4296
Usages of Half Fourier single shot turbo spin echo with deep learning reconstruction and variable flip angle in gynecology1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, kyoto, Japan, 2Department of Radiology, Toyama University, Toyama, Japan, 3School of Pharmaceutical Sciences, Wakayama Medical University, Wakayama, Japan, 4Real World Data Research and Development, Kyoto University Graduate School of Medicine, kyoto, Japan, 5Department of Biomedical Statistics and Bioinformatics, Kyoto University Graduate School of Medicine, kyoto, Japan, 6Department of Gynecology and Obstetrics, Kyoto University Graduate School of Medicine, kyoto, Japan
Synopsis
Keywords: Pelvis, Uterus
Motivation: Without antispasmodics, obtaining T2-weighted images with robustness to artifacts and high tissue contrast is challenging in gynecologic MRI.
Goal(s): Our goals were to investigate HASTE with deep learning-reconstruction and a variable flip angle technique (iHASTE) outperforming conventional sequences without antispasmodics, and to explore its clinical usages.
Approach: The comparison between iHASTE, HASTE, and BLADE without antispasmodics, and the comparison between iHASTE without antispasmodics and TSE with antispasmodics, were performed.
Results: Without antispasmodics, iHASTE outperformed HASTE and BLADE. Compared with TSE with antispasmodics, iHASTE was superior in the robustness to artifact, although inferior in overall imaging quality.
Impact: In gynecologic MRI, HASTE with deep learning-reconstruction and a variable flip angle technique could be clinically the first choice when antispasmodics are unavailable. Even with antispasmodics, it could back up deteriorated TSE via artifacts, for its robustness and rapidity.
Purpose
