics of T1/T2 relaxation?
2. The preferred shape of cardiac latent vectors—a cardiac phase representation with discontinues across the R-wave or as quasiharmonic components?
To answer these questions, we enforced hard constraints within the encoder’s architecture to produce four latent dimensions representing T1/T2 inversion recovery, cardiac, and respiratory motion states in 16 combinations of forms to determine which latent space representation could best encode the input signal. The combinations were drawn from:
T1/T2 representations
a) A baseline of linear timing diagrams, representing knowledge about sequence timing, but not about the nature of T1/T2 recovery; versus
b) Nonlinear T1/T2 relaxation representation, incorporating physics knowledge based on typical myocardial T1/T2 values: $$$\mu_1\ =\ 1-2e^{-T_I(\frac{1}{T_1} - \frac{ln cos \alpha}{T_R})}$$$ and $$$\mu_2 = e^{-\tau/T_2}$$$
Cardiac representations
a) A baseline of a linear timing diagram with no boundary conditions (cardiac phases from 1-20 with no continuity across the R-wave)
b) Either sine or cosine representations, reflecting circular boundary conditions of cardiac motion but simplifying diastolic function as a time-reversal of systolic motion
c)Two latent vectors, one sine and one cosine, as a harmonic model of real and imaginary parts of a complex exponential
Respiratory representation
Respiratory representation was always chosen to be respiratory position/amplitude
These various signal representations are shown in Fig. 2. We compared the VAE networks with 16 different hard constraint combinations by evaluating their L2 reconstruction loss. Each network was trained with 100 epochs.
Results
The results of the network performance are displayed in Fig. 3. The results show that enhancing T1/T2 inversion recovery signals with nonlinearities enhances network performance. Among the 16 evaluated representations, the one incorporating nonlinear T1 and T2 inversion recovery along with phase cardiac signals demonstrates the best performance. No improvement was observed by modifying the cardiac phase signal into sinusoidal curves.Discussion and conclusions:
