4313
Classification of MRI-only suspicious breast lesions: Development and validation of a nomogram combining MRI features and ADC-based histogram1Radiology, Department of Radiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, China, 2Department of Radiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, China, 3Clinical & Technical Support, Philips Healthcare, Beijing, China
Synopsis
Keywords: Breast, Breast, Magnetic resonance imaging; Nomogram; Diffusion-weighted imaging; Histogram analysis
Motivation: MRI-only lesions tend to be small in size and often have limited specific morphologic features on MRI, posing a significant diagnostic challenge for clinicians.
Goal(s): A simple, objective, and noninvasive approach is required to improve the diagnostic accuracy of MRI-only lesions.
Approach: We aimed to develop and validate a nomogram combining clinicoradiologic features and ADC-based histogram parameters for MRI-only suspicious lesions.
Results: Our results showed that ADC entropy in histogram parameters and kinetic pattern in clinicoradiologic parameters were identified as the most valuable predictors for differentiating MRI-only lesions, and a nomogram combining them exhibited better diagnostic performance than the two variables alone.
Impact: A nomogram combining ADC entropy and kinetic pattern, as a simple, objective, and noninvasive tool, displays satisfactory diagnostic performance for MRI-only suspicious lesions and may be utilised to avoid unnecessary biopsy.
