4324
Predicting Preoperative Pathologic Grades of Bladder Cancer Using Intravoxel Incoherent Motion and Amide Proton Transfer-Weighted Imaging1Qilu Hospital of Shandong University, Jinan city, Shandong province, China, 2GE Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: Urogenital, Bladder, Intravoxel Incoherent Motion, Amide Proton Transfer-Weighted Imaging, Bladder Cancer Grading
Motivation: Preoperative grading of bladder cancer (BC) impacts the choice of operative modality and prognosis of patients.
Goal(s): We aimed to perform an accurate and non-invasive preoperative grading method for BC by MRI sequences.
Approach: IVIM as well as APTw imaging were included in this study.
Results: The IVIM-related parameter (D, true-diffusion-coefficient) and APTw values were significantly different in low- and high-grade BC. Robust diagnostic efficacies were separately confirmed with high AUCs for IVIM and APTw in BC grading, and the diagnostic efficacy of the combined IVIM and APTw model was significantly higher compared to the individual parameters on their own.
Impact: Our findings suggest a complementary effect between the IVIM and APTw imaging parameters The combined model shows promise as a noninvasive biomarker for predicting BC histologic grading, aiding in the development of clinical therapeutic strategies, and assessing prognosis.
INTRODUCTION
The tumor grades of bladder cancer (BC) are primarily associated with its clinical treatment and prognosis1,2. Therefore, accurately diagnosing the histological grade of BC in the clinic is essential.IVIM offers a comprehensive view of tumor microphenomenon and allows differentiation between capillary microcirculation and water molecule diffusion in living tissues3. Amide proton transfer-weighted (APTw) imaging reflects the concentration and pH of endogenous free proteins or peptides in tissues by monitoring the rate of exchange of amide protons with water protons4. Several previous studies have separately used IVIM or APTw in evaluating the diagnostic values in grading BC5,6. Although good results were obtained, distinctive physiological and pathological features of BC, including tumor cellularity, heterogeneity, and perfusion, cannot be comprehensively evaluated with either single technique. Many studies have demonstrated the benefit of the combination of the two techniques, IVIM and APTw, in tumors such as hepatocellular carcinoma, rectal adenocarcinoma, and endometrial cancer, there are no studies related to the preoperative application of APTw in combination with IVIM for predicting the BC grading7,8,9.
Therefore, this study aimed to investigate the predictive effectiveness of APTw imaging in conjunction with IVIM for BC grading before surgery.
METHODS
Subjects69 patients with suspected BC were consecutively enrolled in the trial. Certain exclusion criteria were defined as follows: (1) chemotherapy performed before MRI examination (2) lesion smaller than 5 mm (3) patient motion or inadequate image quality.
MRI acquisition
MRI examination was conducted using a 3.0T-MR system (Discovery 750w, GE Healthcare, USA) with a 16-channel coil.
For IVIM, a single shot spin-echo echo-planar imaging sequence was applied in axial view with 11 b-values (0, 10, 25, 50, 75, 100, 150, 200, 400, 800, and 1000s/mm2). TR/TE,4000/80.4ms; field-of-view, 320×320mm2; matrix, 128×128; slice thickness, 4mm; scan time, 2mins 46s.
For APTw imaging, a two-dimensional spin-echo echo-planar imaging sequence was performed on the largest slice of lesion. A saturation pulse with an amplitude of 2.0 μT and saturation duration of 2 s was applied. TR/TE,4806/35.6ms; field-of-view, 220×220mm2; matrix, 128×128; slice thickness, 4mm; scan time, 3mins 27s.
Data analysis
All original IVIM and APTw imaging datasets have been relocated to the GE ADW4.6 workstation. The ROIs were manually delineated on the biggest cross-section of the tumor on T2WI and autonomously duplicated to the IVIM and APTw pseudo-color maps via the workstation to measure the D, perfusion related pseudo-diffusion coefficient (D*), perfusion fraction (f), and APTw values. All parameter values of the ROIs were manually delineated three times on one slice and averaged for subsequent assessment.
