4284
High Resolution MRI Protocol for Ovarian Cancer Screening1Radiology, University of California, San Diego, San Diego, CA, United States, 2Gynecology Oncology, University of California, San Diego, San Diego, CA, United States, 3Obstetrics, Gynecology, & Reproductive Sciences, University of California, San Diego, San Diego, CA, United States, 4Bioengineering, University of California, San Diego, San Diego, CA, United States
Synopsis
Keywords: Pelvis, Pelvis, Ovary, Diffusion
Motivation: Addressing the critical need for improved ovarian cancer detection, given its high mortality rate and limited screening options.
Goal(s): Explore diffusion properties of normal ovaries and lesions at high b-values (>1000 s/mm2 to develop a high-resolution ovarian cancer screening (OCS) protocol for average and high-risk individuals.
Approach: Utilized multishell diffusion-weighted MRI (DW-MRI) with simultaneous multi-slice excitation (Multiband) to capture high-resolution images in healthy, high-risk BRCA 1/2, and patients with potential cancer based on prior imaging.
Results: Distinct abnormal lesion types exhibited distinct contrasts at high b-values, with normal ovaries showing no signal, as expected.
Impact: Preliminary ovarian cancer MRI results with multishell DWI with Multiband, show promise in a new screening tool for ovarian cancer screening. This marks a significant step toward non-invasive screening advancements for high-risk individuals and early detection strategies.
INTRODUCTION:
Ovarian cancer ranks as the fifth-leading cause of cancer-related deaths among U.S. women, often presenting with metastasis (60%)1 and a 5-year survival rate of 28.9%2. Despite previous attempts3, routine screening is non-existent for average-risk women due to studies finding no mortality benefit with ultrasound and CA125. For high-risk BRCA1/2 individuals aged 35-40, standard of care includes prophylactic salpingo-oophorectomy, along with variable screening using ultrasound and CA125 before definitive treatment4-8. Early detection significantly improves the 5-year survival rate of ovarian cancer to 92.5%2, emphasizing the critical need for advancements and non-invasive strategies. High-resolution imaging modalities are required for high sensitivity, as the suspected site of initial disease for high risk patients is often the