When antispasmodics are unavailable, BLADE or half Fourier single shot turbo spin echo (HASTE) have been clinically used in gynecologic MRI. But their imaging qualities are limited, compared to T2-weighted Turbo Spin Echo (TSE) with antispasmodics. Also, even when antispasmodics are available, TSE images are sometimes affected by artifacts, and the rapid backup sequence could be clinically helpful. The purposes of the study were to develop improved HASTE with deep learning (DL)-reconstruction and variable flip angle (iHASTE) outperforming conventional sequences without antispasmodics, and to explore its clinical usages when antispasmodics are available and when unavailable.Materials and methods
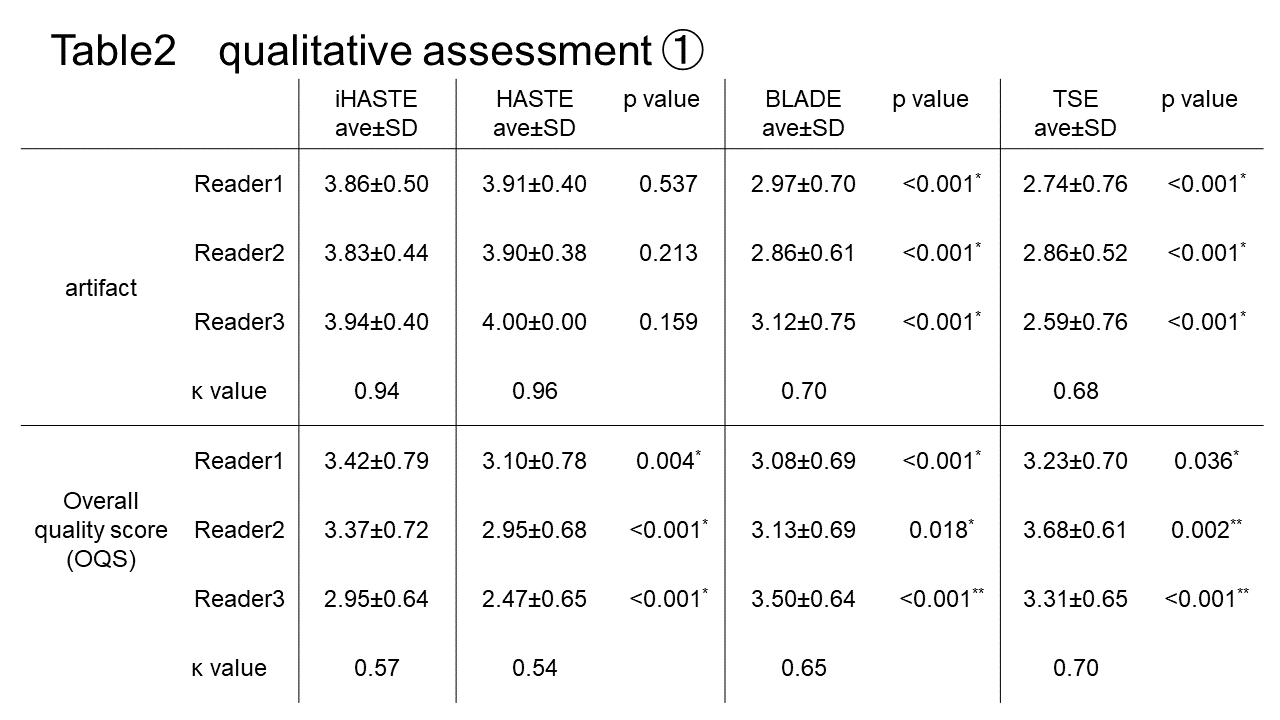
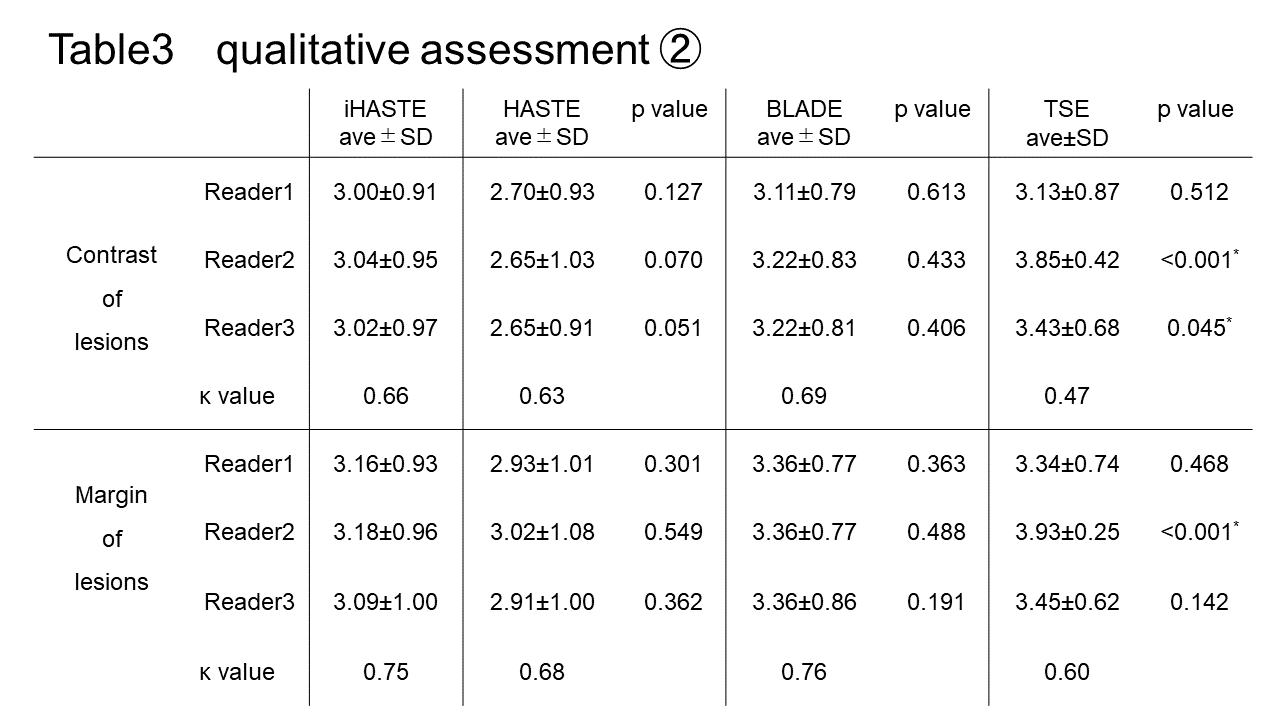
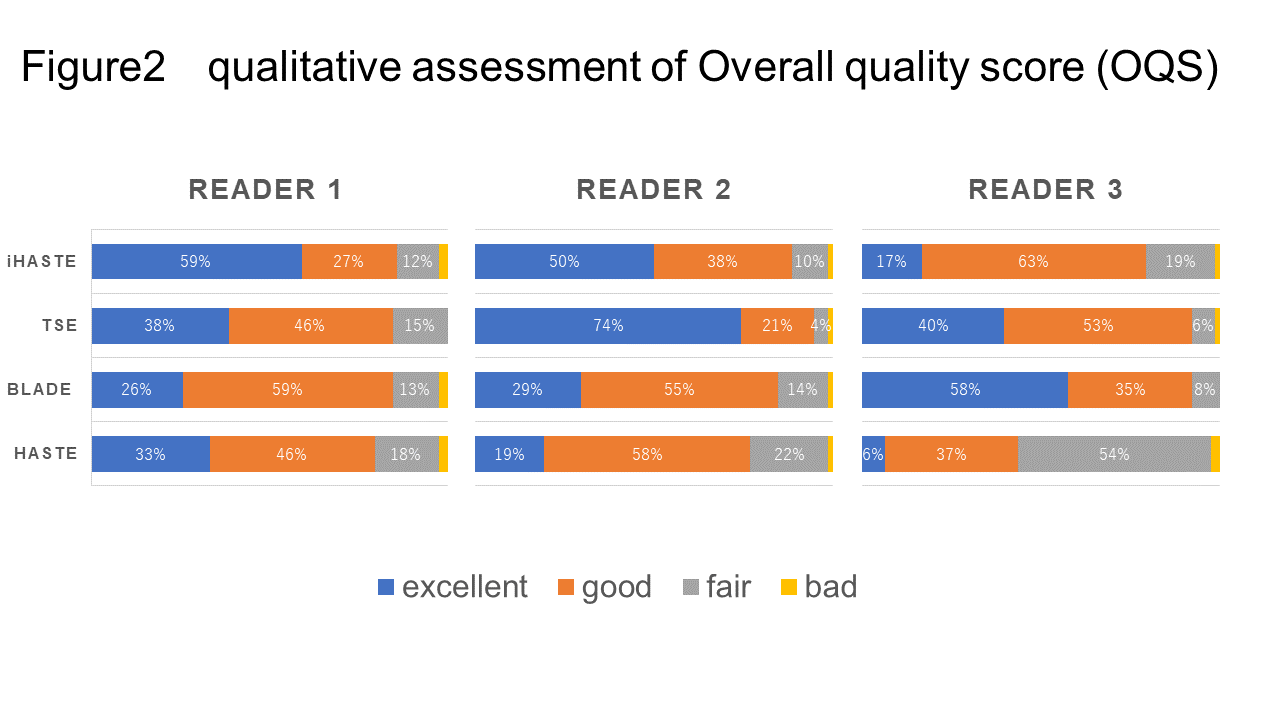
This retrospective study constituted two patient cohorts. The cohort without antispasmodics included 79 patients who underwent clinically indicated gynecologic MRI with sagittal iHASTE, HASTE, and BLADE between November 2021 and December 2022. The cohort with antispasmodics included 79 patients, matched to the cohort without antispasmodics based on their ages and diseases, among patients with TSE with antispasmodics during the same period.The research sequence iHASTE comprises two techniques: DL-reconstruction for enhanced image quality and resolution and a variable flip angle approach to improve tissue contrast.The qualitative and quantitative evaluations of the two patient cohorts were performed by radiologists expertized to gynecologic imaging. First, three radiologists with 15 year-, 16 year-, and 25 year-experience in gynecologic imaging independently evaluated the sagittal iHASTE, HASTE and BLADE of the cohort without antispasmodics, and sagittal TSE of the cohort with antispasmodics: overall quality and robustness to artifacts in all patients; tissue contrast of lesions in patients with leiomyoma/adenomyosis/uterine malignancy; margin of lesions in patients with leiomyoma/uterine malignancy. A Likert scale of 1–4 was used: 1, bad; 2, fair; 