4298
Investigating the Feasibility of Upright 0.5T MR Defaecating Proctography: initial results reveal potential for clinical assessments.1Sir Peter Mansfield Imaging Center, University of Nottingham, Nottingham, United Kingdom, 2Department of Radiology, Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom
Synopsis
Keywords: Pelvis, Low-Field MRI, Proctography, Pelvic floor disorder
Motivation: Pelvic floor assessments using X-ray proctography involve ionising radiation and only image the posterior compartment. Conventional supine-MR defaecography lacks in sensitivity as it fails to replicate the physiological position of defaecation. Upright-MR avoids ionising radiation and allows defaecography in sitting position whilst visualising all pelvic compartments.
Goal(s): To image defaecation using upright scanner with optimised acquisition and assess its feasibility for clinical defaecography.
Approach: Upright scanner with purpose-built commode coil and optimised HASTE acquisition were used to capture pelvic floor changes during defaecation in sitting position.
Results: Structural and functional images were satisfactory for qualitative and quantitative clinical assessments−performed by two experienced Radiologists.
Impact: Our upright 0.5T scanner with purpose-built RF commode coil and optimised HASTE acquisition will enable Radiologists to identify anatomical and functional abnormalities in pelvic floor disorders. The technique shows potential to be a compatible alternative to X-ray Proctography.
Introduction
Evacuation disorders, such as intussusception, rectocele, enterocele and pelvic organ prolapse severely limit the quality of life for many patients and nearly 50% of multiparous women aged more than 50 years are affected by pelvic floor disorders (PFD)1. Conventional clinical assessment uses either X-ray or MR-based defaecography. Fluoroscopic proctography (FP) consists of administration of barium contrast per-rectum and assessment of defaecation in the sitting position. Aside from its invasive nature, the poor soft-tissue contrast and exposure to ionising radiation, the technique is not ideal to obtain a full assessment of the pelvic floor. Conventional MR defaecating proctography (MRDP) mitigates these limitations and provides