SPSS 26.0 statistic software was used for statistical analyses. The intraclass correlation coefficients (ICCs) was used to access the interobserver agreement9. The independent samples t-test and Mann-Whitney U test were applied to compare quantitative variables between the two groups. The receiver operator characteristic (ROC) curve was conducted to evaluate the predictive performances of different parameters and the Delong test was implemented to compare the area under the curve (AUC) for each of the meaningful parameters and their combinations. P < 0.05 was deemed statistically significant.
RESULTS
In total, 19 low-grade and 50 high-grade patients were included for data analysis.Excellent inter-observer agreements of MRI parameter measurements were confirmed by high ICCs, ranging between 0.80 and 0.88.
ADC and D values of low-grade BC were significantly higher than those of high-grade BC ([1.42 ± 0.20 ×10-3 mm2/s] vs. [1.09 ± 0.25 ×10-3 mm2/s] and [1.24 ± 0.24×10-3 mm2/s] vs. [0.89 ± 0.18 ×10-3 mm2/s], respectively; all P < 0.001). Opposite patterns were found for APTw ( [1.53 ± 0.42]% vs. [2.38 ± 0.71]%, P <0.001) (Figure 1-3). The ROC curves indicated that the combination of D and APTw values could distinguish low- from high-grades of BC with the highest predictive efficacy (AUC = 0.96), as well as a significant difference compared to those by ADC, D, and APTw values separately(AUC = 0.84, 0.88, 0.85, respectively; all P < 0.05) (Figure 4-5).
DISCUSSION
Our results demonstrated that the parameters (ADC, D, APTw) were significantly different in BC with different grades. This may be due to high-grade BC with higher tumor cell densities than low-grade tumors, which impede the movement of water molecules, leading to decreased ADC and D values. In addition, the APTw values were higher in high-grade BC due to more active mitoses and the synthesis of more mobile proteins and peptides11,12,13.CONCLUSION
IVIM combined with APTw imaging significantly improved the predictive efficacy of assessing low-and high-grade BC compared to the individual parameters on their own.Acknowledgements
No acknowledgement found.References
1 Flaig T W, Spiess P E, Agarwal N, et al. NCCN Guidelines Insights: Bladder Cancer, Version 5.2018[J]. J Natl Compr Canc Netw, 2018, 16(9): 1041-1053.
2 Flaig T W, Spiess P E, Agarwal N, et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology[J]. J Natl Compr Canc Netw, 2020, 18(3): 329-354.
3 Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders[J]. Radiology, 1986, 161(2): 401-7.
4 Ray K J, Simard M A, Larkin J R, et al. Tumor pH and Protein Concentration Contribute to the Signal of Amide Proton Transfer Magnetic Resonance Imaging[J]. Cancer Res, 2019, 79(7): 1343-1352.
5 Wang F, Wu L M, Hua X L, et al. Intravoxel incoherent motion diffusion-weighted imaging in assessing bladder cancer invasiveness and cell proliferation[J]. J Magn Reson Imaging, 2018, 47(4): 1054-1060.
6 Wang H J, Cai Q, Huang Y P, et al. Amide Proton Transfer-weighted MRI in Predicting Histologic Grade of Bladder Cancer[J]. Radiology, 2022, 305(1): 127-134.
7 Jia F, Wu B, Yan R, et al. Prediction Model for Intermediate-Stage Hepatocellular Carcinoma Response to Transarterial Chemoembolization[J]. J Magn Reson Imaging, 2020, 52(6): 1657-1667.
8 Li J, Lin L, Gao X, et al. Amide Proton Transfer Weighted and Intravoxel Incoherent Motion Imaging in Evaluation of Prognostic Factors for Rectal Adenocarcinoma[J]. Front Oncol, 2021, 11: 783544.
9. Lin Y, Luo X, Yu L, et al. Amide proton transfer-weighted MRI for predicting histological grade of hepatocellular carcinoma: comparison with diffusion-weighted imaging[J]. Quant Imaging Med Surg, 2019, 9(10): 1641-1651.