3, good; 4, excellent.Next, quantitative evaluations of tissue contrast in 34 cases with leiomyoma and 10 cases with uterus cancer (corpus or cervical cancer) was performed by a radiologist with 6-year experience. Using the signal intensity of the lesion (SIL), uterus tissue (myometrium or cervical stroma) (SIU), and subcutaneous fat (SIF), measured by a circular Region-of-interest (ROI) in each sequence, the normalized tissue contrast (normalized TC) was calculated by the following formula.TC = |SIL - SIU| / SIFThe statistical analyses below were performed. For the qualitative evaluations, the Wilcoxon signed rank test was used for the comparison of the three radiologists’ Likert scale evaluations. Weighted inter-rater agreements of them were assessed by Gwet’s AC2 (Gwet, 2014), a measure of inter-rater reliability for ordinal measurements. For the quantitative analyses, a paired t-test was used to compare iHASTE to HASTE/BLADE in the cohort without antispasmodics, and an unpaired t-test was used to compare iHASTE in the cohort without antispasmodics to TSE in the cohort with antispasmodics. A p value < 0.05 was considered statistically significant.Results and discussion
In evaluation of leiomyoma, the normalized TC of iHASTE (mean, 0.246) were significantly better than those of HASTE (mean, 0.190) and BLADE (mean, 0.202) (p < 0.001). And there was no significant difference between iHASTE and TSE (mean, 0.234). In evaluation of uterine malignancy, the normalized TC of iHASTE (mean, 0.189) were better than those of HASTE (mean, 0.144), BLADE (mean, 0.111), and TSE (mean, 0.147), although the difference was not significant.There was mostly good inter-observer agreement between the three radiologists. In assessment of artifacts, iHASTE was significantly better than BLADE and TSE. In assessment of overall quality, iHASTE was significantly better than HASTE. As for comparison between iHASTE and