multiplanar, high soft-tissue-contrast anatomical information about the pelvic compartments1,2,3,4; however patients have to lie supine while defaecating, an abnormal and uncomfortable posture5. FP is more sensitive than MRDP in detecting rectal intussusception; the hypothesised reason being the more natural patient positioning, thus higher rates of complete or near-complete rectal emptying6.In this study, we use an Open 0.5T ASG scanner with purpose-built commode coil and optimised T2 acquisition protocol, to perform MRDP in the sitting position and investigate whether the acquired data can provide the conventional anatomical and functional metrices used for clinical PFD assessments, without the need for Gadolinium-based contrast administration into the vagina, urinary bladder or small bowel.
Methods
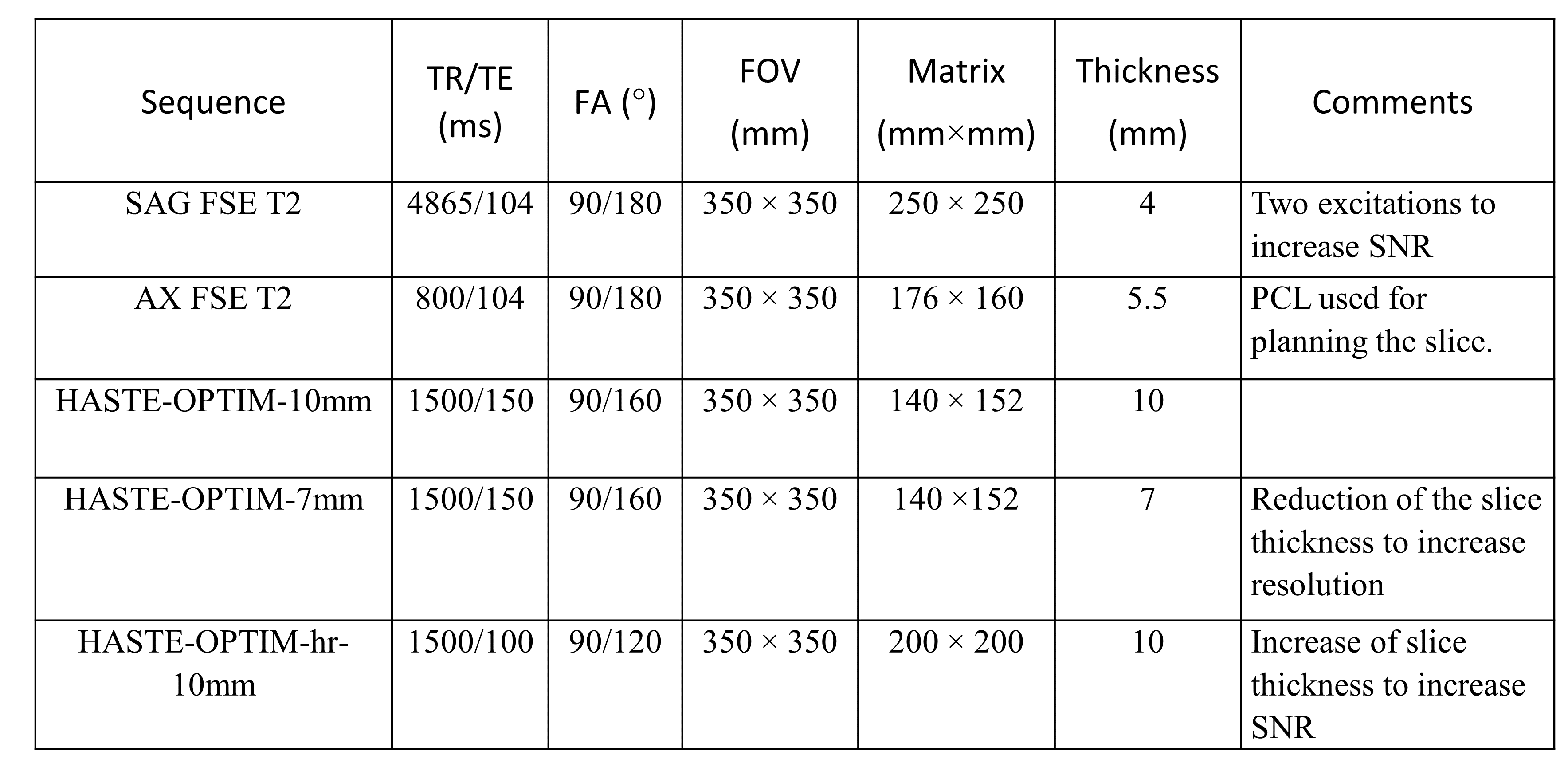
Three healthy participants (one male) with no history of pelvic floor or bowel abnormalities were scanned with 0.5T ASG Paramed Open MRI scanner at University of Nottingham, UK. A purpose-built, MR-compatible commode with an integrated RF coil provided coverage of the pelvis and lower back (Figure 1). The RF commode consisted of two single turn coils, arranged at 105o, with the horizontal coil being shaped to the outline of the bedpan cut-out moulding and the vertical coil being oblong with a small bend to null coupling. These coils were made from 4 mm diameter copper wire, tuned, and matched to 50 ohms for the built-in pre-amplifiers used.Baseline structural data were collected using sagittal and axial fast spin echo (FSE) sequence, while subjects were sitting on the commode coil. To optimise the dynamic acquisition protocol, several HASTE sequences were run before rectal preparation whilst participants were asked to mimic Kegel manoeuvres. An experienced Radiologist then selected the dynamic sequence with suitable contrast and resolution for the subsequent off-line anatomical and functional analysis (Table 1).
After filling of the rectum with 120 ml ultrasound gel, subjects were asked to reseat on the commode coil, in complete privacy. Dynamic data were collected while participants performed Kegel manoeuvres expelling the gel under Radiologist's instructions (i.e., 'rest', 'clench', ‘push’) (Figure 2, gif).
