4309
Stratified management of gestational hypertension: Superiority of functional magnetic resonance parameters over ultrasonography1Department of Radiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 2MR Research Collaboration, Siemens Healthineers, Shanghai, China, 3Department of Obstetrics & Gynecology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 4MR Research Collaboration, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Placenta, fMRI, gestational hypertension, placenta, preeclampsia, virtual magnetic resonance elastography
Motivation: Effective prenatal prediction of gestational hypertension (GH) can improve the clinical management of pregnant women at high risk of preeclampsia (PE) as pregnancy progresses.
Goal(s): To investigate the findings of placental virtual magnetic resonance elastography (vMRE), intravoxel incoherent motion (IVIM) parameters, and ultrasound examination to predict the progression of GH to PE.
Approach: We calculated vMRE and IVIM parameters and apparent diffusion coefficient and retrospectively performed ultrasound examinations. The differences in the aforementioned parameters were compared, and their predictive efficacy was evaluated.
Results: Patients with PE had higher placental stiffness and lower microcirculation.
Impact: Virtual magnetic resonance elastography and intravoxel incoherent motion comprise a vital complementary diagnostic method to conventional ultrasound screening for placental dysfunction in patients with high-risk hypertensive disorders in pregnancy, further improving the sensitivity and specificity of pregnancy screening.
Introduction
Hypertensive disorders in pregnancy (HDP) are serious complications of obstetrics (1). Preeclampsia (PE) is the most vital type of HDP, which is characterized by hypertension with proteinuria and/or target organ damage. It progresses from gestational hypertension (GH) and has serious impacts on maternal and fetal health (2). Early prediction of PE in GH is essential for timely action to prevent the progression of GH to PE and minimize adverse maternal and fetal outcomes. PE is a placental disorder. Doppler velocimetry can help in evaluating placental disorders. Intravoxel incoherent motion (IVIM) techniques can detect placenta microcirculation perfusion (3-5). Virtual magnetic resonance elastography (vMRE) was recently proposed for noninvasively assessing the elasticity of soft tissues such as the liver and placenta (6-8). However, no studies have assessed and stratified HDP based on placental functional MRI parameters. We aimed to use Doppler and placental vMRE and IVIM parameters to differentiate pregnant women with PE from those with GH.Methods
The institutional review board approved this retrospective study, and 38 patients were recruited. MRI examinations were performed using a 1.5T system (MAGNETOM Aera, Siemens Healthineers AG, Erlangen, Germany) with a 12-channel surface body coil and 2 embedded spine coils. IVIM sequence was acquired (TR/TE 1300 milliseconds/167 milliseconds; slice thickness 4.0 mm; FOV 380 × 309 mm2) with 7 b values of 0, 50, 100, 150, 200, 500, and 800 s/mm2. The volume of interest was drawn by 2 radiologists with 5 and 10 years of experience, respectively. Using diffusion-weighted images, we obtained a lower b value (b = 200 s/mm2) and paired it with a higher b value (b = 800 s/mm2) to generate the vMRE parameter μdiff using vMRE toolbox: μdiff=α∙ln(S200⁄S800 )+β(α= -9.8, β=14)(6, 8). IVIM parameters [true diffusion coefficient (D), pseudo-diffusion coefficient (D*), and perfusion fraction (f)] and apparent diffusion coefficient (ADC) value were processed with FireVoxel software (CAI2R; New York University, NY, USA). The pulsatility index (PI), resistance index (RI), and peak systolic velocity/end-diastolic velocity (S/D) in the umbilical artery (UA) and middle cerebral artery (MCA) were recorded retrospectively. The cerebroplacental ratio (CPR) value was calculated as MCA – PI/UA – PI. The patient selection flowchart and 2 case studies are displayed in Figure 1.Results
