4321
Optimisation and implementation of high b-value DWI using 200mT/m gradient system for clinical prostate MRI.1Clinical and Research Imaging Centre, South Australian Health and Medical Research Institute, Adelaide, Australia, 2Jones Radiology, Adelaide, Australia, 3Siemens Healthineers Pty Ltd, Adelaide, Australia
Synopsis
Keywords: Prostate, Prostate, Diffusion
Motivation: Diffusion-weighted imaging is critical to the diagnosis of prostate cancer but can be limited by noise. A commercially available 200mT/m gradient system may allow revisiting of higher b-value DWI.
Goal(s): To optimise a feasible high b-value prostate MR protocol for clinical use.
Approach: Phantom, simulation and in vivo iterative optimisation were evaluated against technical metrics and novel discrete choice experimental design for radiologist preference.
Results: Radiologist DWI preference is weighted by signal-to-noise. Emerging high gradient performance and deep learning reconstruction can reduced decline in SNR potentiating a signal-optimised high b-value protocol for clinical prostate cancer imaging within feasible scan times.
Impact: Signal-optimised high b-value DWI for prostate cancer using a 200mT/m gradient 3T MRI system may be clinically feasible and supports a scalable trial of its diagnostic impact.
Introduction
Diffusion-weighted MRI is critical to the diagnosis of prostate cancer with hyperintensity at high b values and hypointensity on apparent diffusion coefficient (ADC) images being a validated imaging marker for clinically significant prostate cancer. A b-value of 1600s/mm2 has previously been defined as optimal at 3T with endorectal coil, a minimum of 1400s/mm2 recommended in PI-RADSv2.1 and values up to 2000 or higher considered advantageous1. However optimising pelvic DWI contrast