4314
DWI for Improving Diagnostic Performance of Breast MRI: Impact of Alternate Apparent Diffusion Coefficient Quantitation and Cutoff Approaches1Radiology, University of Washington, Seattle, WA, United States, 2Clinical research Division, Fred Hutchison Cancer Center, Seattle, WA, United States, 3Department of Radiology, University of Washington, Seattle, WA, United States, 4Bioengineering, University of Washington, Seattle, WA, United States
Synopsis
Keywords: Breast, Screening, ADC, breast cancer, biopsy reduction
Motivation: Apparent Diffusion Coefficient (ADC) measures can help reduce false positives in breast MRI.
Goal(s): Explore different approaches for measuring lesion ADC that emphasize different aspects of tumor microenvironment and biology and their effect on reducing unnecessary biopsies.
Approach: Nine ADC measures were computed for each lesion using different b value combinations and segmentation techniques. Different approaches of selecting ADC threshold were explored to reduce unnecessary biopsies.
Results: Applying ADC cutoffs, the largest reduction of benign biopsies (~20%) was achieved using ADC0-800 mapping and the 2D lesion segmentation technique, with the hotspot ROI measurement providing very similar performance.
Impact: This study demonstrates that a variety of ADC measurement techniques can help reduce unnecessary biopsies of breast MRI, suggesting that the easiest approach of segmenting the darkest pixels in the lesion might facilitate integration of DWI into the clinical workflow.
Introduction
Dynamic contrast enhanced (DCE) MRI has the highest sensitivity for cancer detection among all breast imaging modalities but it suffers from moderate specificity resulting in many unnecessary biopsies. Diffusion weighted MRI (DWI) has emerged as a promising adjunct to DCE-MRI to reduce false positives[1,2]. The apparent diffusion coefficient (ADC) has demonstrated usefulness for distinguishing benign and malignant lesions. Approaches to measure lesion ADC values vary and emphasize different aspects of tumor microenvironment and biology. Choice of diffusion sensitization (or b-value) affects relative contributions from microcirculation and restriction, and region-of-interest (ROI) sampling methods capture different aspects of the lesion microstructure (e.g., whole volume versus ‘hotspot’)[3]. Here, we explored different approaches for measuring lesion ADC and potential effect on reducing false positives and unnecessary biopsies of breast MRI.Method
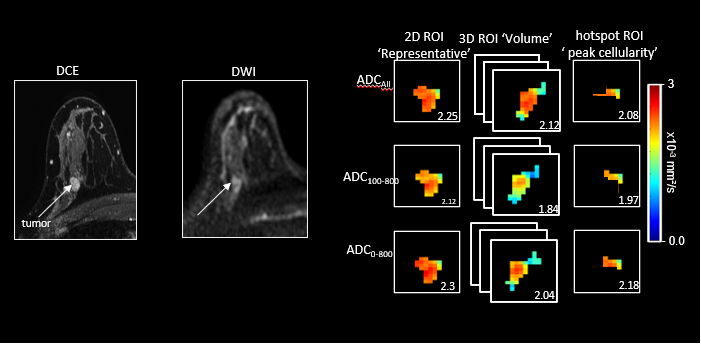
In this IRB-approved study, consecutive breast screening MRI examinations (August 2014 – Dec 2018) that had a suspicious BIRADS 4/5 breast lesion followed by definitive biopsy outcome were retrospectively evaluated.MRI was performed on a 3T scanner (Achieva, Philips Healthcare, Best, The Netherlands) using a clinical breast MRI protocol in accordance with ACR Accreditation guidelines. DWI was acquired with TR/TE=5043/67ms, resolution 1.8 mmx1.8mmx4mm, b=0/100/600/800 s/mm2, scan duration=4:53mins. Lesion ROIs were defined on b=800s/mm2 images using a semi-automated threshold-based tool to avoid fat and fibroglandular tissue in MATLAB (Mathworks, Nattick, MA). Nine total ADC measures were computed for each lesion using three methods for generating ADC maps and three segmentation techniques. ADC maps were generated using different b value combinations: b=0/800s/mm2(ADC0-800), b=100/800s/mm2(ADC100-800) and b =0/100/600/800s/mm2(ADCAll). Lesion ROIs were defined for a single representative slice (‘2D’), whole tumor volume (‘3D’) and darkest region with lowest ADC values (‘hotspot’) (Fig 1).
The Wilcoxon rank-sum test was used to compare benign and malignant ADC measures. Diagnostic performance was evaluated by calculating the area under the receiver operating characteristic curves (AUC) using R (v4.0.3).