Results
Static and dynamic data were assessed by two Radiologists (CC, RM) with 8 and 4 years of clinical proctography experience.The static images from all subjects had appropriate contrast and resolution to locate/delineate the pubococcygeal line (PCL), H- and M-line, and all organ-specific reference points in the anterior, middle, and posterior compartments (Figure 3).
The dynamic images show normal appearance of pelvic floor level for all subjects. Anorectal angle (ARA) was measured during rest, squeezing, and defaecation (Figure 4). For all subjects, image qualities were satisfactory for the Radiologists to calculate ARAs. At initiation of defaecation, increase in intra-abdominal pressure was visible with downward motion of pelvic floor and widening of ARA. Defaecation was visible with the relaxation of anal sphincter complex along with further ARA widening (within normal range of 15-20°)2.
Discussion
Seated, T2-weighted, static and cine imaging on an Open 0.5T MR system allows reliable extraction of anatomical and functional metrics for MRDP while allowing patients to undertake defaecation in a normal posture.The static images allow clear identification of PCL, H- and M-line from all healthy subjects. These can be used to assess the pelvic floor and aid as reference lines for quantifying the degree of pelvic organ prolapse in each compartment. Our dynamic scans provide ARAs that are within the range prescribed for a normal pelvic floor1,2.
Conclusion
This preliminary data suggests that upright 0.5T MRI with experimental protocol using optimised static and cine T2-weighted sequences, a purpose-built RF commode coil provides satisfactory anatomical and functional measurements of the healthy pelvic floor.We now aim to recruit patients with PFDs and investigate whether MR upright proctography is comparable or superior to supine MRDP or fluoroscopic proctography. This will establish whether upright MRDP can enable Radiologists to perform conventional visual assessments of the PV anatomy/landmarks as well as quantify surrogate metrices (ARA, PCL-line, etc) required to grade PVD, whilst the patient is in a natural defaecating position.
Acknowledgements
We acknowledge "EPSRC grant : Realising the potential of open MRI for dynamic studies of human anatomy and function (RIS1648604)" for funding this study. Big thanks to colleague Arthur Harrison who has actively helped to find research participants.References
1. Maccioni F, Alt CD. MRI of the Pelvic Floor and MR Defecography. In: Hodler J, Kubik-Huch RA, von Schulthess GK, eds. Diseases of the Abdomen and Pelvis 2018-2021: Diagnostic Imaging - IDKD Book. Cham: Springer International Publishing; 2018:13-20.
2. Revels JW, Mansoori B, Fadl S, et al. MR Defecating Proctography with Emphasis on Posterior Compartment Disorders. Radiographics. 2023;43(1):e220119.
3. Pilkington SA, Nugent KP, Brenner J, Harris S, Clarke A, Lamparelli M, Thomas C, Tarver D. Barium proctography vs magnetic resonance proctography for pelvic floor disorders: a comparative study. Colorectal Dis. 2012;14(10):1224-1230.
4. Korula DR, Chandramohan A, John R, Eapen A. Barium Defecating Proctography and Dynamic Magnetic Resonance Proctography: Their Role and Patient's Perception. J Clin Imaging Sci. 2021;11:31.
5. Rao SS, Kavlock R, Rao S. Influence of body position and stool characteristics on defecation in humans. Am J Gastroenterol. 2006;101(12):2790-2796.
6. Grossi U, Di Tanna GL, Heinrich H, Taylor SA, Knowles CH, Scott SM. Systematic review with meta-analysis: defecography should be a first-line diagnostic modality in patients with refractory constipation. Aliment Pharmacol Ther. 2018;48(11-12):1186-1201.