needs to balance signal and artefacts with typical b-values in clinical practice ranging from 800-1200s/mm2. Emerging MRI systems with high performance gradient systems for body imaging may allow revisiting of higher b-value diffusion particularly in conjunction with developments in deep learning, complex averaging and Eddy current correction. This paper describes the initial experiences and optimisation of high b-value prostate MRI using a clinically available system.Methods
Healthy volunteer cohort (no history of prostate disease, normal PSA) DWI images were obtained on a 3T MAGNETOM Cima.X (Siemens Healthineers, Erlangen, Germany) capable of 200mT/m gradients at slew rate of 200T/m/s. Slice thicknesses of 2mm, 3mm and 5mm were used with nine acquired b-values in 250s/mm2 increments from 1000s/mm2 to 3000s/mm2 and calculated b-values to 4000s/mm2, vendor selective field-of-view excitation, complex averaging and deep learning reconstruction. Prostate signal-to-noise (SNR) was measured as the absolute signal difference between peripheral zone and obturator internus muscle divided by the standard deviation of obturator internus, with muscle chosen as the reference given the impact on background tissue suppression. Geometric distortion was calculated from the spatial overlap of manually segmented DWI images. Image analysis was performed in Osirix (Pixmeo, Switzerland) and calculations in Matlab (Mathworks, CA). 156 randomly assigned image pairs (DWI, ADC or both) at mid prostate slice from differing protocols were generated and sampled for a discrete choice experiment (axes resolution, b-value, noise) where 3 experienced prostate radiologists chose between paired images in a method adapted from research on patient healthcare preferences2. Preference weight for a choice among a sets of alternatives can be used to quantify the impact of underlying attribute levels. Using 5-point Likert scale, the same radiologists also graded images individually for overall quality, noise, artefacts, sharpness.Results
