4299
Does Amide proton transfer-weighted mri have diagnostic and differential value in ovarian cystic and predominantly cystic lesion ?1Qilu Hospital of Shandong University, Jinan city, Shandong province, China, 2GE Healthcare, Beijing, China, Beijing, China
Synopsis
Keywords: Pelvis, CEST & MT, APTw
Motivation: Ovarian cystic and predominantly cystic lesions are common tumor-like formations within the ovaries, necessitating precise diagnosis and differential analysis for effective clinical management.
Goal(s): This study examines the effectiveness of amide proton transfer-weighted (APTw) MRI in differentiating cystic or predominately cystic ovarian lesions.
Approach: 49 patients with ovarian lesions were prospectively scanned by APTw before surgery, and 20 volunteers were also scanned by APTw as a control group.
Results: The results demonstrate APTw MRI's substantial value in identifying and distinguishing common ovarian cystic and predominantly cystic lesions, offering enhanced diagnostic precision in ovarian pathology.
Impact: MR diagnostic techniques for ovarian lesions, including DWI and DCE-MRI, have their limitations. A timely diagnosis is crucial for improving patient prognosis. APTw imaging has shown research progress across various systems, yet its application in ovarian studies remains limited.
Introduction
Ovarian cystic and predominantly cystic lesions are common tumor-like formations within the ovaries, necessitating precise diagnosis and differential analysis for effective clinical management[1]. Beyond standard MR sequences, techniques such as DWI and DCE-MRI have gained traction[2]. Nevertheless, the inherent limitations of these approaches[3,4] have prompted a search for alternative MR imaging methodologies.Amide Proton Transfer-weighted (APTw) imaging, a member of the chemical exchange saturation transfer (CEST) family, is a non-invasive molecular imaging technique. It works by detecting proton exchange between amide compounds (3.5 ppm from bulk water) and bulk water in biological tissues, thus producing unique images useful in identifying diseased tissues[5]. Although APTw imaging has seen application in tumor diagnostics and neurology[6], specifically in differentiating benign from malignant tumors and determining malignancy levels through protein concentration in lesion tissues, its utility in ovarian lesions has not been extensively studied[7].
This study, therefore, focuses on evaluating the clinical utility of APTw MRI in distinguishing between cystic and predominantly cystic ovarian lesions.
Materials and Methods
SubjectsOvarian data from 20 volunteers and lesion data from 49 patients were included in this prospective study. All patients with lesions underwent surgical treatment and postoperative pathological diagnosis. Subsequently, the data were categorized into solid or cystic components. The solid components were organized as follows: solid components of normal ovaries (Group A, n=29) and malignant lesions (Group B, n=7). The cystic components were categorized as follows: the cystic fluid of follicles (Group C, n=31), benign lesions (Group D, n=46), and malignant lesions (Group E, n=12). Additionally, Group D was further subdivided into the cystic fluid of functional cysts (Group d1, n=8), endometriomas (Group d2, n=28), and cystadenomas (Group d3, n=10) (Figure 1).
MRI Imaging
A 3.0-T MR scanner (GE Medical Systems, DISCOVERY MR750W) with a 16-channel phased-array body coil was used for all subjects. The MRI sequences including T1WI, T2WI, DWI and APTw were performed. Detailed information about scan parameters was showed in Table 1.
Data analysis
All APTw imaging data were post-processed using vendor-provided software on a GE ADW4.6 workstation (Figure 2). Firstly, all lesions were divided into groups according to the postoperative pathological diagnosis, and then the MTRasym values of solid and cystic components of the lesions were measured by placing ROI respectively. Finally, statistical analysis was performed.Statistical analysis SPSS 25.0 statistic software was used. An independent-samples t-test was used for intergroup comparison, and one-way ANOVA was performed for multi-group comparison. The receiver operating characteristic curve (ROC) was used to evaluate the efficacy of differential diagnosis of different lesions. P<0.05 was considered statistically significant.