10 Ma C, Tian S, Song Q, et al. Amide Proton Transfer-Weighted Imaging Combined With Intravoxel Incoherent Motion for Evaluating Microsatellite Instability in Endometrial Cancer[J]. J Magn Reson Imaging, 2023, 57(2): 493-505.
11 Takeuchi M, Sasaki S, Ito M, et al. Urinary bladder cancer: diffusion-weighted MR imaging--accuracy for diagnosing T stage and estimating histologic grade[J]. Radiology, 2009, 251(1): 112-21.
12 Geng Z, Zhang Y, Yin S, et al. Preoperatively Grading Rectal Cancer with the Combination of Intravoxel Incoherent Motions Imaging and Diffusion Kurtosis Imaging[J]. Contrast Media Mol Imaging, 2020, 2020: 2164509.
13 Meng N, Wang X, Sun J, et al. Application of the amide proton transfer-weighted imaging and diffusion kurtosis imaging in the study of cervical cancer[J]. Eur Radiol, 2020, 30(10): 5758-5767.
Figures
FIGURE 1: The scatter plot with bar chart for ADC (a), D (b), D* (c), f (d), and APTw (e) values in low- and high-grade BC.
There were significant differences in ADC, D, and APTw values between low- and high-grade BC (***P < 0.001). There were no significant differences in D* and f values between low- and high-grade BC (ns, not significant).
BC = bladder cancer; ADC = apparent diffusion coefficient; D = true diffusion coefficient; D* = perfusion-related pseudo-diffusion coefficient; f = perfusion fraction; APTw = amide proton transfer-weighted imaging.
FIGURE 2: An 81-year-old man with pathologically confirmed low-grade bladder cancer.
(a) axial T2-weighted image, (b) diffusion-weighted image (b = 1000 mm2/s ), and (c-g) corresponding parametric maps (ADC, D, D*, f, APTw, and T2WI fused image, respectively) showed the ROI placement, respectively. Tumor values were 1.23×10-3 mm2 /s, 1.26×10-3 mm2 /s, 13.8×10-3 mm2 /s, 20.15%, and 1.57%, respectively; (h) pathological image (HE, ×200).
FIGURE 3: A 66-year-old man with pathologically confirmed high-grade bladder cancer.
(a) axial T2-weighted image, (b) diffusion-weighted image (b = 1000 mm2/s ), and (c-g) corresponding parametric maps (ADC, D, D*, f, APTw and T2WI fused image, respectively) showed the ROI placement, respectively. Tumor values were 0.78×10-3 mm2 /s, 0.62×10-3 mm2 /s, 18.2×10-3 mm2 /s, 16.11%, and 2.27%, respectively; (h) pathological image (HE, ×200).
FIGURE 4: ROC curve analysis of the performance of DWI, IVIM, and APTw to evaluate the grade of BC.
D+APTw represents the combination of D and APTw imaging.
a indicated the comparison with statistical significance.
AUC = area under the curve; ADC = apparent diffusion coefficient; D = true diffusion coefficient; D* = perfusion-related pseudo-diffusion coefficient; f = perfusion fraction; APTw = amide proton transfer-weighted imaging; a.u., arbitrary unit; NA, not available.