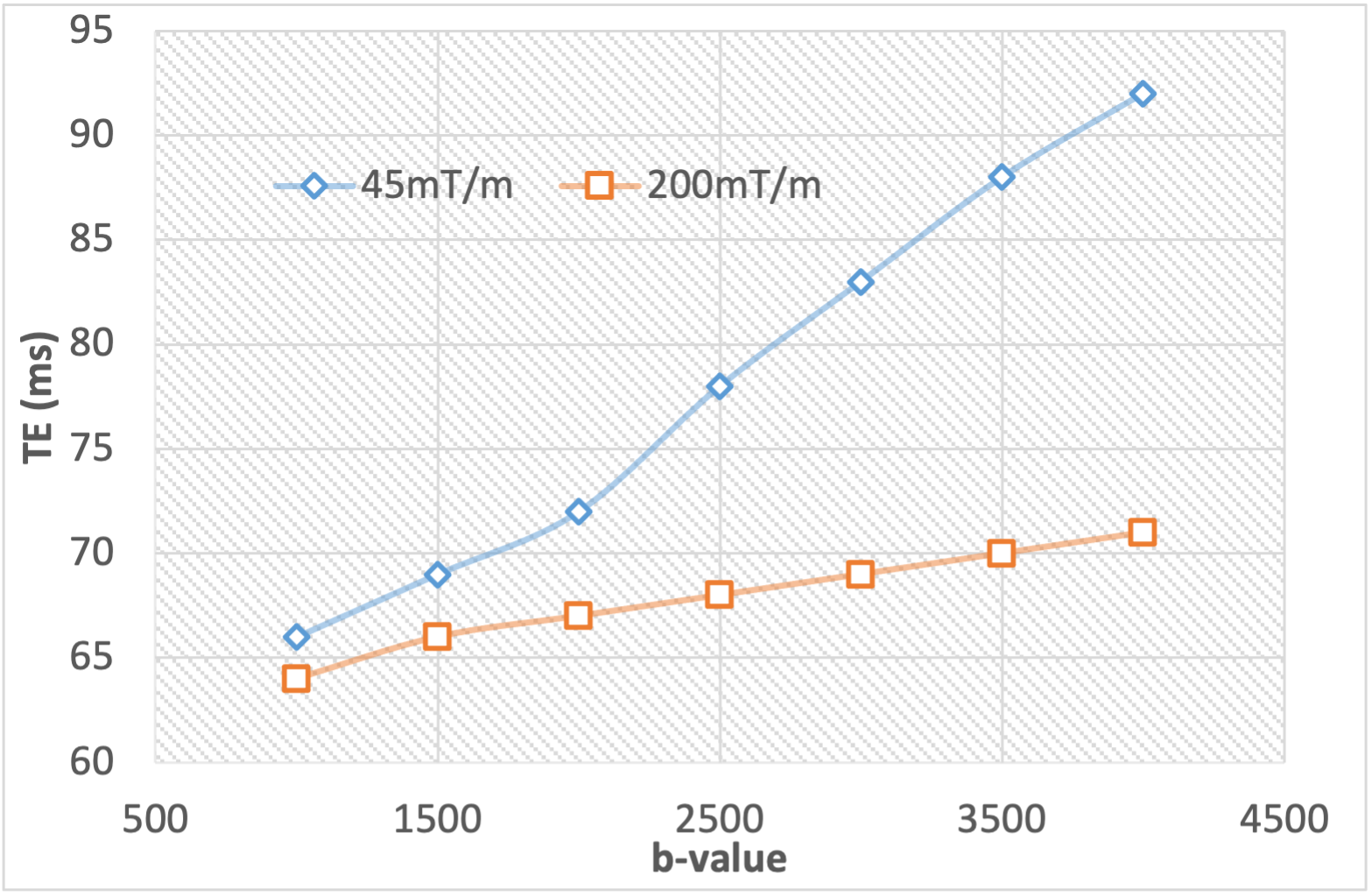
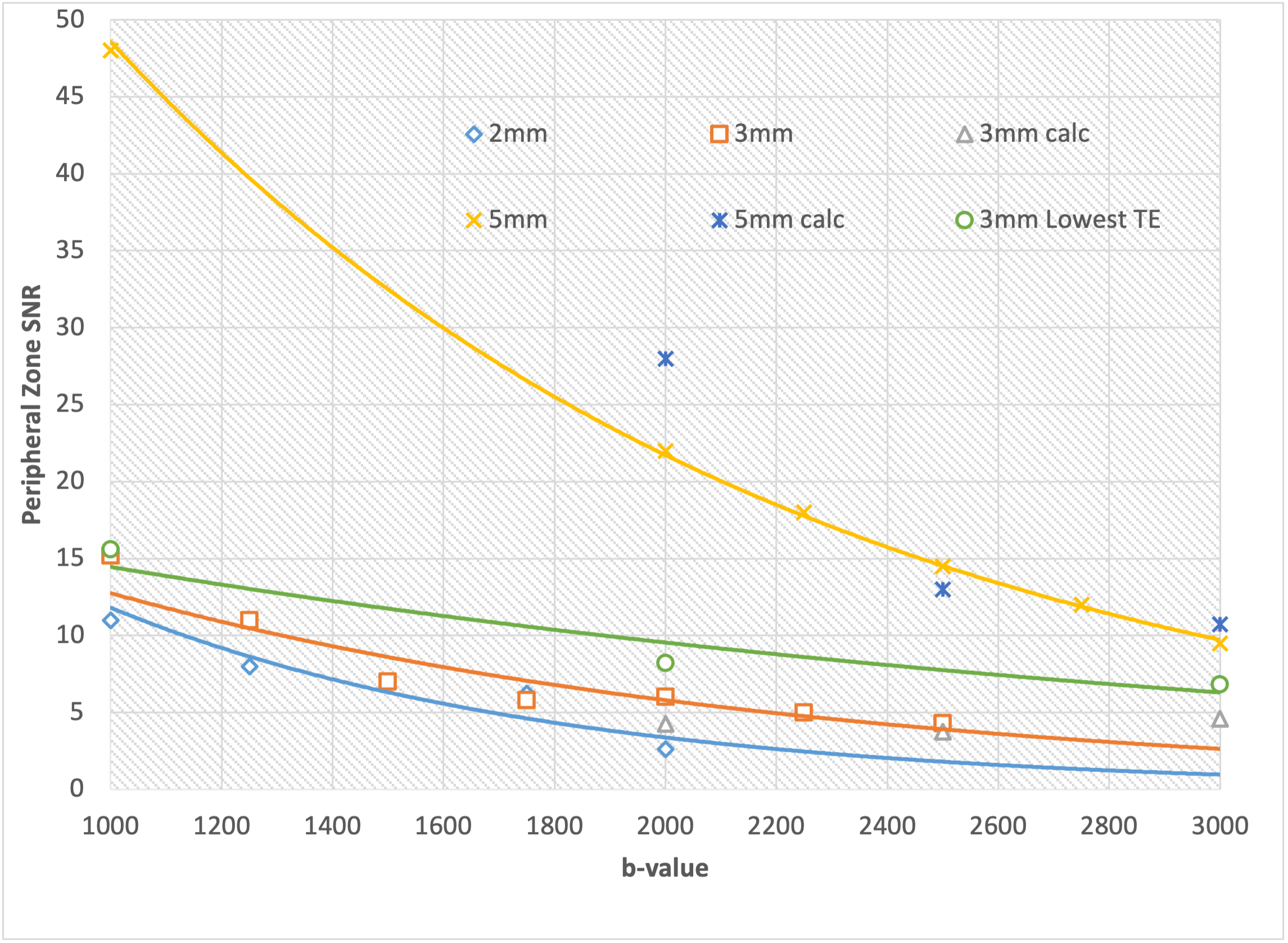
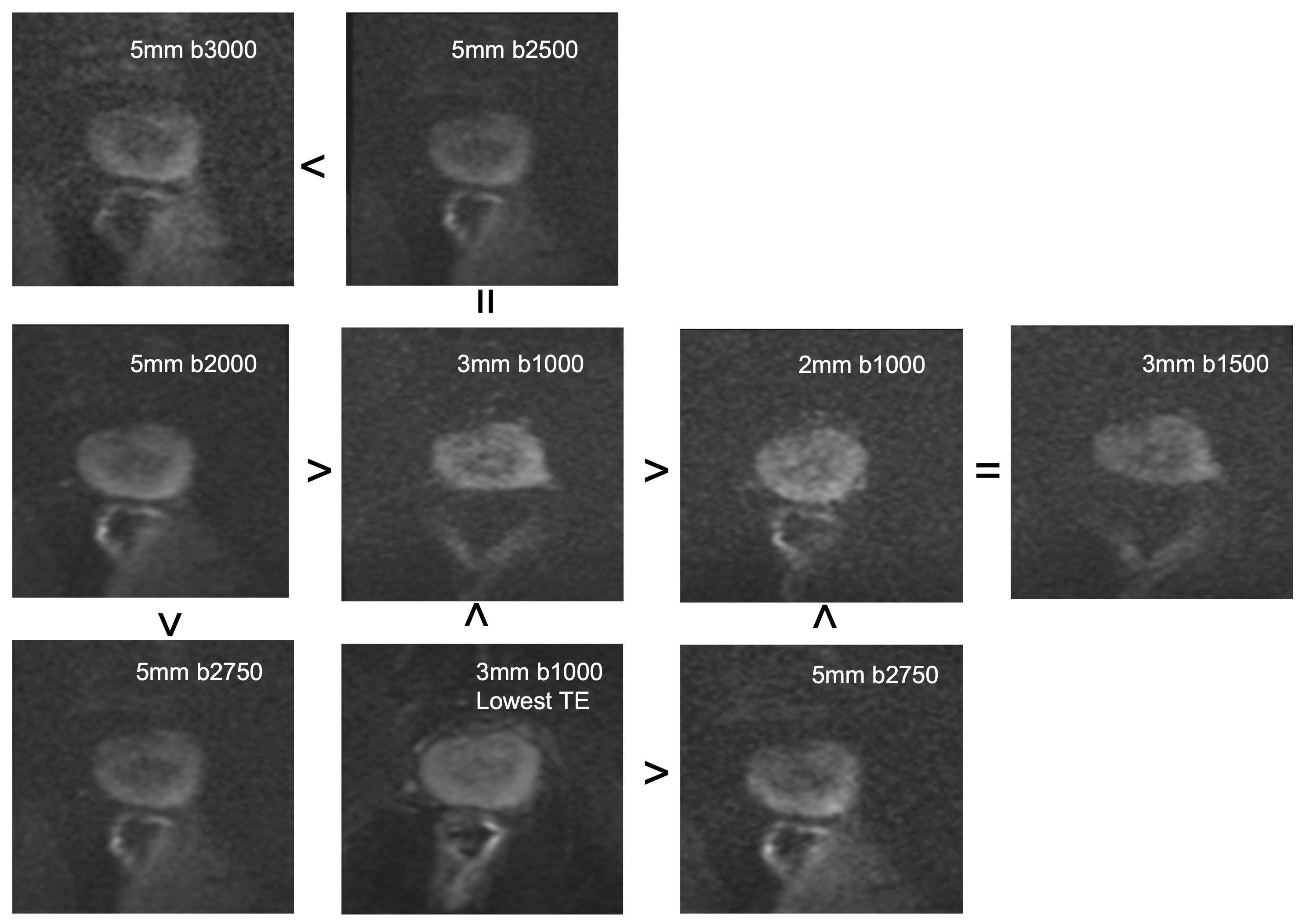
From phantom experiments, deep learning and complex averaging methods contributed 26% and 2% incremental gain in signal respectively at b2000. 200mT/m gradient performance allowed reduction in minimum TE particularly at higher b-values compared to simulation from 45mT/m system (Figure 1). As expected, prostate SNR reduced at higher b-values despite background suppression. Images up to b3000 with comparable SNR to standard b1250 were possible in clinically achievable scan time but highest b-value benefited from increase in slice thickness (Figure 2). Representative images from decision tree and direction of radiologist choice is shown in Figure 3. Preference weight was balanced between attributes provided noise was graded not more than 4/5 (having little or no impact) with trend towards slightly thicker slices (likely to achieve SNR), towards higher b-values and towards higher SNR. Once noise increased, it was the dominant factor other than a case with non-diagnostic artefact. It suggests an SNR floor for image acceptance. Agreement between radiologists was fair (Krippendorf's alpha 0.67). Calculated peripheral zone ADC value was strongly influenced by the upper b-value, almost 50% lower from b1000 to b3000. Homogeneity of ADC images reflected in reducing standard deviation also increased at higher b-values. Geometric distortion was not significantly increased with DICE similarity coefficients using b1000 as reference of 0.974 and 0.963 at b2000 and b3000 respectively (Figure 4).Discussion