Figures
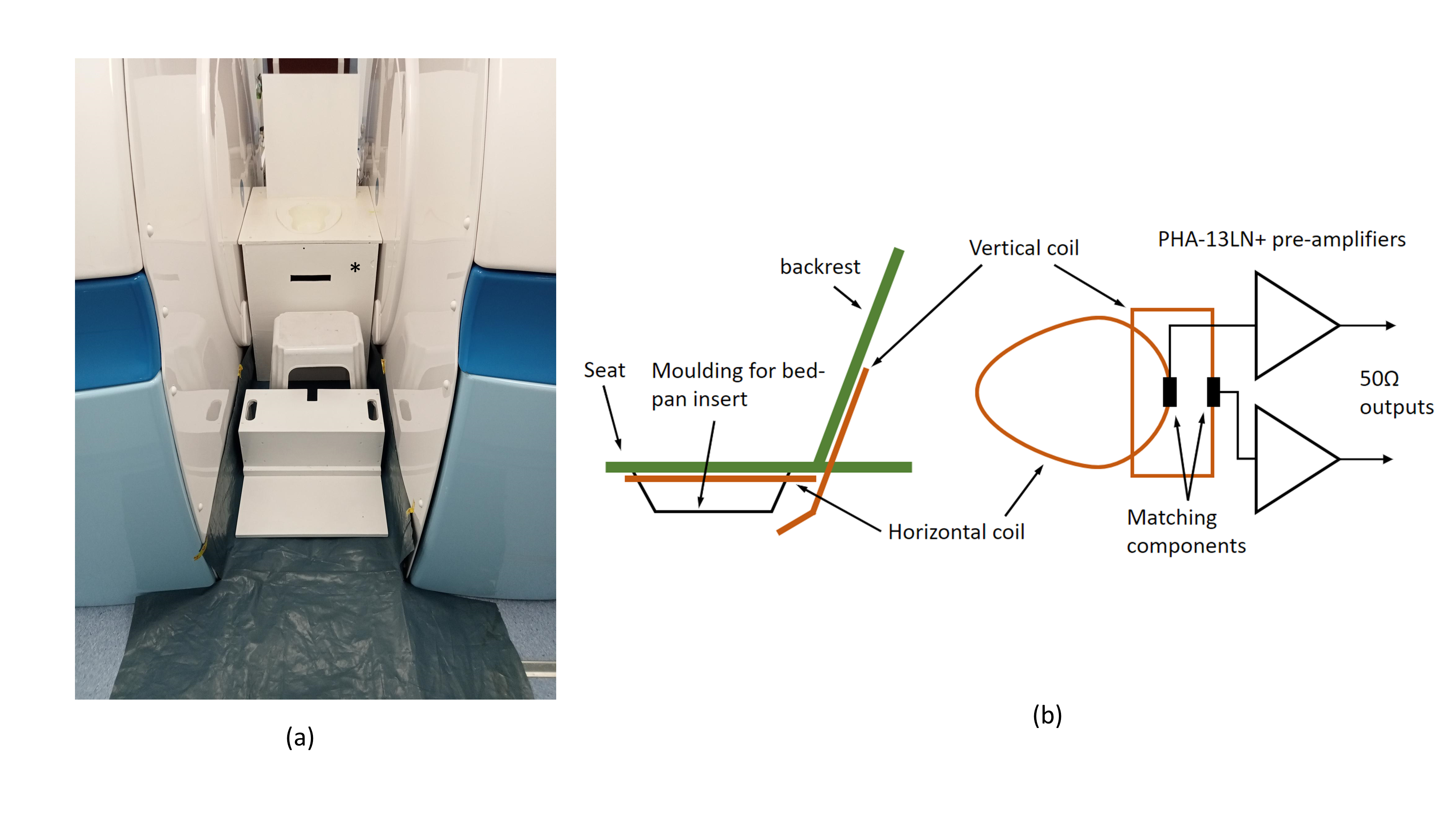
Figure 1(a): Setting in the 0.5T scanner with purpose-built RF commode coil (marked with *) (b): Schematic of commode coil for targeted coverage across the pelvic floor and lower back.

