4297
The Influence of Pelvic Configuration on Pelvic Organ Prolapse in Females of All Ages1The First Central Clinical School, Tianjin Medical University, Nankai District, Tianjin, China, 2Department of Radiology, Tianjin First Central Hospital, School of Medicine, Nankai University, Tianjin, China
Synopsis
Keywords: Pelvis, Prevention, MR imaging;pelvimetry
Motivation: Pelvic organ prolapse(POP) is a common disease in women, and pelvic geometry is one of the influencing factors.
Goal(s): To compare pelvic dimensions in women between diagnosed with POP and control group encompassing all age groups.
Approach: 130 patients with POP and equal women without any pelvic floor dysfunction were retrospectively enrolled.After excluding collinearity, pelvic measurement parameters were included in univariate and multivariate logistic regression to screen independent risk factors, and finally demographic parameters were included to verify their independence.
Results: Pelvic geometry has a role in the incidence of POP, and that having a large pelvis increases the risk of POP.
Impact: A large pelvis is one of the risk factors for POP, which are expected to play a warning role in early prevention in clinical work and are not affected by clinical factors.
Purpose
Pelvic organ prolapse (POP) refers to alterations in pelvic organ anatomical position and physiological abnormalities caused by degeneration and damage of pelvic floor support structures. POP has a negative impact on women’s quality of life and their physical and mental health; it will become an major global public health issue. [1,2]Pelvis is an important anatomic structure that supports the pelvic floor structure and pelvic organs. There is increasing evidence that the size and shape of the pelvis can affect the course of vaginal delivery and the attachment position of muscles and ligaments, resulting in the damage to pelvic floor soft tissues and nerves during delivery or under long-term gravity, which may lead to the occurrence of POP over time, and a larger pelvis was associated with a higher risk of developing POP. [3-5]
