4302
Ex-vivo MRI of Placentas from Women with Congenital Heart Disease: Reproducibility Assessment and Initial Results1Radiology, University of California San Diego, La Jolla, CA, United States, 2Biomedical Engineering, Technion- Israel Institute of Technology, Haifa, Israel, 3Faculty of Medicine and Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel, 4Sagol Brain Institute, Tel Aviv Sourasky Medical Cente, Tel Aviv, Israel, 5Department of Pathology, University of California San Diego, La Jolla, CA, United States, 6Sanford Consortium for Regenerative Medicine, University of California San Diego, La Jolla, CA, United States, 7Bioengineering, University of California San Diego, La Jolla, CA, United States, 8Rady Children’s Hospital, San Diego, CA, United States
Synopsis
Keywords: Placenta, Cardiovascular
Motivation:
Women with CHD are prone to pregnancy complications associated with placental-dysfunction. Our understanding of this phenomenon remains limited, with unexplored data processing reproducibility.
Goal(s):
1. Investigate maternal cardiovascular health's impact on placental vascular architecture.
2. Evaluate data processing method reproducibility.
Approach:
Placentas from mothers with cardiovascular disease and controls underwent ex-vivo MRI. Placental volume and vascular tree architecture were analyzed by two independent double-blinded annotators using established methods.
