4317
Improved Visualization and Staging of Upper Tract Urothelial Carcinoma Using Coronal Reduced Field-of-View Diffusion Weighted Imaging1Peking University First Hospital, Beijing, China, 2MR Collaboration, United Imaging Research Institute of Intelligent Imaging, Beijing, China
Synopsis
Keywords: Urogenital, Urogenital
Motivation: Conventional axial full-field-of-view (fFOV) DWI poorly demonstrates upper tract urothelial carcinoma (UTUC) due to its varying morphology and anatomical position. The additional coronal reduced field-of-view (rFOV) DWI may improve evaluation.
Goal(s): The objective of this study was to assess the diagnostic value and image quality of coronal rFOV DWI in the evaluation of UTUC.
Approach: This study compared the image quality, tumor contrast, ADC value, and staging accuracy between coronal rFOV DWI and axial fFOV DWI in UTUC.
Results: Coronal rFOV DWI provided better image quality and higher tumor contrast than fFOV DWI. It provided additional diagnostic value in the staging of UTUC.
Impact: This study validates the clinical application of reduced field-of-view DWI in the assessment of upper tract urothelial carcinoma. The use of this technique improves image quality and tumor conspicuity in the coronal plane, providing additional value for diagnosis and staging.
Introduction
Upper tract urothelial carcinoma (UTUC) can present with diverse morphological features with its elongated axis predominantly in the coronal orientation, which may not be well visualized on conventional axial diffusion weighted imaging (DWI). Coronal reduced field-of-view (rFOV) DWI offers better visualization of the upper urothelial tract in its long axis and may provide higher image quality and resolution than full field-of-view (fFOV) DWI[1–3]. The aim of this study was to comprehensively assess the additional benefits of using coronal rFOV DWI in the visualization and evaluation of UTUC.Methods
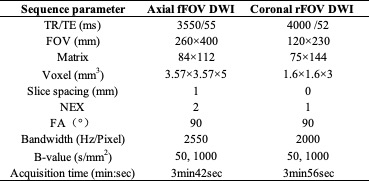
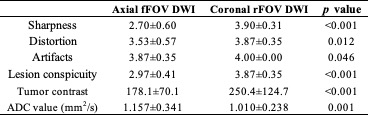
Thirty patients (14 female, median age: 70 years) with pathologically proven UTUC were retrospectively included. They underwent preoperative MR urography with two types of DWI: axial fFOV DWI and coronal rFOV DWI on a 3.0T MRI scanner (uMR 790, United Imaging Healthcare, Shanghai, China). Detailed imaging protocols are listed in Table 1. The corresponding ADC maps were automatically generated.For qualitative analysis, two experienced radiologists independently evaluated image quality parameters for both DWIs, including image sharpness (1 = poor, 2 = fair, 3 = good, 4 = excellent), distortion (1 = severe, 2 = moderate, 3 = slight, 4 = no), artifacts (1 = severe, interfere the diagnosis, 2 = severe, partially interfere the diagnosis, 3 = slight, no interfere the diagnosis, 4 = no artifacts), and lesion conspicuity (1 = poor, outline unrecognized, 2 = fair, most of the outlines unclear, 3 = good, small part of outline unclear, 4 = excellent, clear outline)[1].
For quantitative analysis, the mean signal intensities (SIs) of the tumor and adjacent fat were measured by manually drawn regions of interest (ROIs) on both DWIs. The tumor contrast was defined as the SI difference between the tumor and adjacent fat. The ROI of the tumor was copied to the ADC map to obtain ADC values. Two readers used two DWIs to stage tumors as either T1-2 or T3-4, based on whether the tumor invaded adjacent fat or renal parenchyma[4]. They also subjectively assessed the added value of coronal rFOV to conventional fFOV DWI for diagnosing and staging UTUC. The pathological results from radical nephroureterectomy were used as the reference standard for diagnosing and staging UTUC.