Results
For solid components of lesions, there was a statistically significant difference of MTRasym between Group A and Group B (p < 0.001). For cystic components, significant differences of MTRasym were obtained (F(2, 86) =30.36, p < 0.001) among the Groups C, D, and E, as well as Groups d1, d2 and d3 (F(2, 43)=87.83, p<0.001). With further post-hoc test, Group C showed significantly different MTRasym values from Group D (p<0.001) and Group E (p<0.001), Group d1 showed significantly different MTRasym from Group d2 (p<0.001) and Group d3 (p< 0.01), as well as between Group d2 and d3 (p < 0.001). Furthermore, statistical differences were observed between Groups C and d2, C and d3, E and d1, E and d2, all p<0.001. (Figure 3)
ROC analysis showed high AUC for the identification between Groups A and B, Groups C and D, Groups C and E, Groups d1 and d2, Groups d1 and d3, Groups d2 and d3, Groups C and d2, Groups C and d3, Groups E and d1, Groups E and d2, with all p<0.05. Detailed data are shown in Figure 4.
Discussion
In our study, APTw effectively identified protein differences between normal and abnormal diseased tissues. Despite some limitations in handling complex cystic fluids, APTw shows excellent diagnostic capability in distinguishing among three benign lesions: functional cysts, endometriomas, and cystadenomas, and between functional cysts and endometriomas in malignant lesions. Our results indicate a complex microenvironment in cyst fluid, where both protein content and pH levels play a role. It's observed that a lower pH value correlates with a lower APTw value.Conclusion
In conclusion, APTw technology, as a molecular-level, non-invasive MR imaging technology, can accurately reflect the differences in MTRasym (3.5 ppm) values between normal ovarian tissue and pathological ovarian tissue. Furthermore, it has high value in the differential diagnosis of common ovarian cystic and predominantly cystic lesions.Acknowledgements
None.References
[1] Reinhold C, Rockall A, Sadowski E A, et al. Ovarian-Adnexal Reporting Lexicon for MRI: A White Paper of the ACR Ovarian-Adnexal Reporting and Data Systems MRI Committee[J]. J Am Coll Radiol, 2021, 18(5): 713-729.
[2] Vandecaveye V, Dresen R, De Keyzer F. Novel imaging techniques in gynaecological cancer[J]. Curr Opin Oncol, 2017, 29(5): 335-342.
[3] Sadowski E A, Bennett L K, Chan M R, et al. Nephrogenic systemic fibrosis: risk factors and incidence estimation[J]. Radiology, 2007, 243(1): 148-57.
[4] Thomassin-Naggara I, Daraï E, Cuenod C A, et al. Contribution of diffusion-weighted MR imaging for predicting benignity of complex adnexal masses[J]. Eur Radiol, 2009, 19(6): 1544-52.
[5] Pankowska A, Kochalska K, Łazorczyk A, et al. Chemical exchange saturation transfer (CEST) as a new method of signal obtainment in magnetic resonance molecular imaging in clinical and research practice[J]. Pol J Radiol, 2019, 84: e147-e152
[6] Jones K M, Pollard A C, Pagel M D. Clinical applications of chemical exchange saturation transfer (CEST) MRI[J]. J Magn Reson Imaging, 2018, 47(1): 11-27.
[7] Ishimatsu K, Nishie A, Takayama Y, et al. Amide proton transfer imaging for differentiating benign ovarian cystic lesions: Potential of first time right[J]. Eur J Radiol, 2019, 120: 108656.