The results suggest that it is useful to include some physics knowledge in the design of fixed T1/T2 relaxation latent vectors, but that it is not necessary to promote quasiperiodicity or circular boundary conditions of cardiac motion. Future work will focus on using the knowledge gained on effective latent space representations to remove hard constraints on respiratory and cardiac latent vectors, aiding in the design of statistical constraints to push latent vectors towards cardiac phase representation; nonlinear T1/T2 latent vectors will be retained.If a latent space can be successfully learned, this not only presents an opportunity for better cardiac/respiratory binning, but also for generating unseen motion states for subspace calculation, and for moving towards multidimensional quantitative CMR with continuous independent variables rather than discrete motion bins.
Acknowledgements
This work was partially supported by NIH R01 EB028146References
1. Christodoulou AG, Shaw JL, Nguyen C, et al. Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging. Nat Biomed Eng. 2018;2(4):215-226. doi:10.1038/s41551-018-0217-y
2. Hoppe E, Wetzl J, Yoon SS, et al. Deep Learning-Based ECG-Free Cardiac Navigation for Multi-Dimensional and Motion-Resolved Continuous Magnetic Resonance Imaging. IEEE Trans Med Imaging. 2021;40(8):2105-2117. doi:10.1109/TMI.2021.3073091
3. Zou Q, Priya S, Nagpal P, Jacob M. Joint Cardiac T1 Mapping and Cardiac Cine Using Manifold Modeling. Bioengineering. 2023;10(3):345. doi:10.3390/bioengineering10030345
Figures

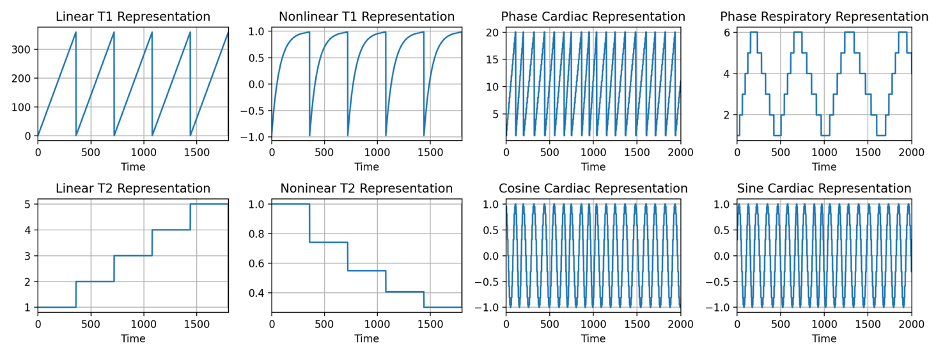

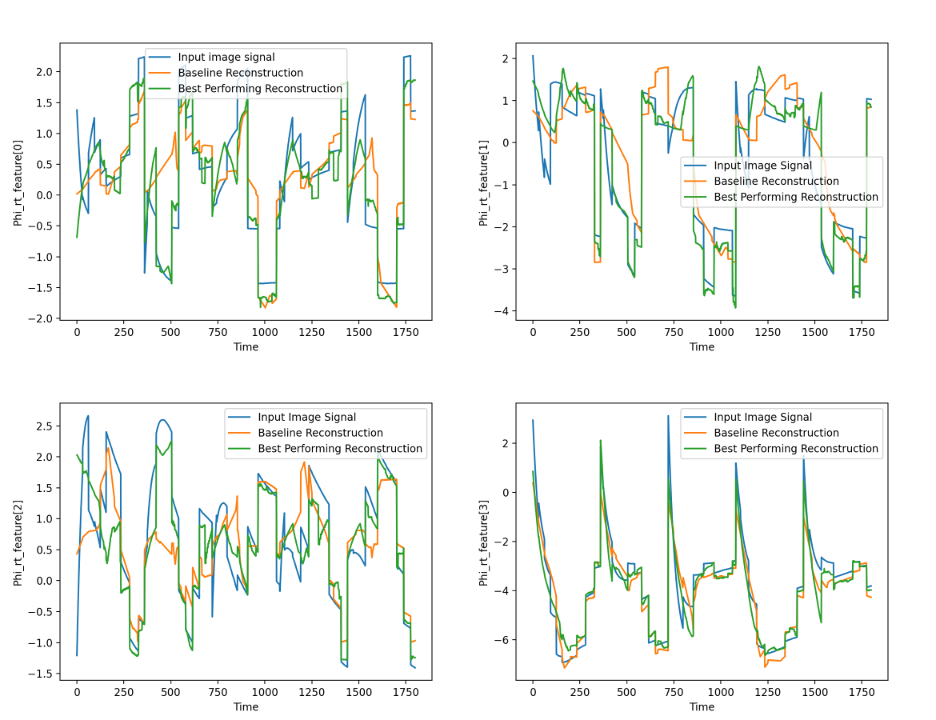
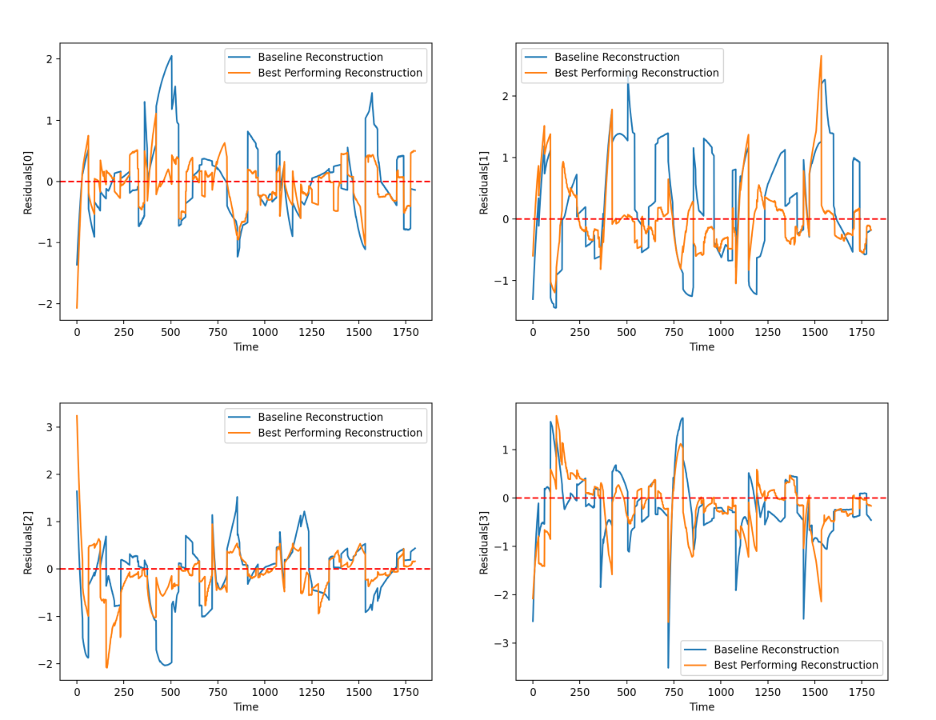
Figure 5. Error residuals of the first 4 reconstructed principal components of the self-gating data. The model for baseline reconstruction is linear T1/T2 representation andcardiac phase representation. The model with the best performing reconstruction is with nonlinear T1/T2 representation and cardiac phase representation.