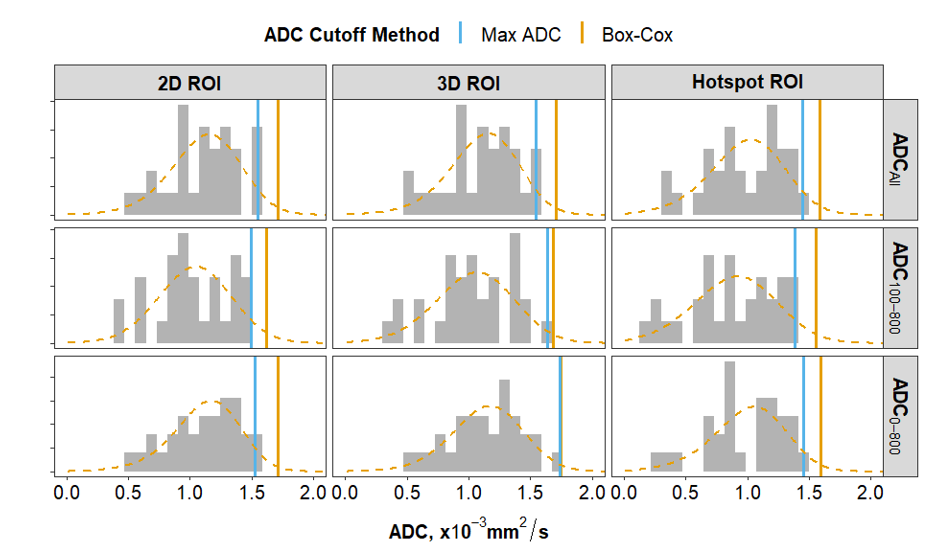
The highest ADC observed among malignant lesions was identified to determine an ADC threshold (Max-ADC cutoff) for each of the nine ADC techniques to reduce false positives while maintaining high sensitivity, as previously described[1]. The Max-ADC threshold by definition will achieve 100% sensitivity in the current sample but is very data and sample size dependent. Therefore, a potentially more generalizable ADC threshold was also estimated for each ADC measure using the Box-Cox transformation[4] (Box-Cox ADC cutoff). A threshold was calculated as mean + 1.96 x (standard deviation) after Box-Cox transformation of ADC values of malignant lesions to a normal distribution (~97.5% sensitivity in the population) and then inverse transformed to get the corresponding Box-Cox ADC cutoff.
The reduction in benign biopsies was calculated as a ratio of (#benign lesions with ADC > cutoff)/(total number of benign lesions).
Results
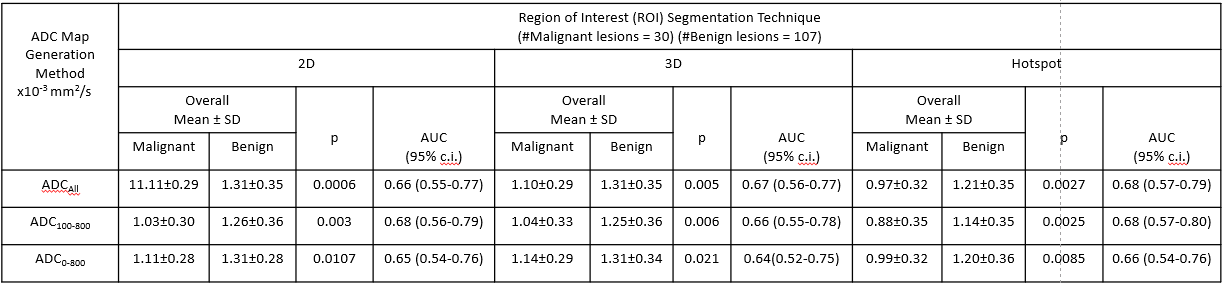
Over the study period, 137 suspicious lesions (in 121 women, median age 44 years [range, 20-75yrs]) were detected on DCE-MRI and recommended for biopsy. Of those, 30 (21.9 %) were malignant and 107 (78.1 %) were benign. Mean ADC values of benign lesions were significantly higher than malignancies in all nine measurement approaches. The AUC for predicting malignancy ranged from 0.64 (95% CI: 0.52-0.75) for 3D ADC0-800 to 0.68 (95% CI: 0.57-0.80) for hotspot ADC100-800 (Table 1). There were no statistically significant differences in AUC between the nine measurement approaches after accounting for multiple testing.ADC Threshold: The Max-ADC cutoff for each of the nine ADC generation method was lower than those obtained using the generalized Box-Cox ADC cutoff except for the 3D ADC0-800 technique. (Fig 2)
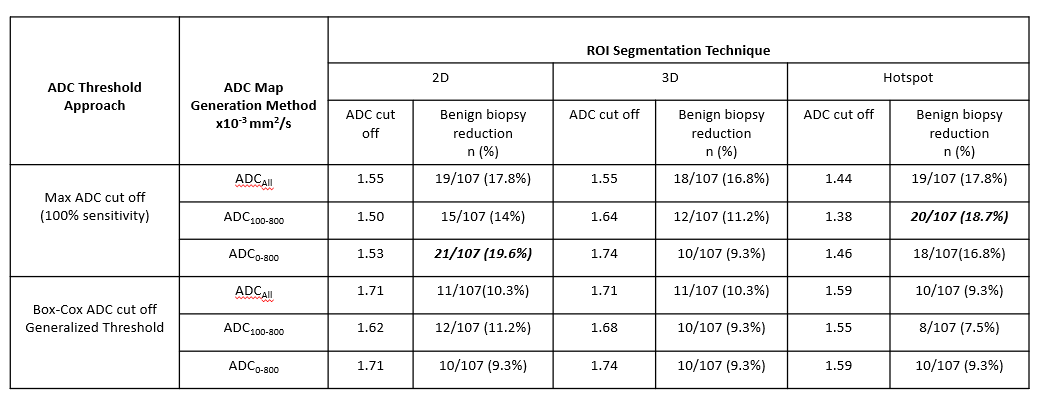
Diagnostic Performance: Applying the Max-ADC cutoff values resulted in a maximum reduction of benign biopsies of nearly 20% (21/107) using ADC0-800 and 2D (cutoff = 1.53x10-3 mm2/s). The other alternate ADC calculation techniques provided 9-18% reduction in benign biopsies. The higher, more generalized cutoffs estimated using Box-Cox ADC transformation showed a similar trend but with lower reduction (7.5-11%) in the number of unnecessary biopsies. (Table 2).
