4311
Pilot implementation of vendor-provided on-scanner gradient nonlinearity correction for breast tumor ADC measures in a prospective trial1Department of Radiology, University of Washington, Seattle, WA, United States, 2Department of Bioengineering, University of Washington, Seattle, WA, United States, 3Department of Radiology, University of Michigan, Ann Arbor, MI, United States, 4MR Clinical Science, Philips, Best, Netherlands, 5Department of Radiology, College of Medicine, Chung-Ang University Hospital, Seoul, Korea, Republic of, 6Philips Healthcare, Bothell, WA, United States, 7Advanced Imaging Research Center, Oregon Health and Science University, Portland, OR, United States
Synopsis
Keywords: Breast, Gradients, Gradient Non linearity
Motivation: Improve accuracy of ADC measurement by correcting spatial nonuniformity of diffusion weighting caused by gradient nonlinearity (GNL) using novel vendor implemented on-scanner tools
Goal(s): Evaluate GNL correction of breast tumor ADC in a treatment response study
Approach: Implement on-scanner GNL correction, evaluate uncorrected and corrected tumor ADCs, evaluate GNL bias and ADC changes pre-treatment and post one cycle of neoadjuvant chemotherapy.
Results: Preliminary results from this study indicate adequate performance of the vendor implemented GNL correction of ADC in breast DWI assessment of response to neoadjuvant chemotherapy.
Impact: This pilot study demonstrates vendor-implemented GNL-correction (GNC) of spatially dependent b-value bias can dramatically simplify the process of obtaining more accurate ADC measures, which can improve robustness of ADC as a biomarker for treatment response.
Introduction
Apparent Diffusion Coefficient (ADC) has shown potential as a non-invasive biomarker to predict tumor response in neoadjuvant chemotherapy (NAC) trials [1]. Previous retrospective studies have demonstrated that offline correction for spatial non-uniformity of diffusion weighting (DW) b-values caused by system-specific gradient nonlinearity (GNL) can improve ADC accuracy. The bias in ADC measures is mainly determined by the gradient platform and the tissue offset from magnet isocenter [2]. In longitudinal studies such as for monitoring response to therapy, scanner system and patient positioning may vary between MRI examinations. Emerging vendor provided GNL correction (GNC) tools can generate accurate ADC maps in real time, increasing feasibility of integration in clinical workflow [3]. The purpose of this study was to prospectively explore the utility of on-scanner GNL correction for breast cancer ADC measures in a longitudinal NAC response study.Method
Study Cohort: In this ongoing prospective IRB approved study, women diagnosed with breast cancer and recommended for NAC as a part of their clinical care were enrolled to undergo longitudinal MRI monitoring during treatment. They underwent research MRIs at four treatment timepoints: 1) pre-treatment (baseline), 2) after one cycle of NAC (post-NACx1), 3) mid-treatment, and 4) after completion of NAC and prior to surgery. For this preliminary analysis of GNC efficacy, we evaluated only the first two treatment timepoints (pre-treatment and post-NACx1).MRI Acquisition: MRI acquisitions were performed on a 3T clinical scanner using a 16-channel breast coil (Achieva [60 cm bore diameter with Mammotrak coil] or Ingenia system [70 cm bore with dStream coil], Philips, Best, Netherlands). Data were acquired according to ACR guidelines, including DCE, T2w TSE, and DWI. DWI was acquired with b = 0, 100, 600, 800 s/mm2, TR/TE = 3500/66 ms, SENSE = 2.8, MB SENSE = 2, EPI factor = 67, and 1.8 × 1.8 × 4 mm3 resolution. DWI and ADC maps before and after GNC were created on the scanner in real time.
Image Processing: Tumor regions of interest (ROIs) were segmented on b=800 s/mm2 images using a semi-automated threshold tool, supervised by a fellowship trained radiologist. The tumor ROIs were propagated to the scanner generated ADC maps. All image processing was performed in the MATLAB environment. Fractional Bias was calculated as (ADC-ADCGNC)/ADCGNC for ROI-mean ADC values.