Background and Purpose
Breast MRI can detect suspicious breast lesions (BI-RADS category 4 or 5) undetected by mammography and ultrasound; therefore, we assigned such lesions named "MRI-only" breast lesions1,2. MRI-guided vacuum-assisted breast biopsy (VABB) is necessary to sample suspicious lesions on breast MRI if they are invisible on second-look ultrasound (detection rate reported in the literature is 55.3%)3. However, MRI-guided VABB presents a range of issues. For example, biopsy carries the risk of complications, etc. Therefore, a simple, objective, and noninvasive approach is required to improve the diagnostic accuracy of MRI-only suspicious lesions. In our previous work4, we found that quantitative apparent diffusion coefficient (ADC) metrics based on large 2D-ROI measurements, particularly mean ADC values, exhibited superior performance over BI-RADS features in distinguishing MRI-only suspicious lesions. Beyond that, we wished to ascertain whether ADC-based histogram parameters are of added value for the classification of MRI-only suspicious lesions. Hence, this study is the first to use histogram analysis to further investigate the additional value of diffusion-weighted imaging (DWI) for the diagnosis of MRI-only suspicious lesions and to establish a visual nomogram.Materials and methods
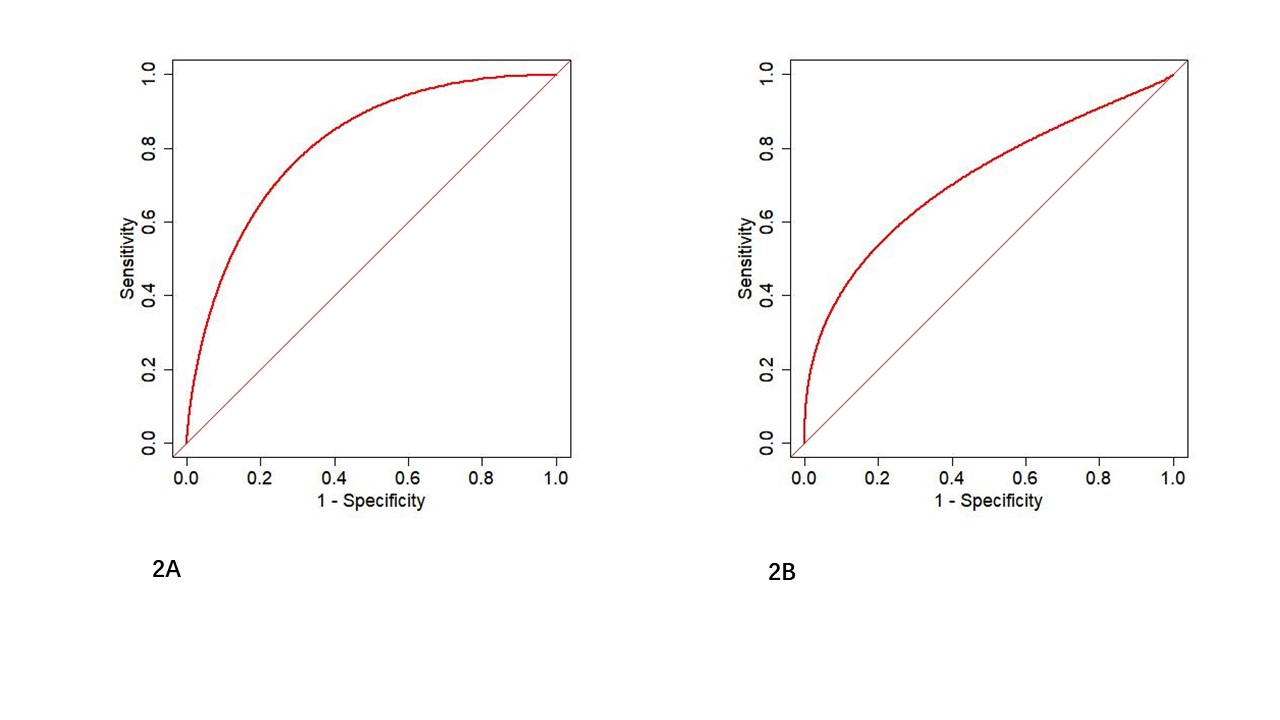