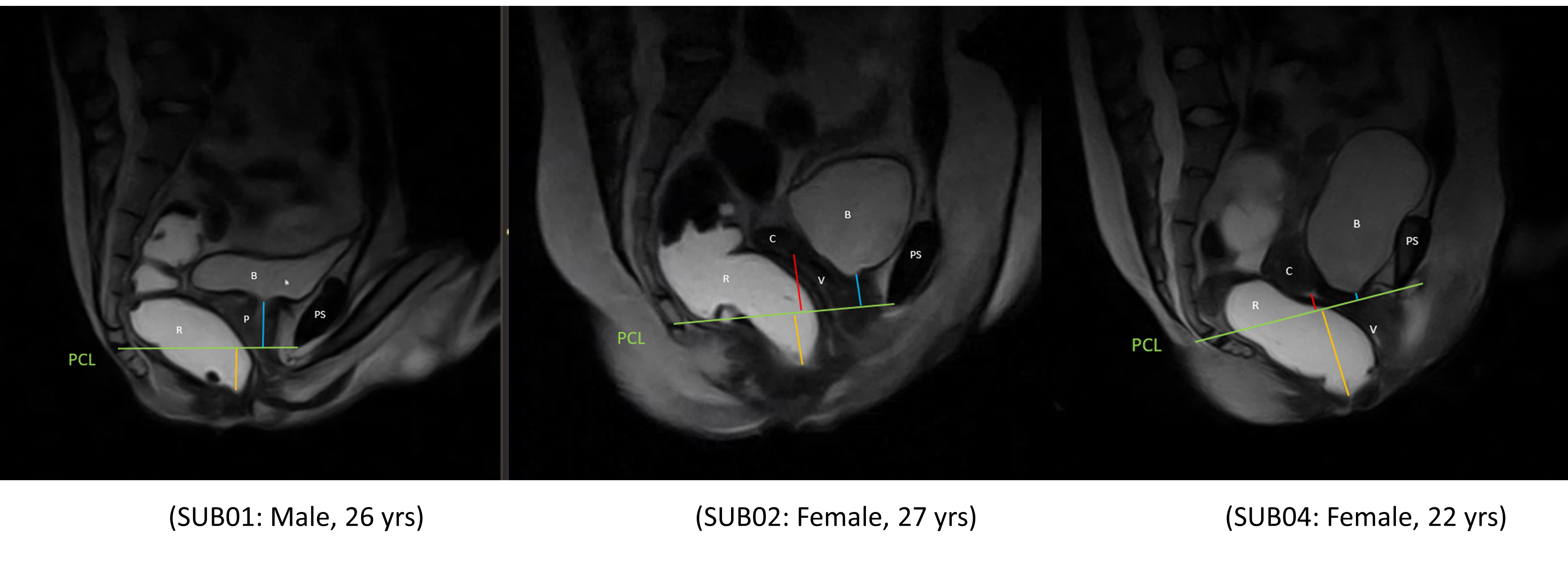
Figure 3: Presentation of the metric measurements at rest (after filling rectum with ultrasound gel) for one male and two females with sagittal T2-FSE sequence. Reference points are marked using the pubococcygeal line (PCL, in green). All organ-specific reference points were seen. Figure shows the location of rectum (R), pubic symphysis (PS), bladder (B), vagina (v), the pouch of Douglas (P), cervix (C). The descent of levator plate (M-line, blue line), the length of the hiatus (H-line, yellow line) and the distance to anterior cervical lip (red line) can also be identified clearly.