Figures
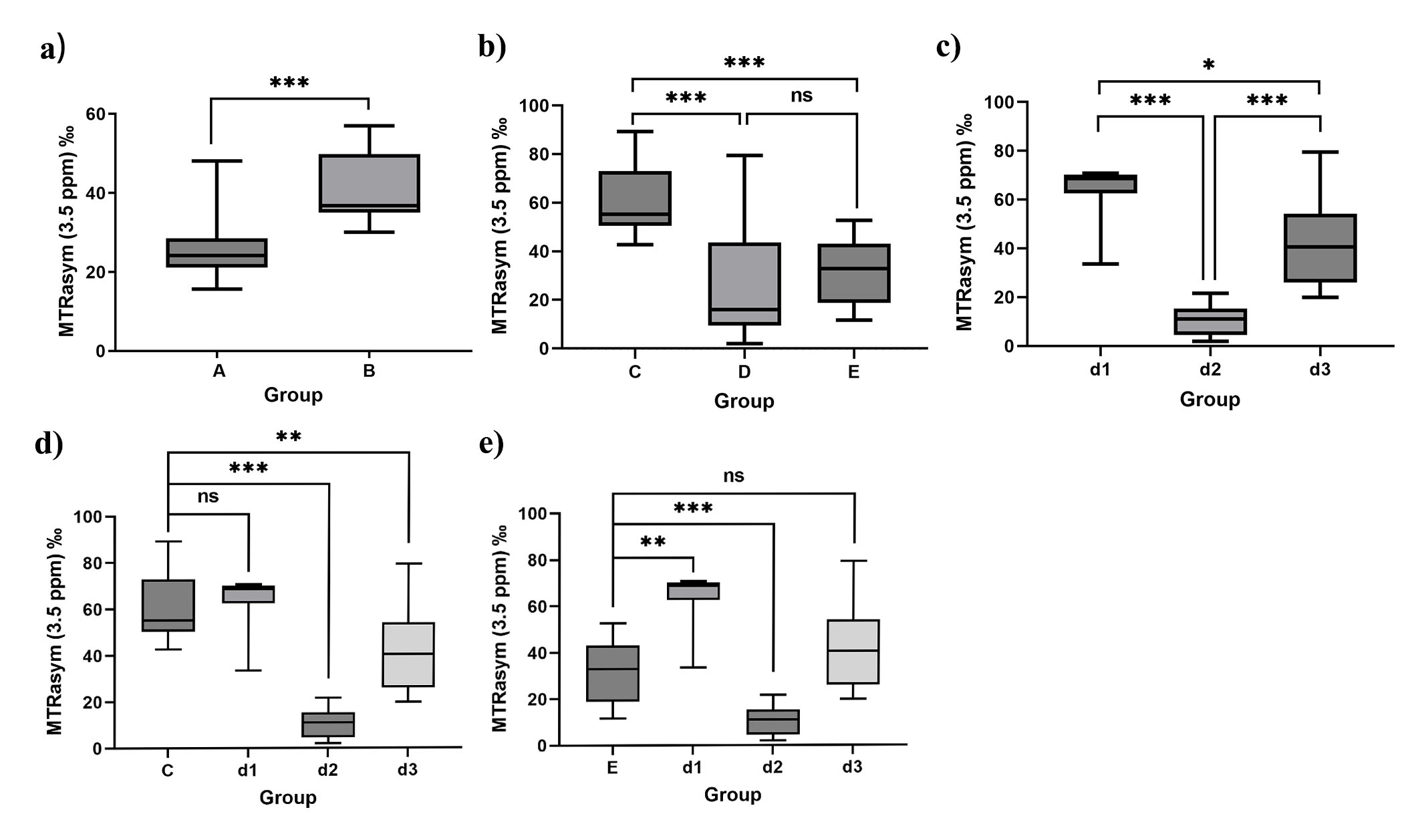
Figure 3:
a) Distribution of MTRasym (3.5 ppm) values in the solid components of Groups A and B. b-c) Distribution of MTRasym (3.5 ppm) values in the cystic components of Groups C, D, E, d1, d2, and d3.d-e) Distribution of MTRasym (3.5 ppm) values in the cystic components of Groups C, d1, d2, d3, and E. All data are expressed as mean ± standard deviation and a,d,e tested by independent-samples t-test and b,c tested by one-way ANOVA.
'ns' indicates that p > 0.05 is not statistically significant, *p < 0.05, **p < 0.01, ***p < 0.001.