Ninety patients who underwent breast MRI between May 2017 and August 2023 and were found to have MRI-only suspicious lesions were retrospectively included and randomly divided into training (n = 62) and validation (n = 28) cohorts. The clinical information and MRI features of each patient were reviewed and analyzed. The ADC maps of each patient were subjected to histogram analysis, and then 17 histogram parameters were extracted. Univariate and multivariate logistic regression analyses were performed to identify significant variables associated with predicting MRI-only malignant lesions, which were then included in the nomogram. The diagnostic performances of significant variables and the nomogram were evaluated and compared in terms of the area under the receiver operating characteristic (ROC) curve (AUC) and DeLong’s test.Results
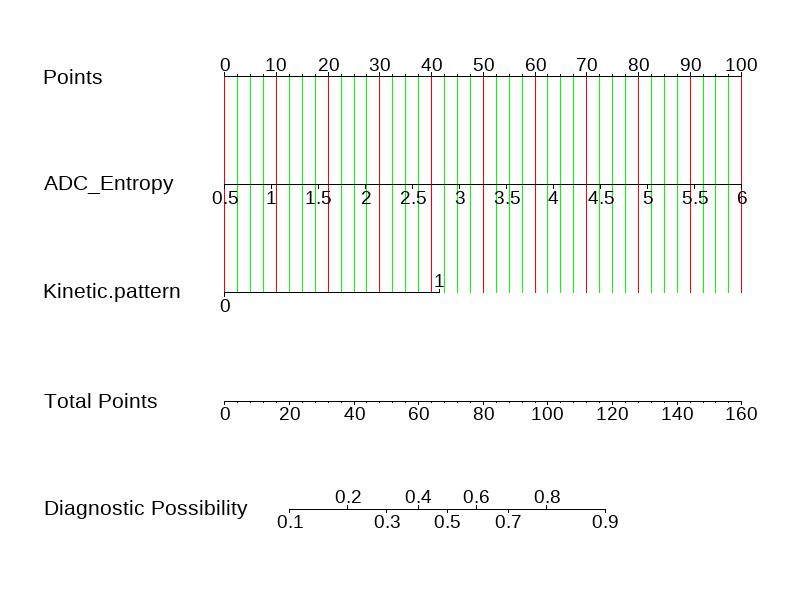
The kinetic pattern in clinicoradiologic features (P = 0.004, odds ratio [OR] = 2.268) and ADC entropy in histogram parameters (P = 0.003, OR = 6.49) were significant variables associated with the classification of MRI-only suspicious lesions. The C-index values for the nomogram combining ADC entropy and kinetic pattern were 0.820 (95% confidence interval [CI]: 0.702–0.906) for the training cohort and 0.728 (95% CI: 0.528–0.878) for the validation cohort.Discussion and Conclusions
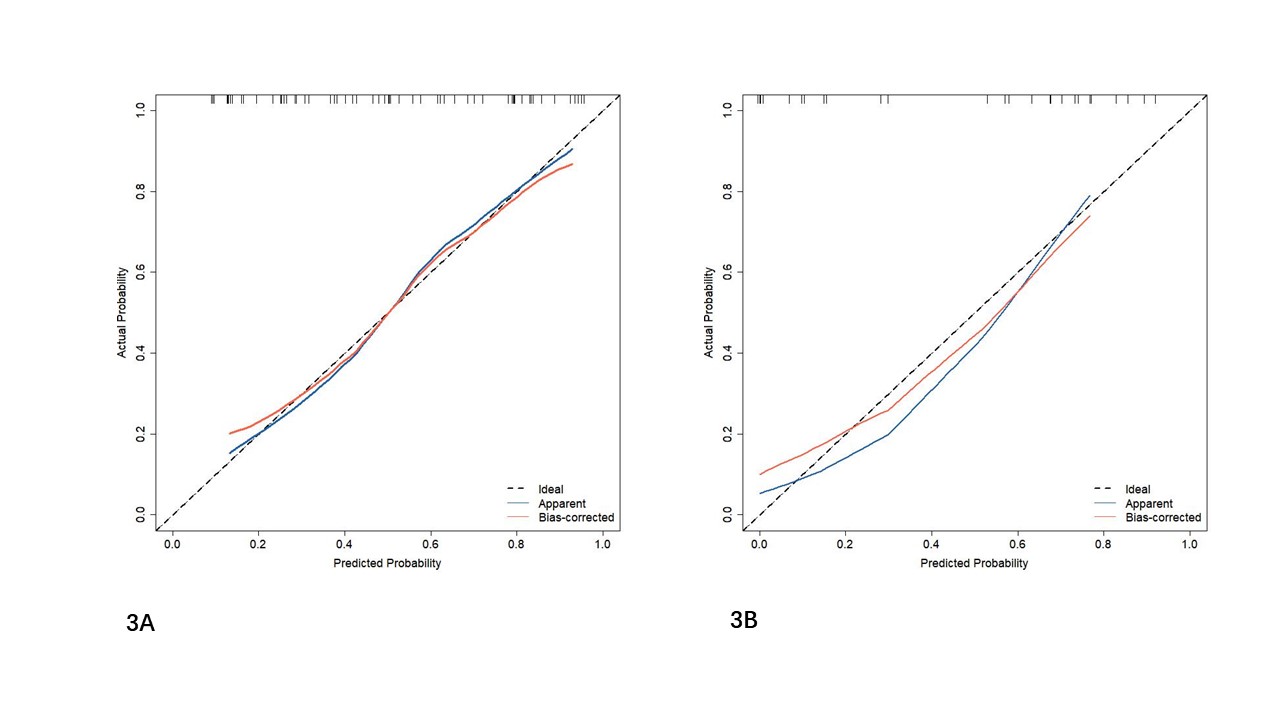
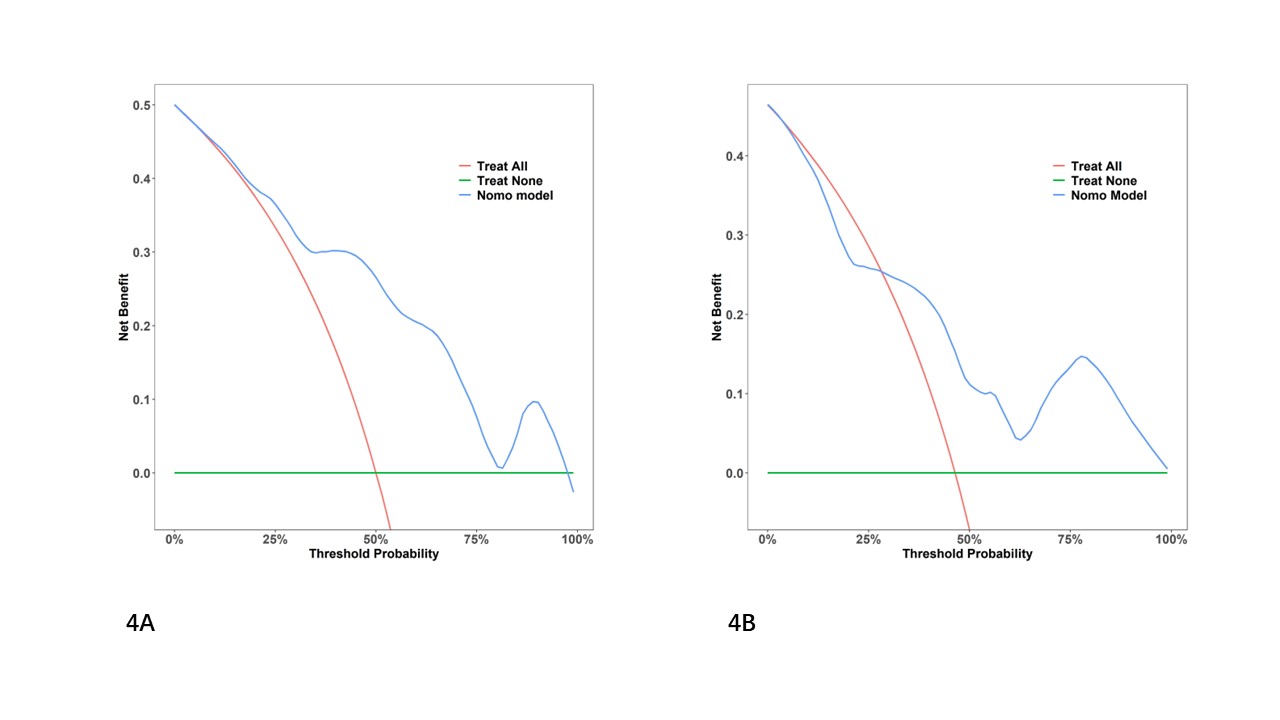