A total of 38 patients were divided into 2 groups: 24 with PE and 14 with GH. The demographic and clinical characteristics are depicted in Table 1. The f and CPR values were substantially lower and µdiff, UA-PI, UA-RI, and UA-S/D values were considerably higher in the PE group compared with the GH group (P <.05) (Table 2 and Fig. 2). The f had the highest area under curve (AUC) value of 0.821 for differentiating PE from GH compared with other parameters. The fMRI combined model (µdiff and f) exhibited a higher AUC of 0.847 compared with Doppler combined model (UA-PI, UA-RI, UA-S/D, and CPR) and any single model. The model combining all parameters with statistical significance displayed the best predictive performance with an AUC of 0.920 (Table 3 and Fig. 3).Discussion
These ultrasound findings suggested that preeclampsia increased fetal–placental circulatory resistance, leading to reduced diastolic blood flow in the UA and increased PI, RI, and S/D. (9). The changes in CPR highlighted changes in cerebral blood flow during hypoxia, indicating placental abnormalities even when MCA and UA-PI values were normal (10). We observed lower f values in the PE groups, aligning with previous studies indicating that diminished IVIM-based perfusion fraction (f) values correlated with placental dysfunction like fetal growth restriction (FGR) (7, 11, 12). This might be explained by more severe placental pathology in early-onset placental dysfunction cases. We also observed that the stiffness (µdiff) was higher in the PE group than in the GH group. The biomechanical characteristics of human tissue can be evaluated noninvasively using vMRE (6, 7, 13). Placental abnormalities commonly observed in PE, such as infarction, inflammation, and fibrosis, may contribute to a more compact and stiffer placental structure. The ROC results suggested that fMRI parameters could complement conventional ultrasound screening for patients at high risk of placental dysfunction in hypertensive disorders in pregnancy, leading to improved sensitivity and specificity in pregnancy screening. Combining ultrasound and fMRI in a comprehensive model provides a superior performance in predicting the progression of GH to PE.Conclusion
vMRE and IVIM parameters may be superior to ultrasound examination in predicting the progression of GH to PE.Acknowledgements
This study was funded by the Young Scholars Fostering Fund of the First Affiliated Hospital of Nanjing Medical University (PY2021002).
References
1. Tsakiridis I, Giouleka S, Arvanitaki A, et al. Gestational Hypertension and Preeclampsia: An Overview of National and International Guidelines. Obstet Gynecol Surv 2021; 76:613-633.
2. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health 2014; 2:e323-e333.
3. Chen T, Zhao M, Song J, et al. The effect of maternal hyperoxygenation on placental perfusion in normal and Fetal Growth Restricted pregnancies using Intravoxel Incoherent Motion. Placenta 2019; 88:28-35.
4. Deng J, Zhang A, Zhao M, et al. Placental perfusion using intravoxel incoherent motion MRI combined with Doppler findings in differentiating between very low birth weight infants and small for gestational age infants. Placenta 2023; 135:16-24.
5. Malmberg M, Kragsterman E, Sinding M, et al. Perfusion fraction derived from IVIM analysis of diffusion-weighted MRI in the assessment of placental vascular malperfusion antenatally. Placenta 2022; 119:1-7.
6. Deng J, Cao Y, Lu Y, et al. Value of placental virtual magnetic resonance elastography and intravoxel incoherent motion-based diffusion and perfusion in predicting adverse outcomes of small-for-gestational-age infants. Insights Imaging 2023; 14:153.
7. Kromrey ML, Le Bihan D, Ichikawa S, Motosugi U. Diffusion-weighted MRI-based Virtual Elastography for the Assessment of Liver Fibrosis. Radiology 2020; 295:127-135.
8. Le Bihan D, Ichikawa S, Motosugi U. Diffusion and Intravoxel Incoherent Motion MR Imaging-based Virtual Elastography: A Hypothesis-generating Study in the Liver. Radiology 2017; 285:609-619.
9. Zhou P, Sun Y, Tan Y, An Y, Wang X, Wang L. Fetal and Neonatal Middle Cerebral Artery Hemodynamic Changes and Significance under Ultrasound Detection in Hypertensive Disorder Complicating Pregnancy Patients with Different Severities. Comput Math Methods Med 2022; 2022:6110228.
10. Zarean E, Azami N, Shahshahan Z. Predictive Value of Middle Cerebral Artery to Umbilical Artery Pulsatility Index Ratio for Neonatal Outcomes in Hypertensive Disorders of Pregnancy. Adv Biomed Res 2022; 11:46.
11. Siauve N, Hayot PH, Deloison B, et al. Assessment of human placental perfusion by intravoxel incoherent motion MR imaging. J Matern Fetal Neonatal Med 2019; 32:293-300.