Discussion
Using the Max-ADC cutoff approach, mean ADC calculated with b values 0/800 s/mm2 using a 2D ROI had the highest benign biopsy reduction rate but differences were not significant. On the other hand, the higher generalized cutoffs might be more reliable for clinical implementation but would likely have a lower biopsy reduction rate. Our findings demonstrate that reduction in benign biopsies can be achieved using lesion ADC measurements computed from a variety of approaches. This supports that the easiest approach of segmenting the darkest pixels in the lesion similar to the hotspot technique (also suggested by EUSOBI consensus)[5] might facilitate integration of DW imaging into the clinical workflow.Acknowledgements
Supported by NIH/NCI research grant R01CA207290References
1. Rahbar H, Zhang Z, Chenevert TL, Romanoff J, Kitsch AE, Hanna LG, Harvey SM, Moy L, DeMartini WB, Dogan B, Yang WT, Wang LC, Joe BN, Oh KY, Neal CH, McDonald ES, Schnall MD, Lehman CD, Comstock CE, Partridge SC. Utility of Diffusion-weighted Imaging to Decrease Unnecessary Biopsies Prompted by Breast MRI: A Trial of the ECOG-ACRIN Cancer Research Group (A6702). Clin Cancer Res. 2019 Mar 15;25(6):1756-1765. doi: 10.1158/1078-0432.CCR-18-2967. Epub 2019 Jan 15. PMID: 30647080; PMCID: PMC6420847.
2. Partridge SC, Nissan N, Rahbar H, Kitsch AE, Sigmund EE. Diffusion-weighted breast MRI: Clinical applications and emerging techniques. J Magn Reson Imaging. 2017 Feb;45(2):337-355. doi: 10.1002/jmri.25479. Epub 2016 Sep 30. PMID: 27690173; PMCID: PMC5222835.
3. McDonald ES, Romanoff J, Rahbar H, Kitsch AE, Harvey SM, Whisenant JG, Yankeelov TE, Moy L, DeMartini WB, Dogan BE, Yang WT, Wang LC, Joe BN, Wilmes LJ, Hylton NM, Oh KY, Tudorica LA, Neal CH, Malyarenko DI, Comstock CE, Schnall MD, Chenevert TL, Partridge SC. Mean Apparent Diffusion Coefficient Is a Sufficient Conventional Diffusion-weighted MRI Metric to Improve Breast MRI Diagnostic Performance: Results from the ECOG-ACRIN Cancer Research Group A6702 Diffusion Imaging Trial. Radiology. 2021 Jan;298(1):60-70. doi: 10.1148/radiol.2020202465. Epub 2020 Nov 17. PMID: 33201788; PMCID: PMC7771995.
4. Partridge SC, Demartini WB, Kurland BF, Eby PR, White SW, Lehman CD. Differential diagnosis of mammographically and clinically occult breast lesions on diffusion-weighted MRI. J Magn Reson Imaging. 2010 Mar;31(3):562-70. doi: 10.1002/jmri.22078. PMID: 20187198.
5. Baltzer P, Mann RM, Iima M, Sigmund EE, Clauser P, Gilbert FJ, Martincich L, Partridge SC, Patterson A, Pinker K, Thibault F, Camps-Herrero J, Le Bihan D; EUSOBI international Breast Diffusion-Weighted Imaging working group. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol. 2020 Mar;30(3):1436-1450. doi: 10.1007/s00330-019-06510-3. Epub 2019 Nov 30. PMID: 31786616; PMCID: PMC7033067.
Figures