In this study, we retrospectively compared pelvic dimension in women with POP to a normal group of women of all ages to ensure the association between pelvic configuration and POP.
Methods
We recruited 130 patients with POP (age 21-82) who were confirmed by pelvic organ prolapse quantitation (POP-Q) for clinical diagnosis and 130 normal women (age 23-89) as the control group. Their demographic data included their age, body mass index (BMI), parity, and menopause.MRI examination was performed on a 3.0T MRI scanner (Ingenia, Philips Healthcare) with a 16-channel phased-array body coil. Sagittal, coronal and axial pelvis T2W images (TR 4381ms, TE 101ms, slice thickness 5mm) were acquired. Based on MR images, the following parameters were measured: the diameter of the transverse inlet, bispinous diameter, bituberous diameter, pelvic inclination, anterior angle, anatomic conjugate, obstetric conjugate, diagonal conjugate, anteroposterior diameter of mid plane, anteroposterior diameter of lower mid plane, sagittal outlet, coccygeal curved length, ratio of sacrococcyx, the area of left and right obturator internus muscles and the area of anterior and posterior pelvic area (Figure 1).The statistical analysis was conducted using R statistical software, version 4.3 (R Foundation for Statistical Computing, Vienna, Austria), and SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Demographics and measurement data were presented by Student’s t test for continuous variables, Mann-Whitney U-test for nonparametric variables and Chi-squared test for nominal data. After the collinearity problem solve by step-by-step regression and variance inflation, logistic regression analysis was used to avoid over-fitting. Following an analysis of the correlation between the imaging parameters and the demographic variables as confounding factors, several confounding factors were included to establish the model.In addition, to ensure the repeatability of the parameters, 30 cases were chosen randomly from the data two months after the first measurement by the same physician using a simple random sampling method in order to verify the repeatability of the parameters. The intra-group correlation coefficient (ICC) was used for evaluation. 0.75≤ICC≤1.00 was considered as good consistency.Results