TSE, Reader 2 and 3 scored TSE significantly higher, while Reader 1 supported iHASTE. In the comparison between iHASTE and BLADE, Reader 1 and 2 scored iHASTE significantly higher, while Reader 3 supported BLADE. In the evaluation of contrast and margin of lesions, iHASTE had higher scores compared to HASTE, and lower scores compared to BLADE and TSE, but there were no significant differences.We explored the clinical utilities of iHASTE. Compared with HASTE and BLADE without antispasmodics, iHASTE showed the best overall quality. iHASTE could be the first choice when antispasmodics are not available. In the comparison of TSE with antispasmodics, although inferior to TSE in the overall quality, iHASTE was superior in the robustness to artifact. In the situation when antispasmodics are available, TSE should be the first choice as it has been. However, considering the non-negligible frequency of TSE of deterioration by artifact, iHASTE could work as a backup, leveraging its rapidity and robustness to artifact.Acknowledgements
No acknowledgement found.References
- Busse, R. F., et al. (2008). "Effects of refocusing flip angle modulation and view ordering in 3D fast spin echo." Magnetic Resonance in Medicine 60(3): 640-649.
- Fujimoto, K., et al. (2011). "BLADE acquisition method improves T2-weighted MR images of the female pelvis compared with a standard fast spin-echo sequence." European Journal of Radiology 80(3): 796-801.
- Herrmann, J., et al. (2021). "Development and Evaluation of Deep Learning-Accelerated Single-Breath-Hold Abdominal HASTE at 3 T Using Variable Refocusing Flip Angles." Investigative Radiology 56(10): 645-652.
- Saleh, M., et al. (2023). "A Feasibility Study on Deep Learning Reconstruction to Improve Image Quality With PROPELLER Acquisition in the Setting of T2-Weighted Gynecologic Pelvic Magnetic Resonance Imaging." Journal of Computer Assisted Tomography 47(5): 721-728.