Results:
No group differences were observed. Annotator-related differences were only observed for vascular volume. We emphasize the need for expanded research into placental changes in women with cardiovascular diseases and standardization of data processing methods.
Impact:
This study investigates maternal cardiovascular health's impact on placental vascular architecture and evaluates data processing methods reproducibility. In order to understand placental dysfunction patterns across different populations, the need for expanded research and method standardization became evident.
Introduction
Women with congenital heart disease (CHD) represent the largest group of pregnant cardiac patients in developed countries.1 Pregnancy elicits significant cardiovascular (CV) stress,2 increasing the risk of adverse cardiac events and mortality in these patients. Additionally, women with CHD are more prone to pregnancy complications related to placental dysfunction.4 However, the mechanisms linking maternal CV status and placental function are poorly understood. Thus, we aim to 1) assess the effect of maternal CV on placental vascular architecture ex-vivo, and 2) evaluate the reproducibility of established methods to process these data.Methods
In this IRB-approved study, twelve placentas were donated by women recruited from our institution’s Maternal-Fetal care clinics and Obstetrics/Cardiac clinic.Placental preparation
All placentas were prepared and imaged within 48hrs of delivery. Samples were submerged in a warm phosphate-buffered saline (PBS) bath at 37°C for 20mins. Afterwards, a catheter was inserted into the umbilical vessels and flushed with heparin and saline solution over 4 hours. Samples were removed from the bath and placed with the chorionic plate facing down to remove excess PBS. Samples were returned to the bath for 20mins, after which safflower oil at 37°C was infused into the umbilical vein using the same catheter. The process continued until oil was observed returning via umbilical arteries or vascular resistance prevented further infusion, at which point the umbilical cord was clamped.
Image acquisition
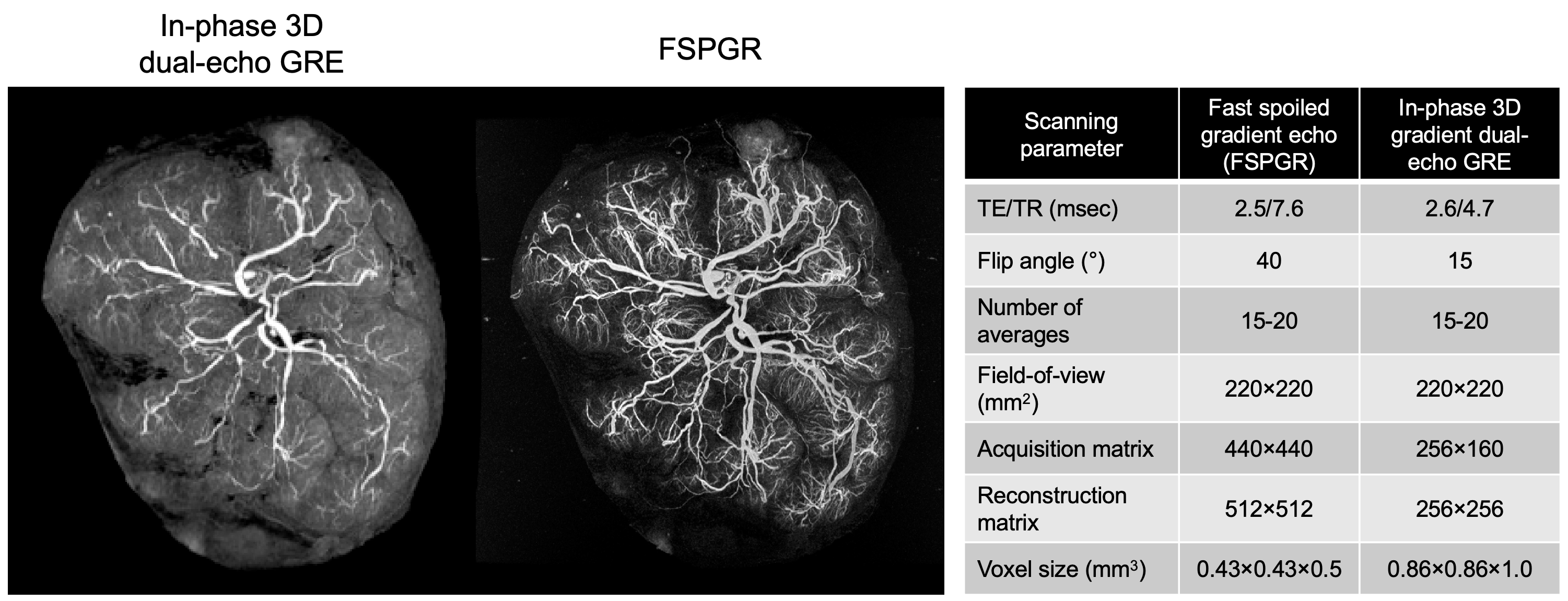
Placentas were imaged in a 3T scanner (MR750, GE Healthcare, Chicago IL) using a 10-element cardiac coil. Fast spoiled gradient echo (FSPGR) and 3D-gradient dual-echo GRE sequences were collected (Figure 1).
Image analysis
Data processing was performed in Analyze 12.0 (AnalyzeDirect, Overland Park, KS) as described by Link et al.5 Four structural parameters were extracted and calculated:
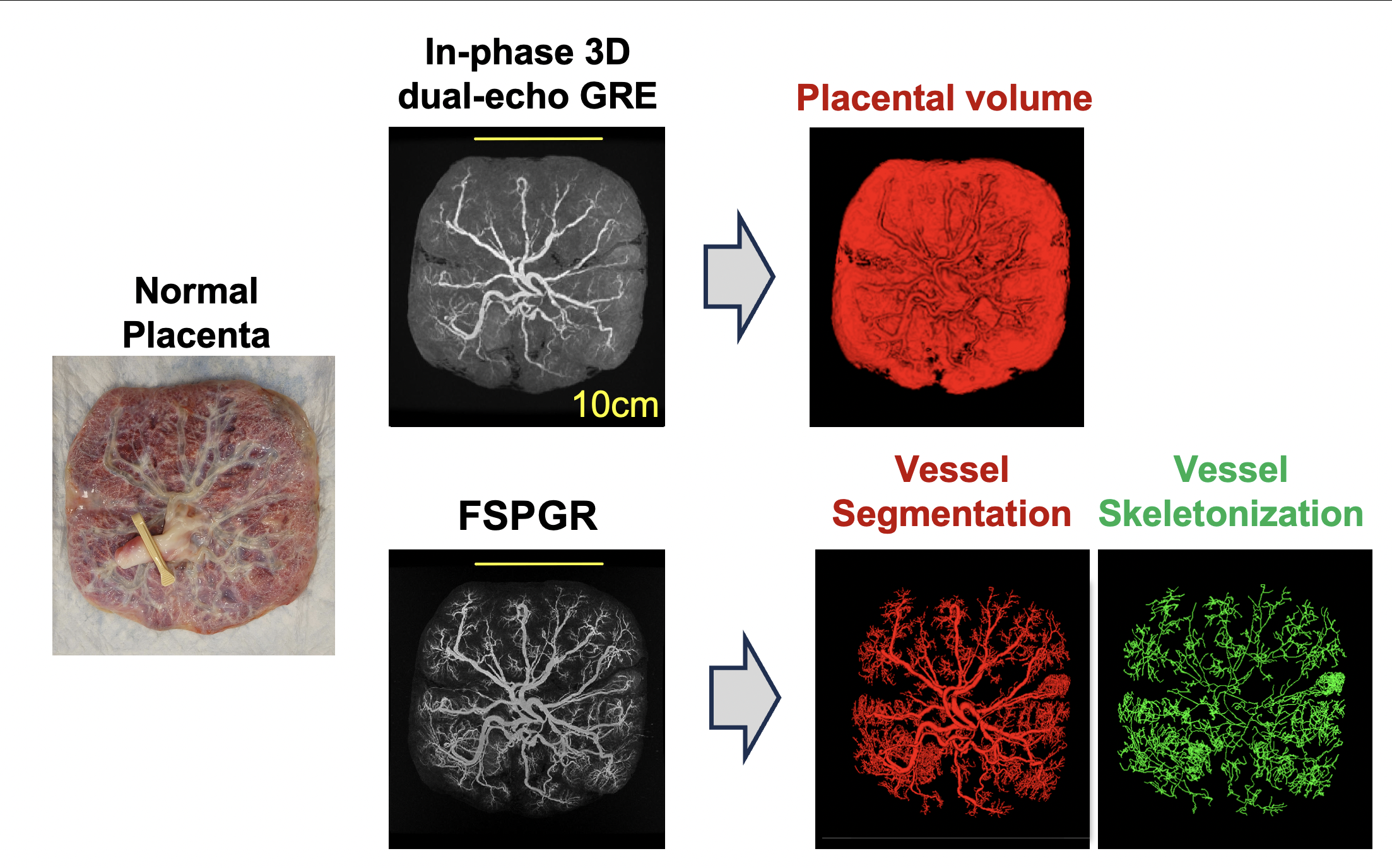
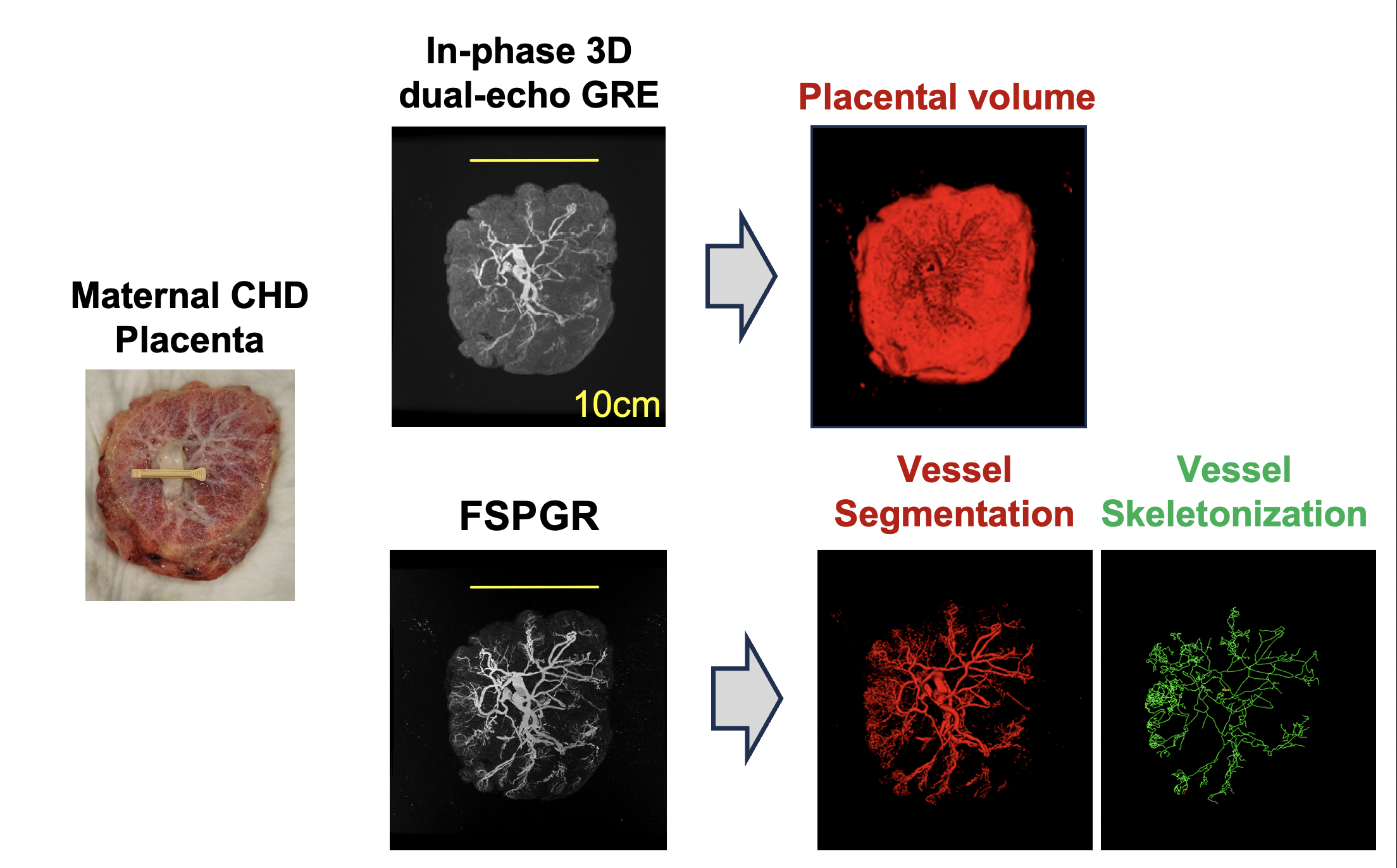
1. Placental volume– manual threshold was used to segment the placenta and estimate its volume, from the GRE images (Figure 1).