The importance of SNR on radiologist preference in pelvic DWI portends challenges in high b-value acquisitions which are inherently noisier and may explain the common use of below recommended values in clinical practice. Deep learning reconstruction methods and gradient performance to minimise TE can reduce decline in SNR. This provides an opportunity to revisit the role of higher b-values in prostate cancer diagnosis but compromises are still required in the acquisition. A framework such as ours with optimisation guided by SNR can support deployment of an advanced higher b-value diffusion protocol for clinical research. Dependence of calculated ADC on b-value will require adaptive thresholds if used for quantitative imaging but the increased homogeneity in ADC of normal prostate tissue may also improve hypointense lesion detection. Initial results from implementation in a clinical cohort will be presented.Conclusion
Emerging high-performance diffusion gradients and reconstruction methods for pelvic imaging may challenge existing norms and allow new approaches to higher b-value imaging in clinical practice. Ongoing research such as this is needed to assess the impact on diagnostic accuracy and clinical outcomes.Acknowledgements
The authors acknowledge the support of the National Imaging Facility, a National Collaborative Research Infrastructure Strategy (NCRIS) capability of Australia.References
1. PI-RADS Steering Committee. American College of Radiology. https://www.acr.org/-/media/ACR/Files/RADS/Pi-RADS/PIRADS-v2-1.pdf
2. Hauber B et al. Statistical Methods for the Analysis of Discrete Choice Experiments: A Report of the ISPOR Conjoint Analysis Good Research Practices Task Force,Value in Health,19:4, 2016.
Figures