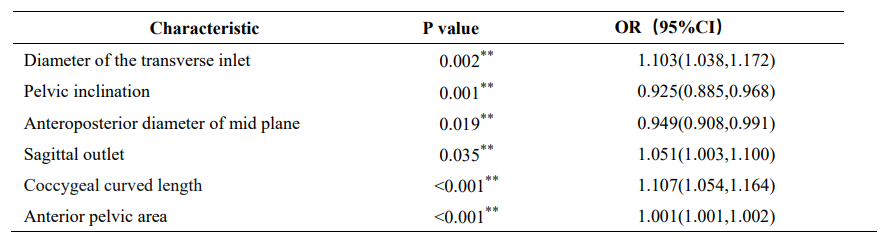
Good interobserver reliability was found. After analysing the demographic characteristics and imaging parameters of the two groups, POP group had higher BMI, transverse inlet diameter, bispinous diameter, bituberous diameter, anterior angle, anteroposterior diameter of lower mid plane, sagittal outlet, coccygeal curved length, anterior and posterior pelvic area than those in normal group (P < 0.05). Pelvic inclination was decreased in the POP group compared to the normal group (P < 0.05) (Table 1). After multiple collinearity test for the imaging measurement variables, we deleted anatomic conjugate and obstetric conjugate, and performed univariate regression on the remaining variables, and the results were consistent with the difference analysis (Table 2). Multivariate logistic regression was performed after excluding collinearity for statistically significant parameters again. The results showed that as an independent risk factor for POP in women was positively correlated with the larger the diameter of the transverse inlet (OR:1.10; p=0.02), the sagittal outlet (OR:1.05; p=0.04), the coccygeal curved length (OR:1.11; p<0.01), the anterior pelvic area (OR:1.00; p<0.01), the smaller the anteroposterior diameter of mid plane (OR:0.95; p=0.02), the pelvic inclination (OR:0.93; p=0.01), the higher the risk of POP (Table 3). Adding demographic factors as covariates did not change the aforementioned parameters' statistical significance. (Figure 2).Conclusion
Regardless of age, BMI, parity, and menopausal status, patients with POP have higher transverse inlet diameter, sagittal outlet, coccygeal curvature length, and anterior pelvic area, as well as smaller pelvic inclination and anteroposterior diameter of mid plane.Acknowledgements
None.References
1. Raju R, Linder BJ. Evaluation and Management of Pelvic Organ Prolapse[J]. Mayo Clin Proc, 2021, 96(12):3122-3129. DOI:10.1016/j.mayocp.2021.09.005.2. Pang H, Zhang L, Han S, et al. A nationwide population-based survey on the prevalence and risk factors of symptomatic pelvic organ prolapse in adult women in China - a pelvic organ prolapse quantification system-based study[J]. BJOG, 2021, 128(8):1313-1323. DOI:10.1111/1471-0528.16675.