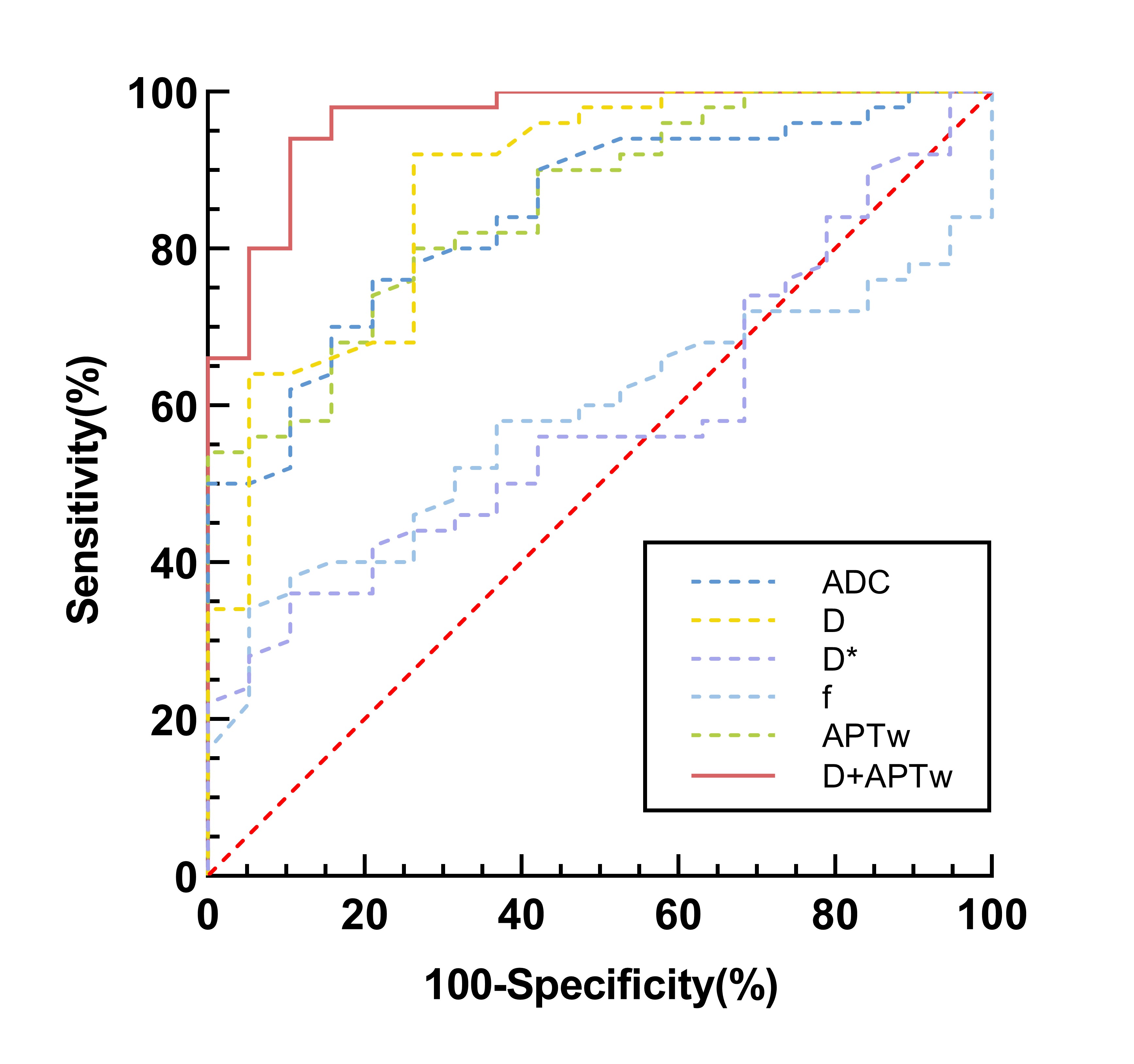
FIGURE 5: Receiver operating characteristic curves of each imaging parameter for discrimination between low- and high-grade BC.
AUCs of ADC value, D value, D* value, f value, APTw value and D + APTw were 0.844 (0.736 - 0.920), 0.878 (0.777 - 0.944), 0.538 (0.458 - 0.700), 0.579 (0.454 - 0.697), 0.853 (0.747 - 0.927), 0.964 (0.889 - 0.994), respectively.
BC, bladder cancer; ADC, apparent diffusion coefficient; D, true diffusion coefficient; D*, perfusion-related pseudo-diffusion coefficient; f, perfusion fraction; APTw, amide proton transfer-weighted imaging.