2. The vascular tree was segmented from FSPGR images and used to quantify the number of vascular bifurcations and number of vascular generations (Figure 2).
3. The location of the umbilical cord insertion (centricity index, CI) was quantified based on GRE images by one annotator, as the distance from the insertion to the geometric center of the placenta, normalized by the placenta radius determined as the average of principal axes of the placental disc (0<CI<1).
4. Mother-to-daughter diameter ratio were manually calculated for the first six generations by one annotator.
Statistical analysis
Placental vascular architecture measurements were compared using two-way repeated-measures ANOVA and post-hoc tests to identify differences between patient groups and annotators.
Results
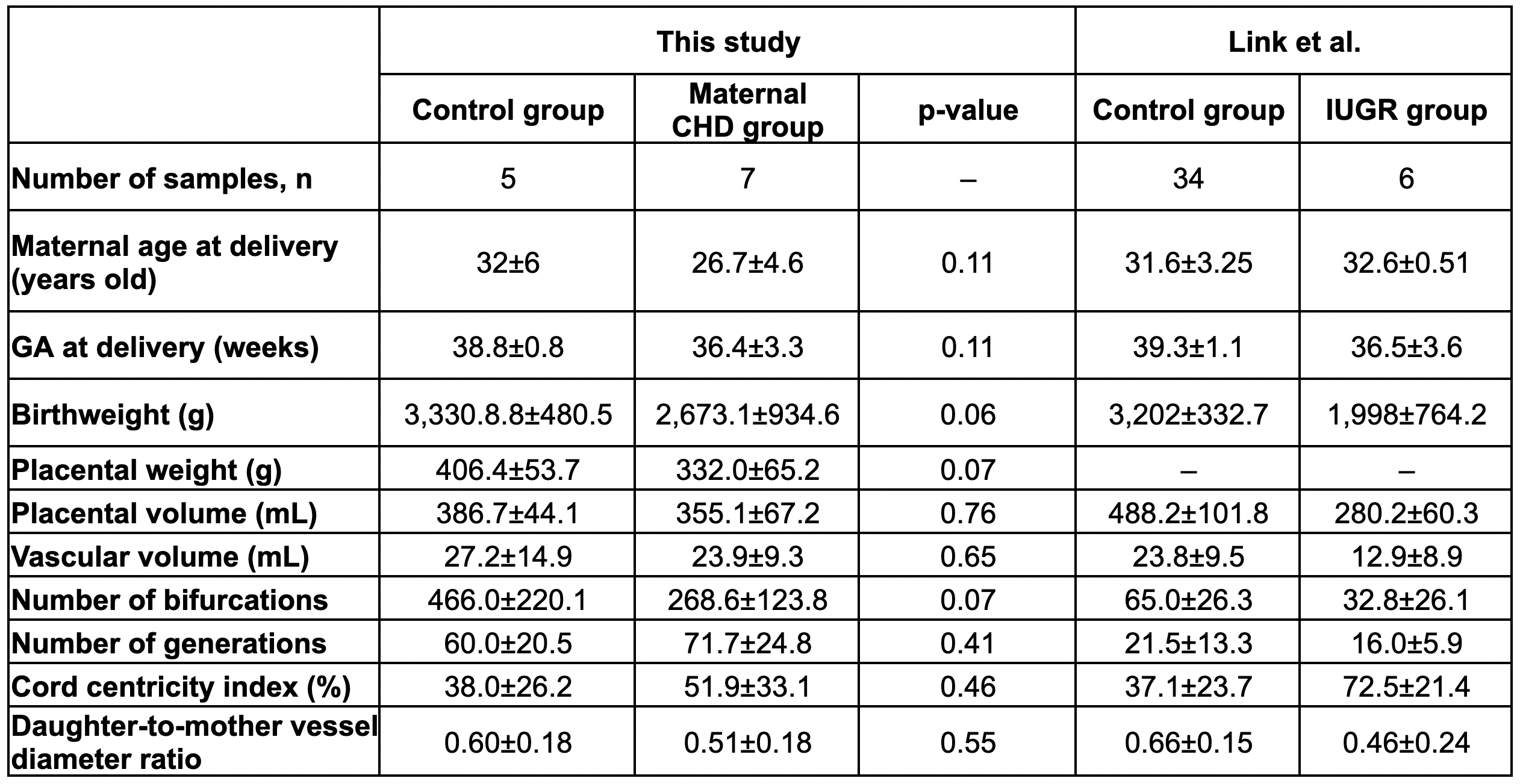
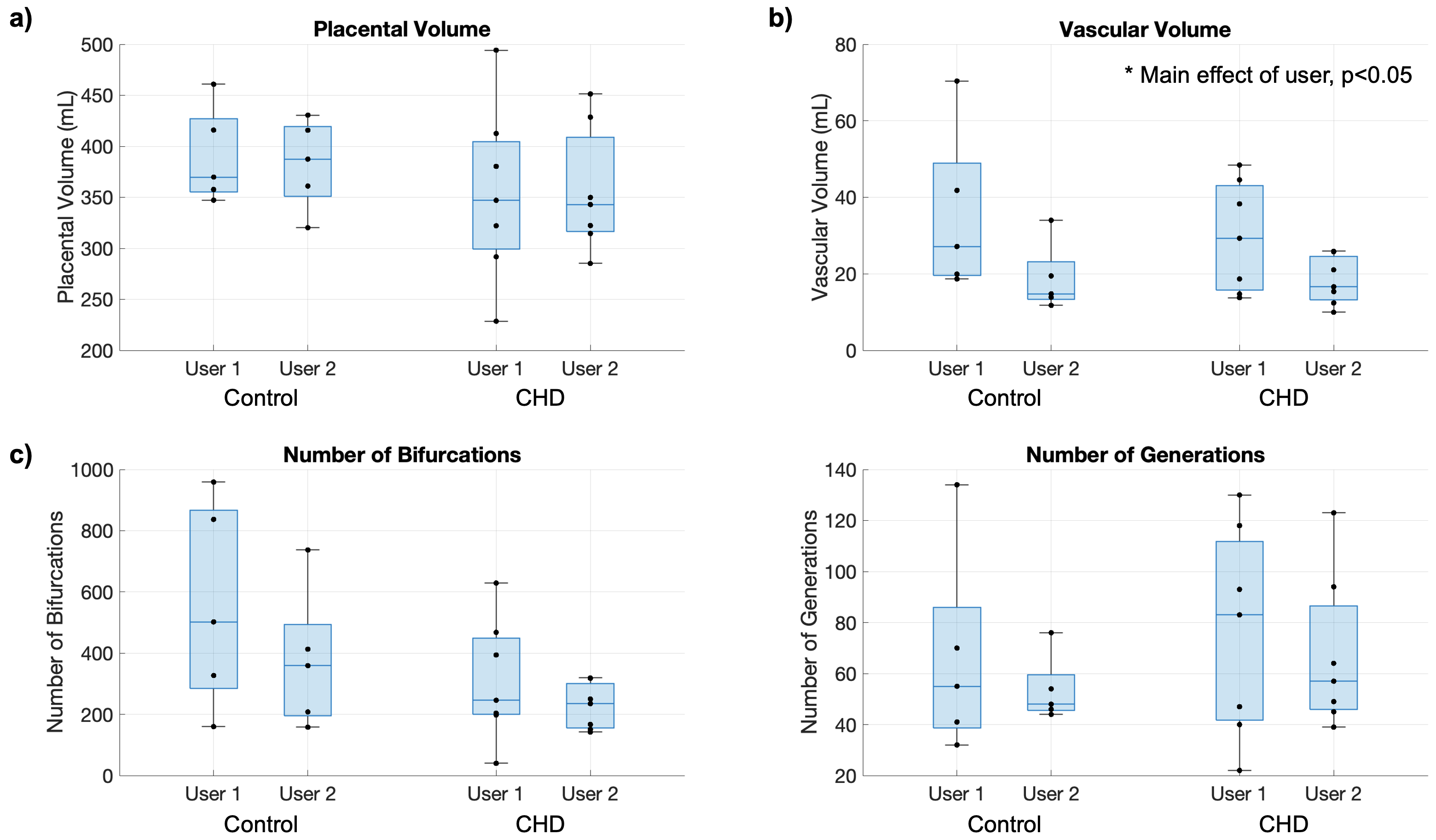
Basic demographic information of participants are shown in Table 1. No differences were observed between our control and CHD groups. However, two placentas from the maternal CHD pregnancies were from pregnancies diagnosed with intrauterine growth restriction (IUGR), and two had marginal umbilical cord insertion, one of them in both groups.No differences (p>0.05, Figure 4) were observed between annotators in terms of placental volume, number of bifurcations, and number of generations. However, the estimated vascular volume was different between annotators (Figure 4).