Accurate diagnosis of MRI-only suspicious lesions is important for clinical decision-making and management. Our results showed that the values of histogram parameters (ADC energy, entropy, range, and uniformity) differed significantly between benign and malignant groups of MRI-only suspicious lesions, promising for differentiating between the two groups of lesions. ADC entropy in histogram parameters and kinetic pattern in clinicoradiologic parameters were identified as the most valuable predictors for differentiating MRI-only lesions, and a nomogram combining them exhibited better diagnostic performance than the two variables alone. In addition, the nomogram was well-calibrated in both training and validation cohorts and demonstrated good clinical utility.Acknowledgements
Not applicableReferences
1. Arponen O, Masarwah A, Sutela A, et al. Incidentally detected enhancing lesions found in breast MRI: analysis of apparent diffusion coefficient and T2 signal intensity significantly improves specificity. Eur Radiol. 2016;26(12):4361-4370.
2. Nykänen A, Arponen O, Sutela A, Vanninen R, Sudah M. Is there a Role for Contrast-enhanced Ultrasound in the Detection and Biopsy of MRI Only Visible Breast Lesions? Radiol Oncol. 2017;51(4):386-392.
3. Aribal E, Tureli D, Kucukkaya F, Kaya H. Volume Navigation Technique for Ultrasound-Guided Biopsy of Breast Lesions Detected Only at MRI. AJR American Journal of Roentgenology. 2017;208(6):1400-1409.
4. Li X, Wang H, Gao J, Jiang L, Chen M. Quantitative apparent diffusion coefficient metrics for MRI-only suspicious breast lesions: any added clinical value? Quant Imaging Med Surg. 2023;13(10):7092-7104.
Figures