12. Sohlberg S, Mulic-Lutvica A, Lindgren P, Ortiz-Nieto F, Wikström AK, Wikström J. Placental perfusion in normal pregnancy and early and late preeclampsia: a magnetic resonance imaging study. Placenta 2014; 35:202-206.
13. Aunan-Diop JS, Andersen M, Friismose AI, et al. Virtual magnetic resonance elastography predicts the intraoperative consistency of meningiomas. J Neuroradiol 2023; 50:396-401.
Figures
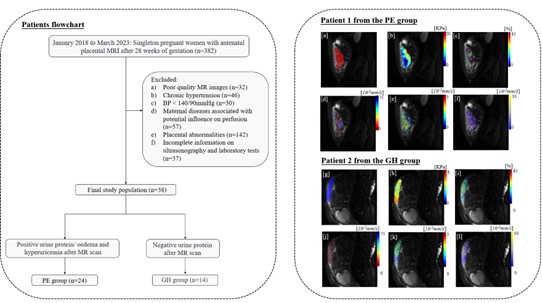
Figure 1. Patient selection flowchart and 2 cases studies.
Patient 1 was in the PE group with 33.5 weeks’ gestation at the time of the MRI scan (a–f). Patient 2 was in the GH group with 34 weeks’ gestation at the time of the MRI scan (g–l). (a and g) Region of interest was drawn on a diffusion-weighted image (b = 100 mm2/s) of the placenta. (b and h) vMRE map. (c–e and i–k) IVIM-based diffusion and perfusion pseudo-color maps of f, D*, and D. (f and l) Apparent diffusion coefficient map.
Abbreviations: GH, gestational hypertension; PE, preeclampsia; vMRE, virtual magnetic resonance elastography.
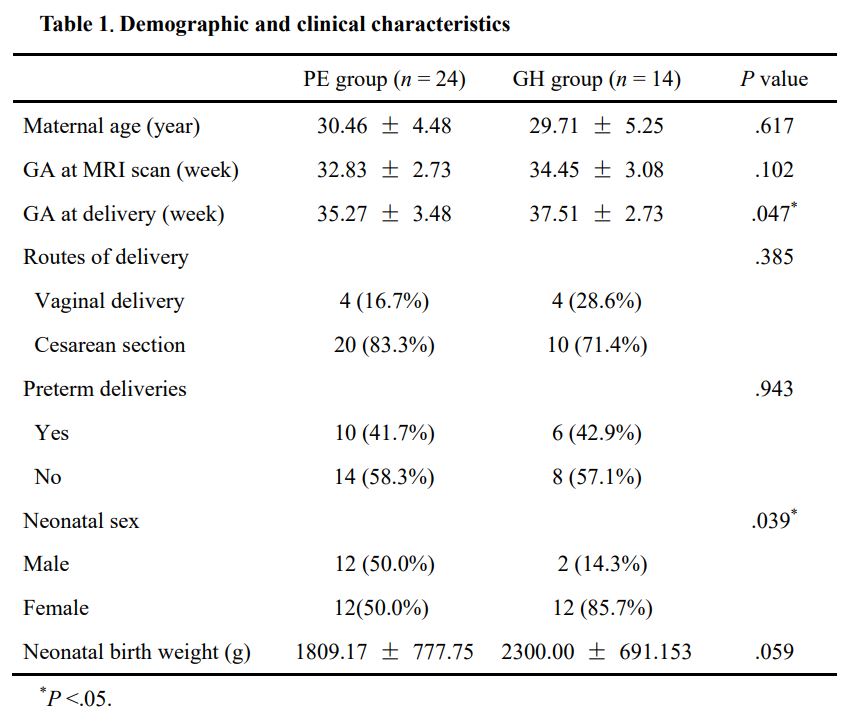
Table 1. Demographic and clinical characteristics
Abbreviations: GA, Gestational age; GH, gestational hypertension; MRI, magnetic resonance imaging; PE, preeclampsia.