Discussion and Conclusions
Several MRI studies have explored ex-vivo placental imaging to identify vascular architectural differences between normal and disease groups.5-8 Our processing pipeline closely resembles that of Link et al. While in our cohort no differences were found between groups, when compared to the results of Link et al suggest that placentas of women with CHD (Figure 3) have a trend towards placentas in IUGR cases, which significantly differ from control. Notably, the CI of the control groups was consistent across studies. However, the IUGR group reported by Link exhibited significantly higher values compared to the maternal CHD group, suggesting greater deviations from the control cases in terms of the insertion point. This trend was also observed in the daughter-to-mother ratio.Our study revealed significantly higher numbers of vascular bifurcations and generations compared to Link et al. This could be due to differences in MRI acquisition parameters, motivating standardization to ensure quality evaluations and facilitate cross-study comparisons.
It's important to note that the study's small sample size limits our ability to detect differences between patient groups. Future efforts will involve expanding our enrollment, as well as correlating imaging findings to placental histopathology, to further assess placental vascular changes in women with CHD.
We demonstrate the robustness of placental vascular tree measurements to annotator variability. Variations in vascular volume suggest different annotators selected different segmentation threshold values. However, we hypothesize that the analysis of vascular tree elements is less sensitive to the choice of threshold. Future work aims to automate this pipeline for user independence.
Acknowledgements
Supported by UCSD Senate Grant.References
1 Deanfield, J. et al. Management of grown up congenital heart disease. Eur Heart J 24, 1035-1084 (2003). https://doi.org:10.1016/s0195-668x(03)00131-3
2 Ruys, T. P., Cornette, J. & Roos-Hesselink, J. W. Pregnancy and delivery in cardiac disease. J Cardiol 61, 107-112 (2013). https://doi.org:10.1016/j.jjcc.2012.11.001
3 Schlichting, L. E., Insaf, T. Z., Zaidi, A. N., Lui, G. K. & Van Zutphen, A. R. Maternal Comorbidities and Complications of Delivery in Pregnant Women With Congenital Heart Disease. J Am Coll Cardiol 73, 2181-2191 (2019). https://doi.org:10.1016/j.jacc.2019.01.069
4 Hayward, R. M., Foster, E. & Tseng, Z. H. Maternal and Fetal Outcomes of Admission for Delivery in Women With Congenital Heart Disease. JAMA Cardiol 2, 664-671 (2017). https://doi.org:10.1001/jamacardio.2017.0283
5 Link, D. et al. Placental vascular tree characterization based on ex-vivo MRI with a potential application for placental insufficiency assessment. Placenta 101, 252-260 (2020). https://doi.org:10.1016/j.placenta.2020.08.001
6 Chen, B. et al. Ex vivo magnetic resonance angiography to explore placental vascular anatomy. Placenta 58, 40-45 (2017). https://doi.org:10.1016/j.placenta.2017.08.002
7 Rasmussen, A. S. et al. High-resolution ex vivo magnetic resonance angiography: a feasibility study on biological and medical tissues. BMC Physiol 10, 3 (2010). https://doi.org:10.1186/1472-6793-10-3
8 Abaci Turk, E. et al. Placental MRI: Developing Accurate Quantitative Measures of Oxygenation. Top Magn Reson Imaging 28, 285-297 (2019). https://doi.org:10.1097/RMR.0000000000000221
Figures