Statistical Analysis: Paired Wilcoxon signed-rank test was used to compare mean ADC values between visits and between ADC and ADCGNC values. All statistical analysis was performed in R.
Results
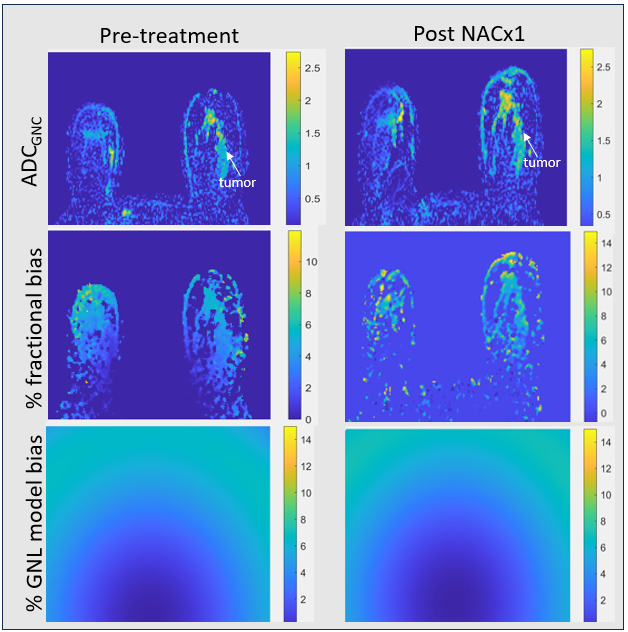
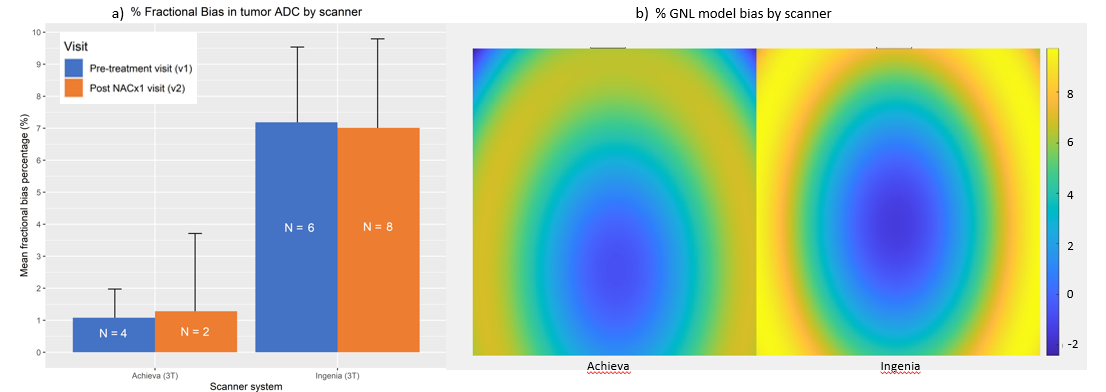
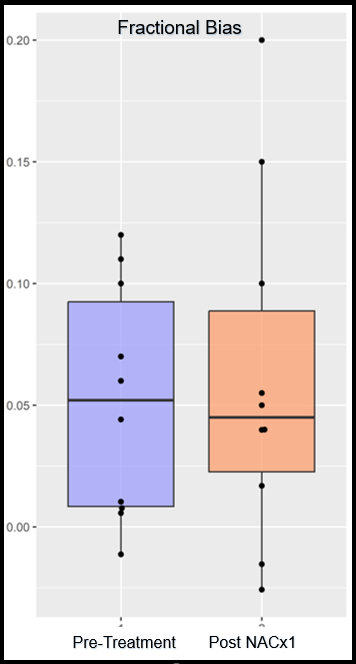
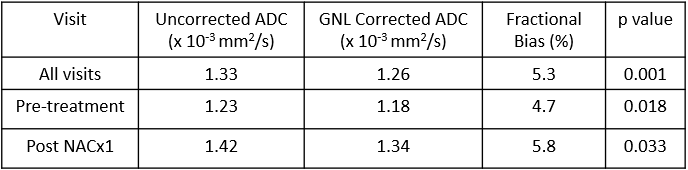
On-scanner GNL-corrected ADC maps were generated for 10 women at baseline and post-NACx1 visits. Of these, 80% (8/10) cases were invasive ductal carcinomas (IDC), 10% (1/10) were invasive lobular carcinomas (ILC) and 1 was a mixture of IDC and ILC. The tumor ROI sizes ranged between 18 and 43 voxels. The ADCGNC map, percentage fractional bias map and the percent GNL model bias map for a patient on the Achieva scanner system are shown in Fig1, indicating good agreement between predicted and observed fractional bias. 30% (6/20) of the exams were scanned on the Achieva system and the remaining on the Ingenia system. The %fractional bias in tumor ADC was higher for the Ingenia versus Achieva gradient systems, which is consistent with the % GNL bias model for these systems (Fig2). GNL corrected tumor ADC measures were significantly lower than uncorrected ADC measures for all visits (Table 1). Observed mean tumor fractional bias was 4.7% and 5.8% for the baseline and post NACx1 visits, respectively, for the entire cohort. Larger unexpected fractional bias was also observed in some patients. (Fig 3).Discussion
On-scanner ADC GNC maps can be generated in real time, which can dramatically simplify data processing. Observed differences in % fractional bias of tumor ADC measures by scanner system could be attributed in part to the differences in bore diameter, breast coil geometry, and table position. Previous studies have shown that predicted GNL bias for typical breast DWI FOV on gradient systems used here should be positive and within 10% [2]. Larger fractional bias deviations (> 10%) with negative excursions were observed for some low SNR cases, which