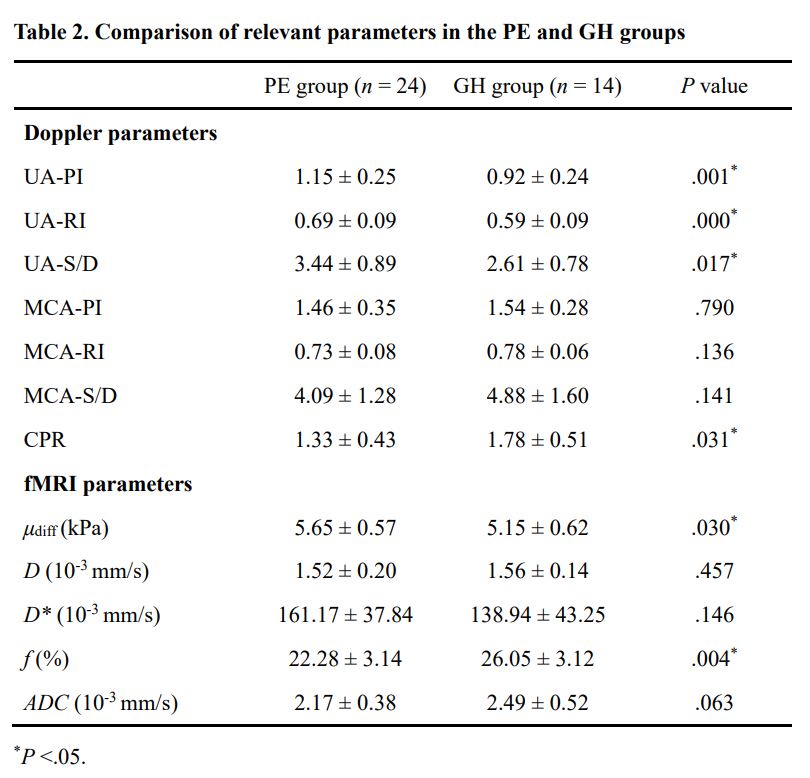
Table 2. Comparison of relevant parameters in the PE and GH groups
Abbreviations: ADC, apparent diffusion coefficient; CPR, cerebroplacental ratio; D, true diffusion coefficient; D*, pseudo-diffusion coefficient; μdiff, diffusion-weighted imaging–based shear modulus; f, perfusion fraction; fMRI, functional magnetic resonance imaging; GH, gestational hypertension; MCA, middle cerebral artery; MRI, magnetic resonance imaging; PE, preeclampsia; PI, pulsatility index; RI, resistance index; S/D, peak systolic velocity/end-diastolic velocity; UA, umbilical artery.
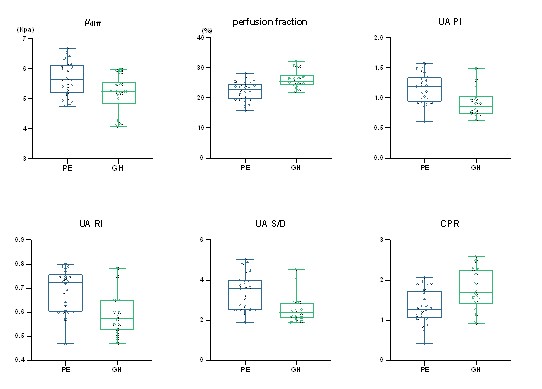
Figure 2. Box plots of µdiff, f, UA-PI, UA-RI, and UA-S/D for the PE and GH groups.
CPR, Cerebroplacental ratio; μdiff, diffusion-weighted imaging–based shear modulus; PI pulsatility index; RI, resistance index; S/D, peak systolic velocity/end-diastolic velocity; UA, umbilical artery.
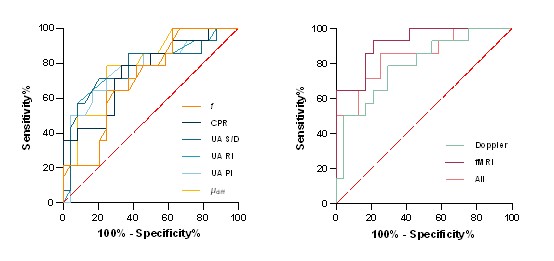
Figure 3. ROC curves for predicting PE groups from GH groups.
Abbreviations: ADC, Apparent diffusion coefficient; CPR, cerebroplacental ratio; μdiff, diffusion-weighted imaging–based shear modulus; f, perfusion fraction; fMRI, functional magnetic resonance imaging; MRI, magnetic resonance imaging; PI, pulsatility index; RI, resistance index; S/D, peak systolic velocity/end-diastolic velocity; UA, umbilical artery.