- Tsuboyama, T., et al. (2022). "Impact of Deep Learning Reconstruction Combined With a Sharpening Filter on Single-Shot Fast Spin-Echo T2-Weighted Magnetic Resonance Imaging of the Uterus." Investigative Radiology 57(6): 379-386.
- Tsuboyama, T., et al. (2020). "Comparison of HASTE with multiple signal averaging versus conventional turbo spin echo sequence: a new option for T2-weighted MRI of the female pelvis." European Radiology 30(6): 3245-3253.
Figures
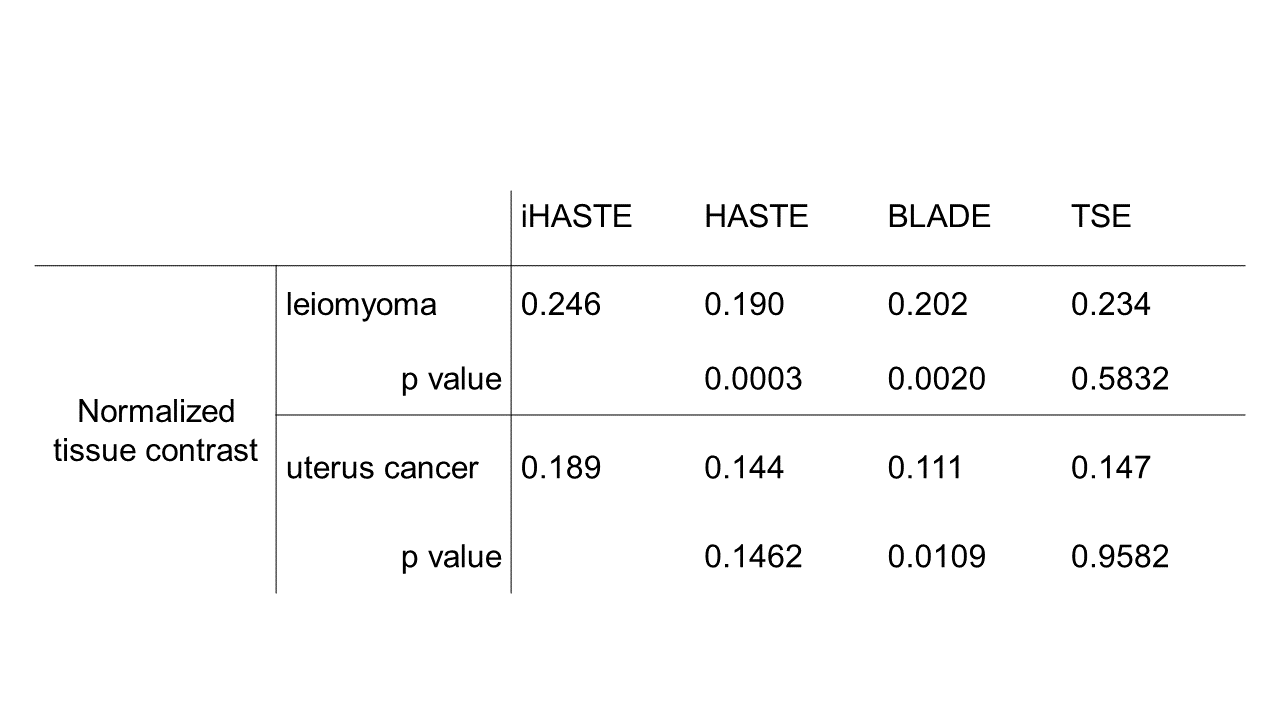
Table1 Quantitative evaluations of normalized tissue contrast (normalized TC) in the case with leiomyoma and uterus cancer (corpus or cervical cancer). The formula of normalized TC was TC = |SIL - SIU| / SIF*. In cases of leiomyoma, the mean Normalized TC of iHASTE was significantly higher than that of HASTE, BLADE,TSE. In cases with uterus cancer, no significant difference was found between the mean Normalized TC of each sequences.
*SIL: signal intensity of the lesion, SIU: signal intensity of uterus tissue (myometrium or cervical stroma), SIF: signal intensity of subcutaneous fat