Results
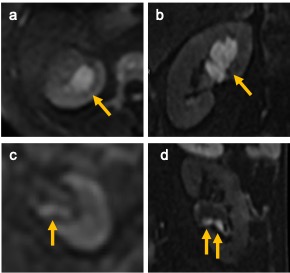
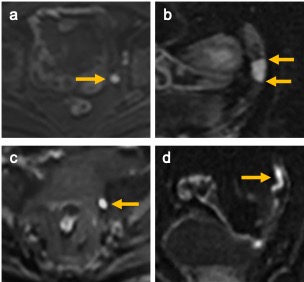
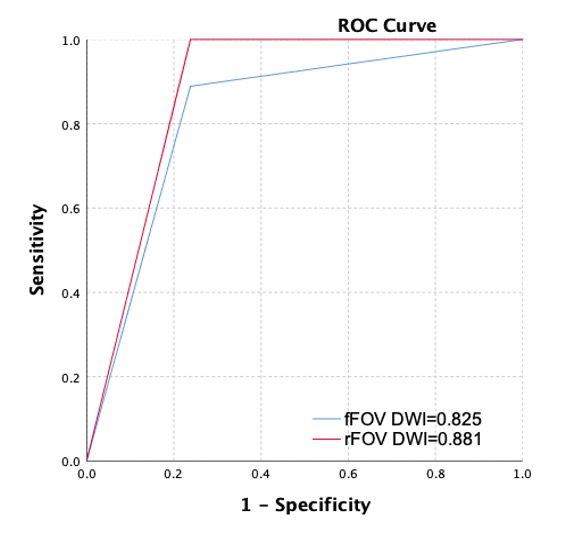
Fifteen lesions were in the renal calyces and/or pelvis, while the other 15 were in the ureters. Nine lesions had pathological T3-4 stage. The image quality of rFOV DWI was rated superior to that of fFOV DWI (Table 2, p<0.05). Representative cases are shown in Figures 1 and 2. The ADC value of fFOV DWI was significantly lower than that of rFOV DWI (1.010±0.238 mm2/s, 1.157±0.341 mm2/s, p=0.001). The tumor contrast of rFOV DWI was significantly higher than that of fFOV DWI (250.4±124.7, 178.1±70.1, p<0.001).The area under the curve value for determining the UTUC stage was 0.825 for fFOV DWI and 0.881 for rFOV DWI, but there was no statistically significant difference between them (Figure 2). The sensitivity and accuracy of rFOV DWI were higher than those of fFOV DWI (100% and 83.3% vs. 88.9% and 80%, respectively). The two readers preferred to add coronal rFOV DWI to conventional fFOV DWI in the diagnosis and staging of UTUC for most of the cases (29 and 27 cases, respectively).
Discussion
Our study showed that coronal rFOV DWI offered superior image quality, enhanced lesion conspicuity, and improved tumor contrast compared with fFOV DWI in the evaluation of UTUC. Coronal rFOV DWI excelled in delineating the extent of the tumor along its long-axis plane while maintaining exceptional image quality. For UTUC staging, the improved sensitivity and accuracy of rFOV DWI compared to fFOV DWI can be attributed to the more distinct visualization of tumor outlines and the higher tumor contrast achieved with rFOV DWI. Furthermore, the preference of both readers for a combination of coronal rFOV and fFOV DWI underscored the diagnostic value added by rFOV DWI to the conventional fFOV DWI in UTUC stage assessment. The ADC, derived from DWI, is associated with tumor malignancy, and UTUC demonstrates lower ADC values than normal tissue[5]. The ADC values from coronal rFOV DWI were significantly lower than those from fFOV DWI of the tumor, suggesting that the former may be potentially more accurate ADC values of UTUC. However, this issue is under debate[6].Conclusion
Coronal rFOV DWI showed significantly better image quality, lesion conspicuity, and tumor contrast than fFOV DWI in UTUC. The incorporation of coronal rFOV DWI to fFOV DWI may hold promise for improving UTUC staging and guiding clinical therapeutic strategies.Acknowledgements
None.References
[1] CHEN M, FENG C, WANG Q, et al. Comparison of Reduced Field-of-View Diffusion-Weighted Imaging (DWI) and Conventional DWI Techniques in the Assessment of Cervical Carcinoma at 3.0T: Image Quality and FIGO Staging[J/OL]. European Journal of Radiology, 2021, 137(1095): 109557. https://doi.org/10.1016/j.ejrad.2021.109557. DOI:10.1016/j.ejrad.2021.109557.
[2] INOUE A, TANABE M, IHARA K, et al. Evaluation of Diffusion-Weighted Magnetic Resonance Imaging of the Rectal Cancers: Comparison between Modified Reduced Field-of-View Single-Shot Echo-Planar Imaging with Tilted Two-Dimensional Radiofrequency Excitation Pulses and Conventional Full Field-O[J/OL]. Academic Radiology, 2022, 30(0123456789): 470–482. https://doi.org/10.1016/j.acra.2022.07.018. DOI:10.1007/s11547-023-01699-2.
[3] PENG Y, LI Z, TANG H, et al. Comparison of Reduced Field-of-View Diffusion-Weighted Imaging (DWI) and Conventional DWI Techniques in the Assessment of Rectal Carcinoma at 3.0T: Image Quality and Histological T Staging[J]. Journal of Magnetic Resonance Imaging, 2018, 47(4): 967–975. DOI:10.1002/jmri.25814.
[4] PANER G P, STADLER W M, HANSEL D E, et al. Updates in the Eighth Edition of the Tumor-Node-Metastasis Staging Classification for Urologic Cancers[J/OL]. European Urology, 2018, 73(4): 560–569. http://dx.doi.org/10.1016/j.eururo.2017.12.018. DOI:10.1016/j.eururo.2017.12.018.
[5] TSIKITAS L A, HOPSTONE M D, RAMAN A, et al. Imaging in Upper Tract Urothelial Carcinoma : A Review[J]. 2023.
[6] YANG T, LI Y, YE Z, et al. Diffusion Weighted Imaging of the Abdomen and Pelvis: Recent Technical Advances and Clinical Applications[J/OL]. Academic Radiology, 2023, 30(3): 470–482. https://doi.org/10.1016/j.acra.2022.07.018. DOI:10.1016/j.acra.2022.07.018.
Figures