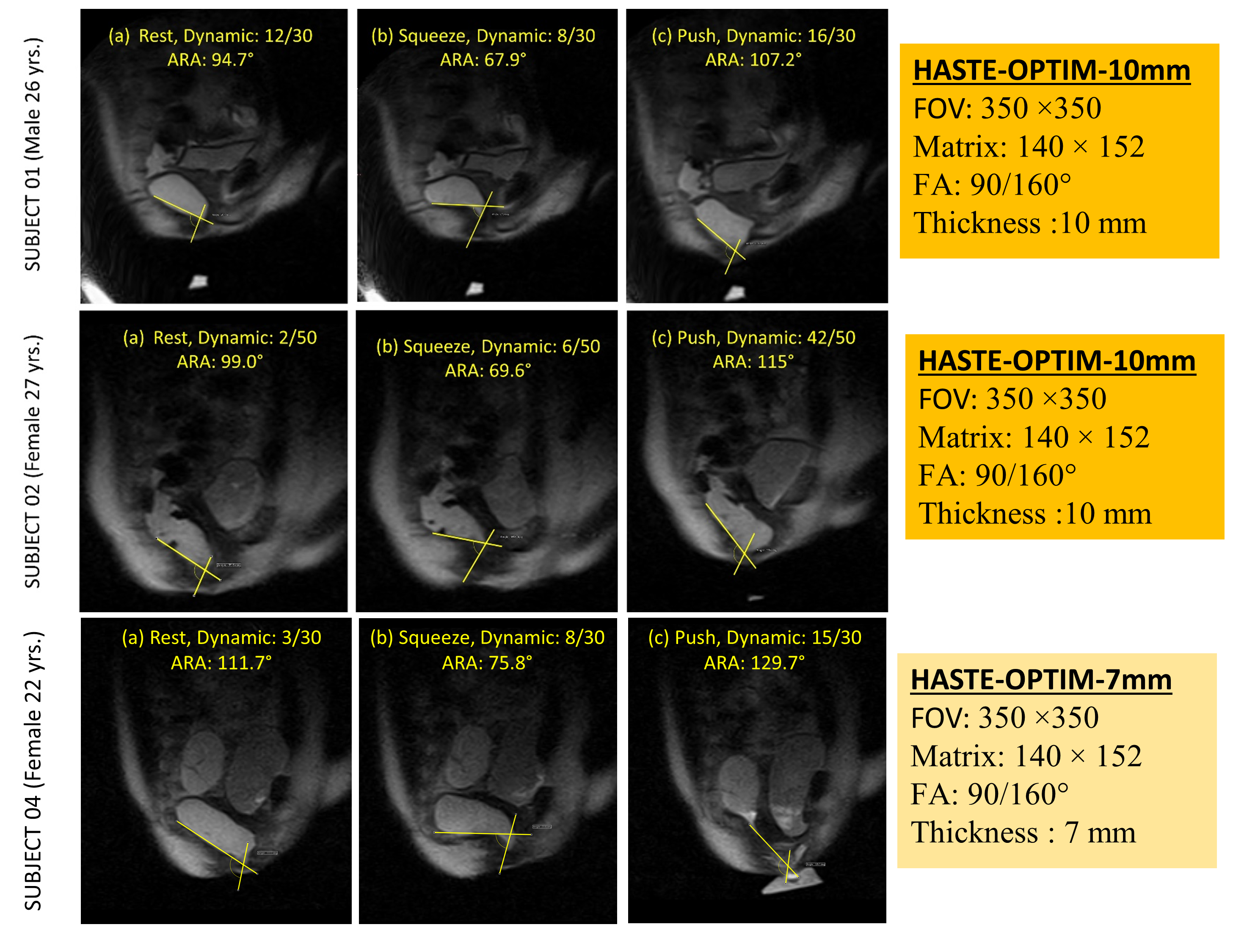
Figure 4: Sagittal T2-weighted dynamic image after rectal filling with ultrasound gel showing anorectal angle (ARA) at different stages of defaecation for one male and two females subjects with no pelvic floor disorder (age: 26,27,and 22 yrs, respectively) along with the image acquisition parameters.