3. Pavličev M, Romero R, Mitteroecker P. Evolution of the human pelvis and obstructed labor: new explanations of an old obstetrical dilemma[J]. Am J Obstet Gynecol, 2020, 222(1):3-16. DOI:10.1016/j.ajog.2019.06.043.
4. Delancey JO, Kane Low L, Miller JM, et al. Graphic integration of causal factors of pelvic floor disorders: an integrated life span model[J]. Am J Obstet Gynecol, 2008, 199(6):610.e1-610.e6105. DOI:10.1016/j.ajog.2008.04.001.
5. Brown KM, Handa VL, Macura KJ, et al. Three-dimensional shape differences in the bony pelvis of women with pelvic floor disorders[J]. Int Urogynecol J, 2013, 24(3):431-439. DOI:10.1007/s00192-012-1876-y.
Figures
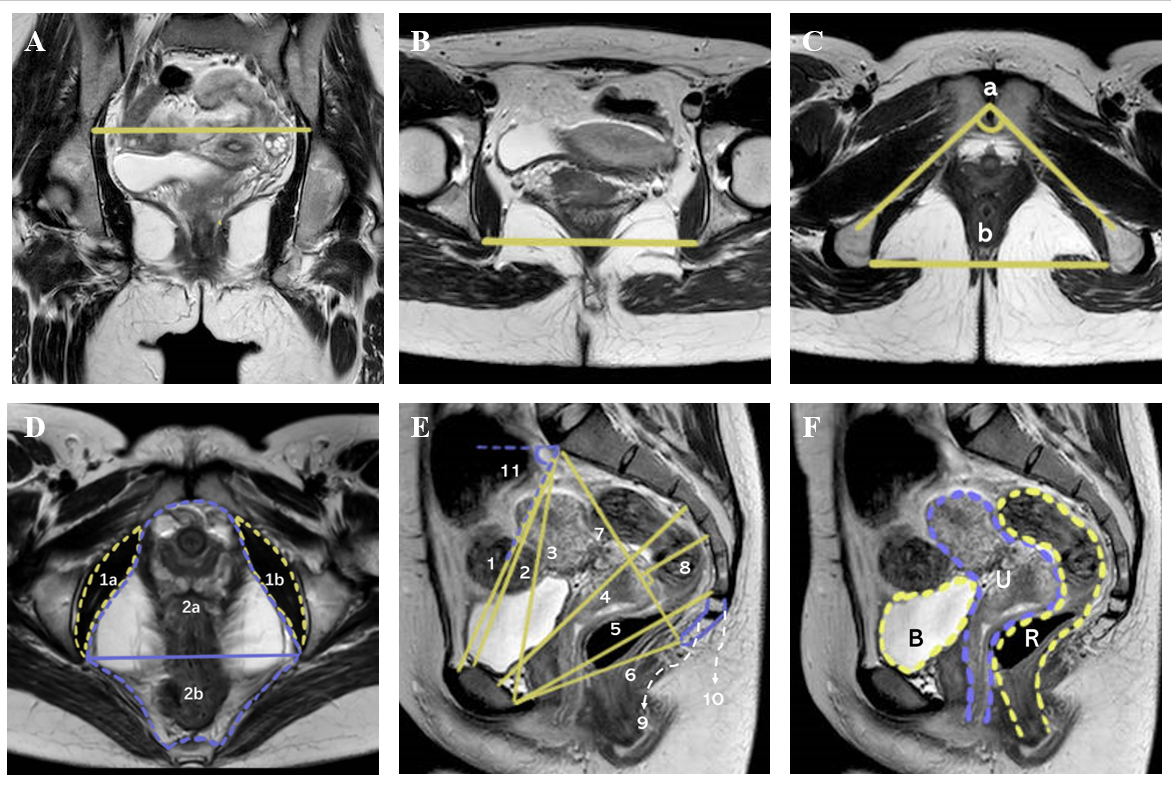
Figuer 1:A:Diameter of the transverse inlet;B:Bispinous diameter;C:a:Anterior angle; b:Bispinous diameter;D:1a:Obturator internus muscle(right);1b:Obturator internus muscle(left);2a:Anterior pelvic area;2b:Posterior pelvic area;E:1:Anatomic conjugate;2:Obstetric conjugate;3:Diagonal conjugate;4:Anteroposterior diameter of mid plane;5:Anteroposterior diameter of lower mid plane;6:Sagittal outlet;7:Depth of the sacral curvature 8:Coccygeal curved length;(9+10)/2:Sacrococcygeal length;11:Pelvic inclination;F:B:bladder;U:uterus;R:rectum
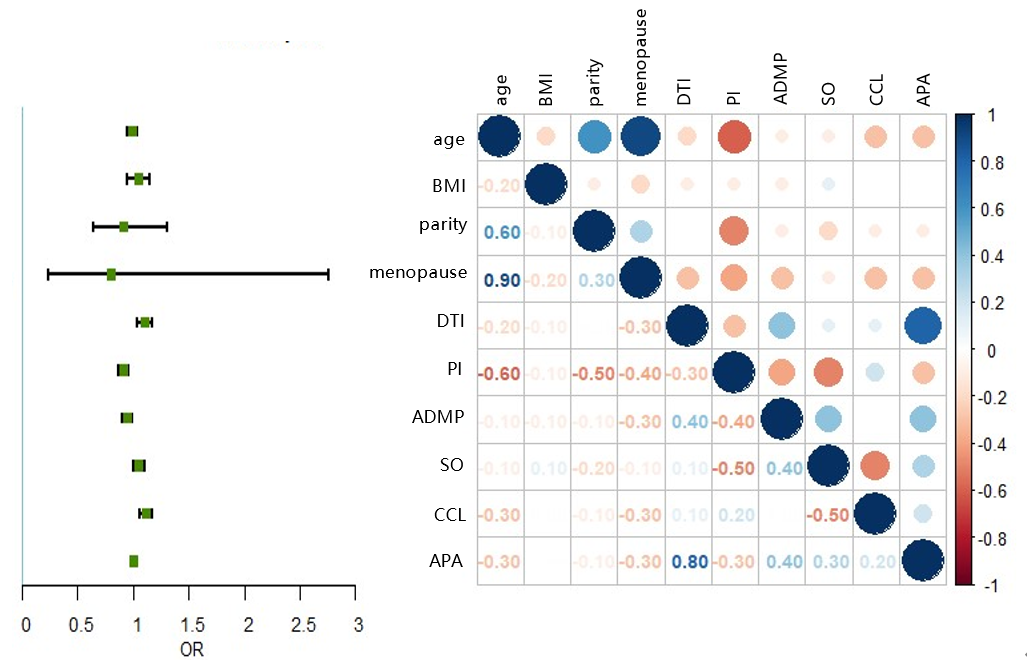
Figuer 2:BMI Body mass index, DTI Diameter of the transverse inlet, PI Pelvic inclination, ADMP Anteroposterior diameter of mid plane, SO Sagittal outlet, CCL Coccygeal curved length, APA Anterior pelvic area
It shows the forest(left) and correlation(right) plot
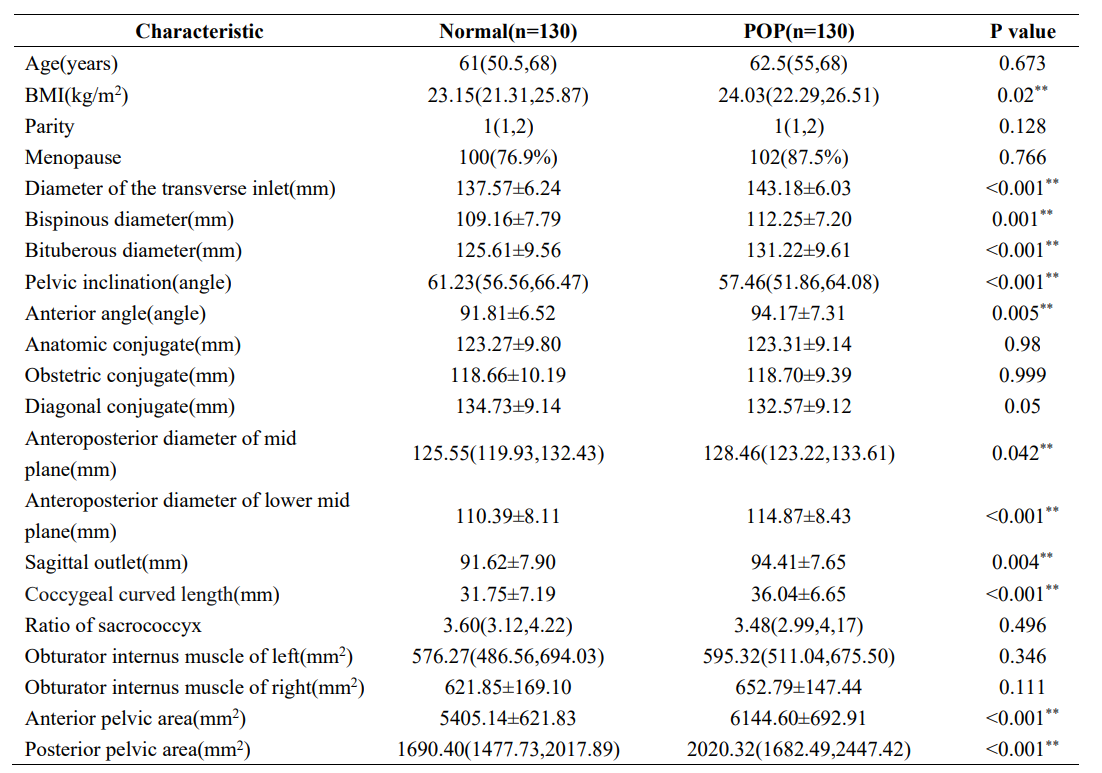
Table 1:Continuous variables given as mean ± standard deviation, nonparametric variables as median (interquartile range), categorical variables as numbers (percentages, %) Between-group comparisons were analyzed by independent sample Student’s t test (continuous data), Wilcoxon rank-sum test and by Chi-squared test (categorical data) POP pelvic organ prolapse, BMI body mass index;** significative results
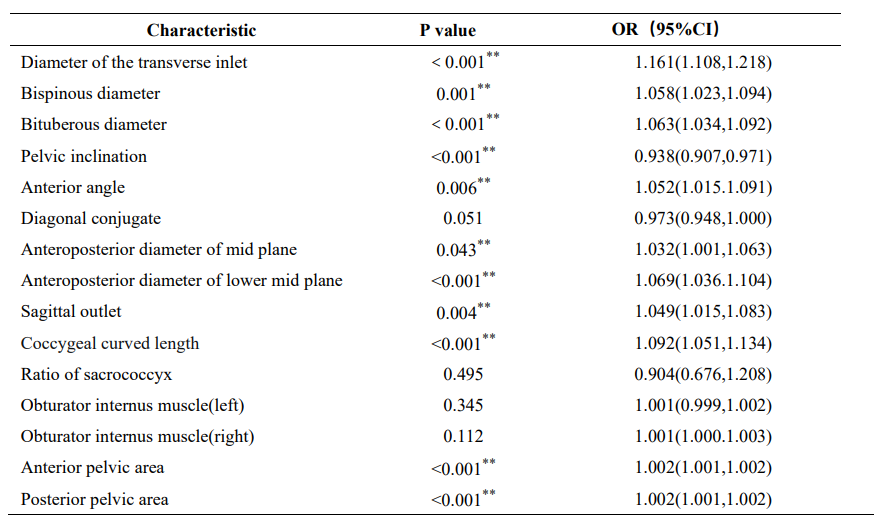
Table 2:OR odds ratio;** significative results.