will be investigated with off-scanner ADC analyses and bias model comparisons. Implementing the on-scanner GNL correction can potentially improve the accuracy of ADC as a biomarker for treatment response while accounting for scanner platform and patient positioning variations. Increasing availability of GNL correction on multi-vendor platforms should help standardize this technique for accurate ADC measurements. Preliminary results from this study indicate adequate performance of the vendor provided GNL correction on breast DWI.Acknowledgements
This study was funded by grants from National Institutes of Health R01 CA248192 and academic industrial partnership R01 CA190299.References
1. Partridge SC, Zhang Z, Newitt DC, Gibbs JE, Chenevert TL, Rosen MA, Bolan PJ, Marques HS, Romanoff J, Cimino L, Joe BN, Umphrey HR, Ojeda-Fournier H, Dogan B, Oh K, Abe H, Drukteinis JS, Esserman LJ, Hylton NM; ACRIN 6698 Trial Team and I-SPY 2 Trial Investigators. Diffusion-weighted MRI Findings Predict Pathologic Response in Neoadjuvant Treatment of Breast Cancer: The ACRIN 6698 Multicenter Trial. Radiology. 2018 Dec;289(3):618-627. doi: 10.1148/radiol.2018180273. Epub 2018 Sep 4. PMID: 30179110; PMCID: PMC6283325.
2. Malyarenko DI, Newitt DC, Amouzandeh G, Wilmes LJ, Tan ET, Marinelli L, Devaraj A, Peeters JM, Giri S, Vom Endt A, Hylton NM, Partridge SC, Chenevert TL. Retrospective Correction of ADC for Gradient Nonlinearity Errors in Multicenter Breast DWI Trials: ACRIN6698 Multiplatform Feasibility Study. Tomography. 2020 Jun;6(2):86-92. doi: 10.18383/j.tom.2019.00025. PMID: 32548284; PMCID: PMC7289257.
3. Chenevert, T.L., Pang, Y., Biswas, D., Paudyal, R., Konar, A., Liang, J., Wiles, L.J., Abad, N., Marinelli, L., Tariq, H., Devaraj, A., Turley, D., Peeters, J.M., Hylton, N.M., Newitt, D.C., Partridge, S. C. Shukla-Dave, A. & Malyarenko, D. Standardized QC procedure for vendor-implemented ADC correction of gradient nonlinearity bias in multi-center clinical trials. 32nd Annual Meeting of the ISMRM
Figures