distal fallopian tube. Improved specificity is also key to minimize unnecessary surgeries for benign lesions.Diffusion-Weighted Imaging MRI (DW-MRI) is a non-contrast technique which has been used in several body applications, showing potential to distinguish between benign and malignant lesions. Though integrated into MR ovarian scoring systems like O-RADS9 and ADNEx MR10, the role of DW-MRI is limited due to the physiologic characteristics of premenopausal normal ovaries. Differentiation from cancer is challenging at standard imaging parameters (bmax = >1000 s/mm2), due to the increased cellularity and high diffusion signal of normal ovaries. Despite this, there is untapped potential for improving and utilizing DW-MRI in ovarian imaging.
The purpose of this study is to explore the diffusion properties of normal ovaries and abnormal lesions, providing preliminary insights toward developing a high-resolution OCS protocol. High-resolution high b-value (>1000 s/mm2) multishell DW-MRI will be explored using simultaneous multi-slice excitation (Multiband). This approach may address current challenges in DW-MRI applications while maintaining the essential components of a robust OCS protocol.
METHODS:
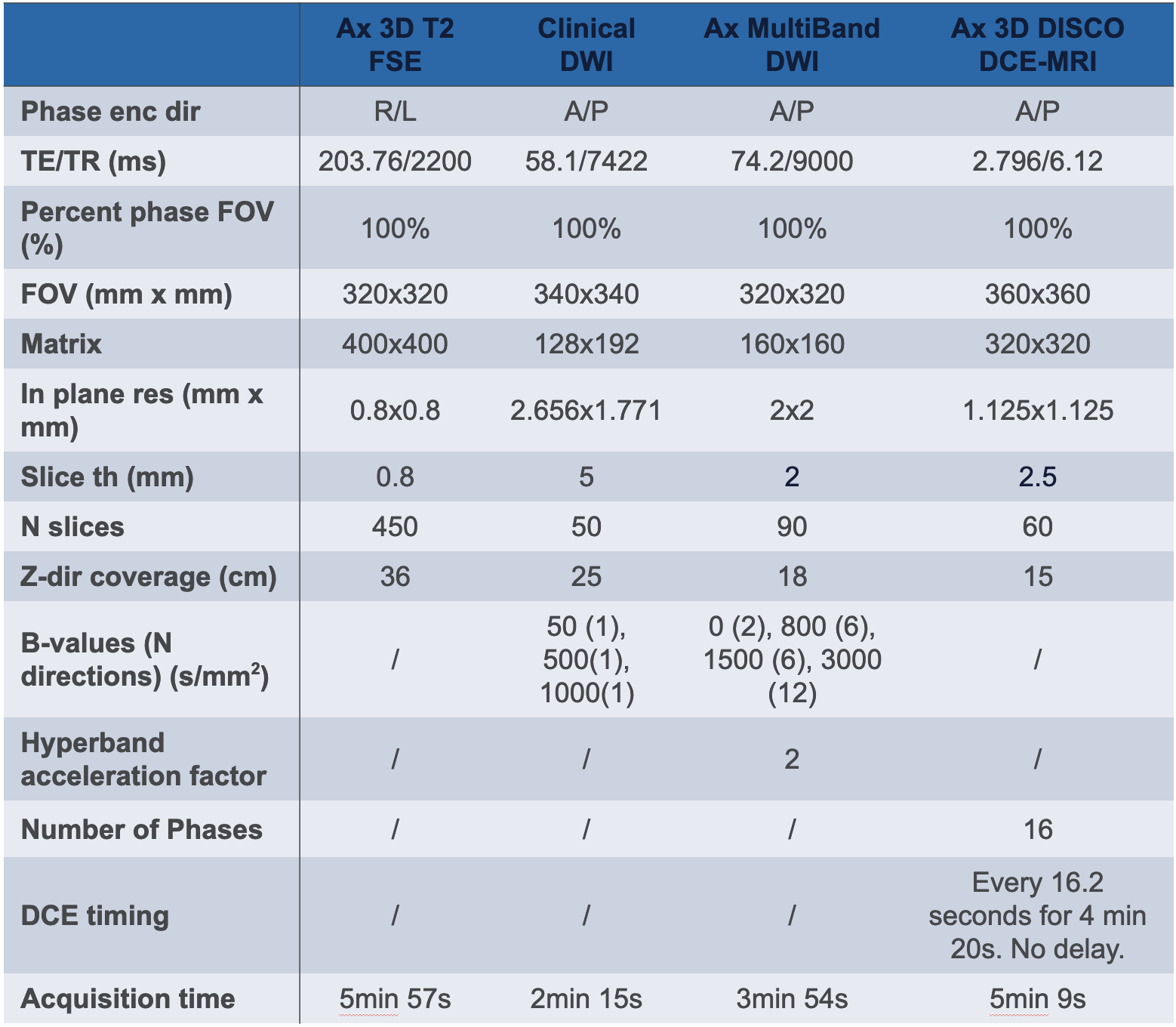
Four participants underwent scanning on a 3.0T scanner (GE Healthcare, USA) equipped with a 32-channel body coil. One was a healthy volunteer, one was a high-risk BRCA 1/2 patient scheduled for prophylactic oophorectomy, and the other two were patients with potential cancer based on previous imaging and examination. All sequences were concordant with American College of Radiology's (ACR) ovarian MRI guidelines11, but improvements were made to the DWI and T2 sequences to achieve high resolution (2mm isotropic and 0.8mm isotropic, respectively). These sequences were collected along with the clinical DWI (clinDWI) protocol at our institution (Table 1).Contrast-to-noise (CNR)12 was then calculated using the following equation:
$$CNR = \frac{m_x - m_y}{\sqrt{\frac{{sd_x^2+sd_y^2}}{2}}}$$
Where m is the mean signal intensity and sd is the standard deviation of the signal intensity. x represents the lesion while y is the muscle tissue region.
RESULTS:
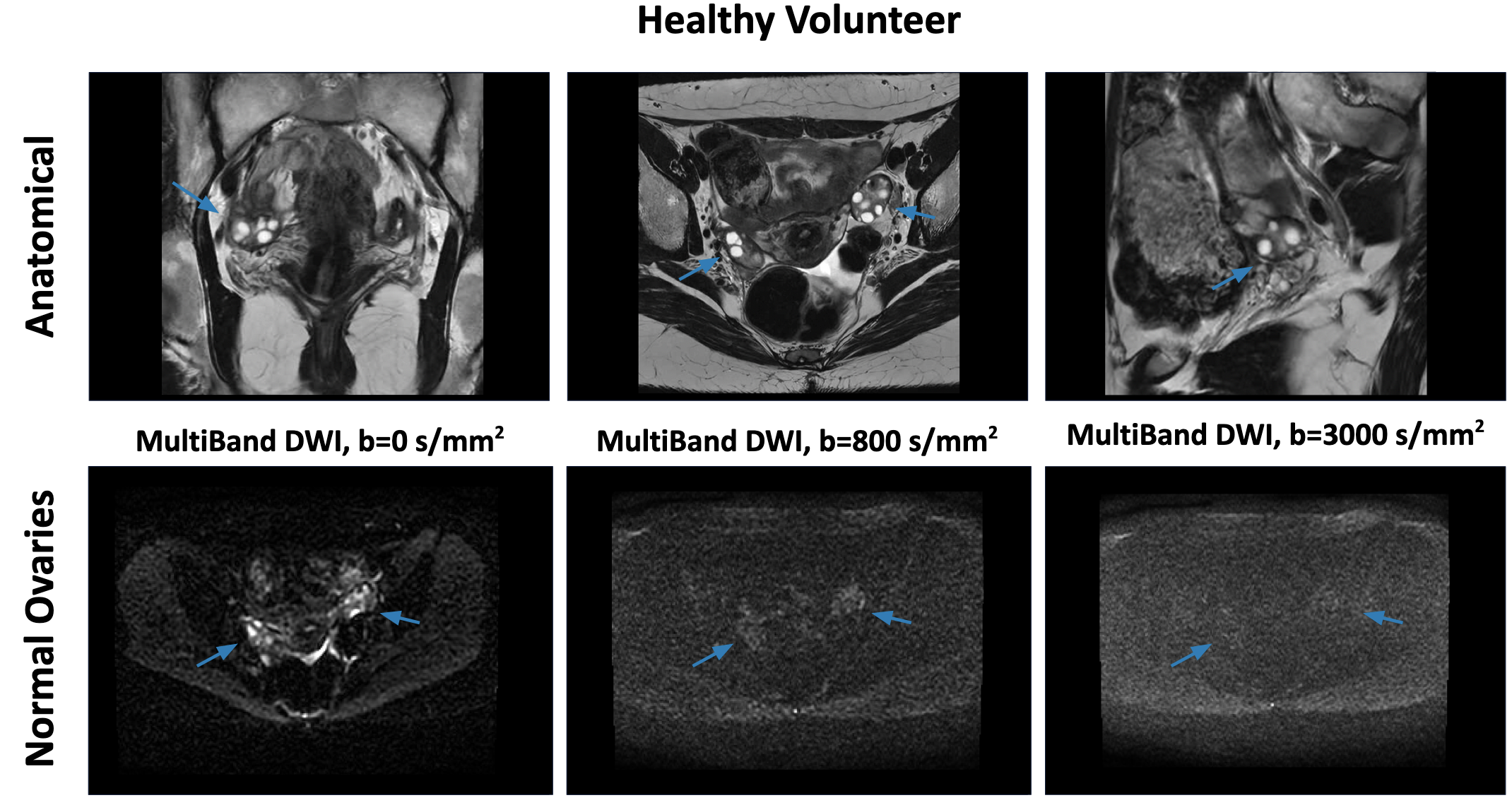
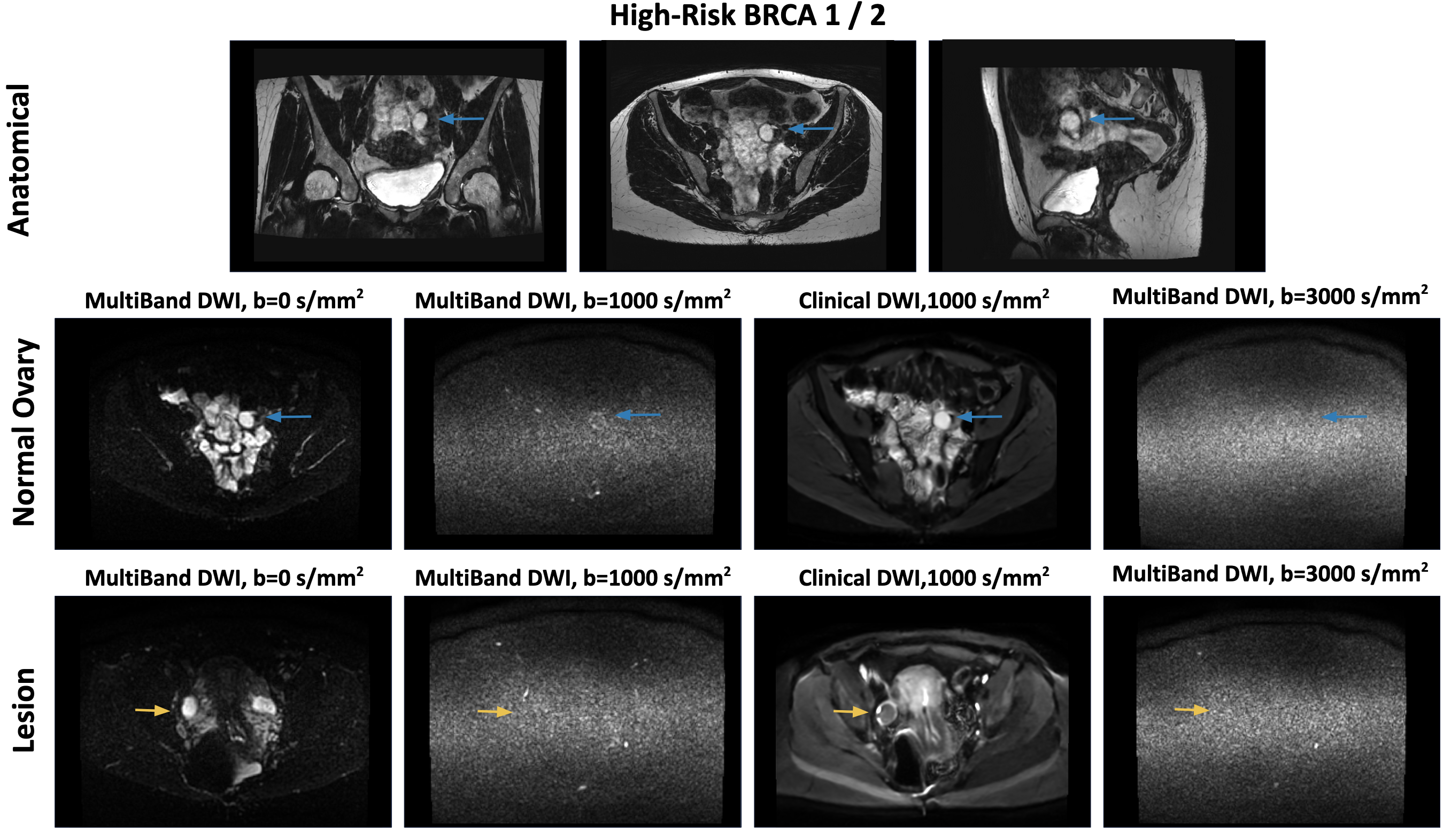
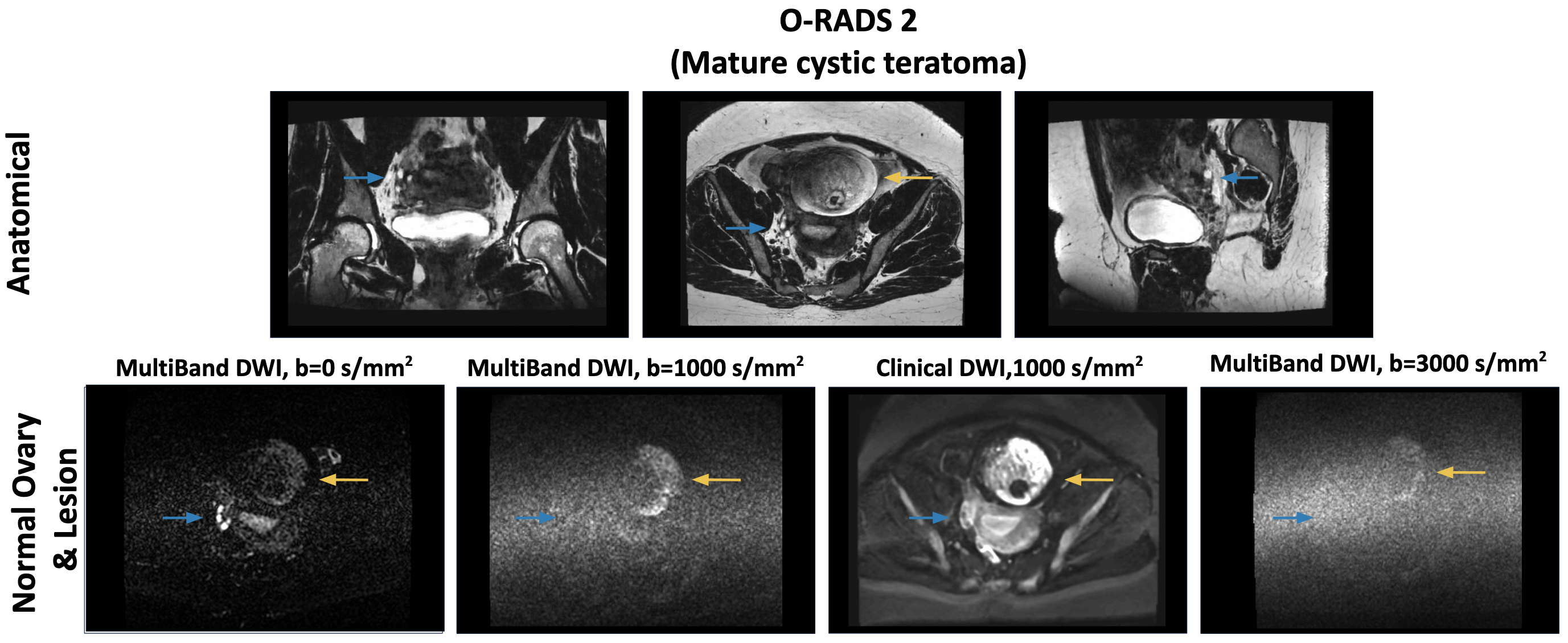
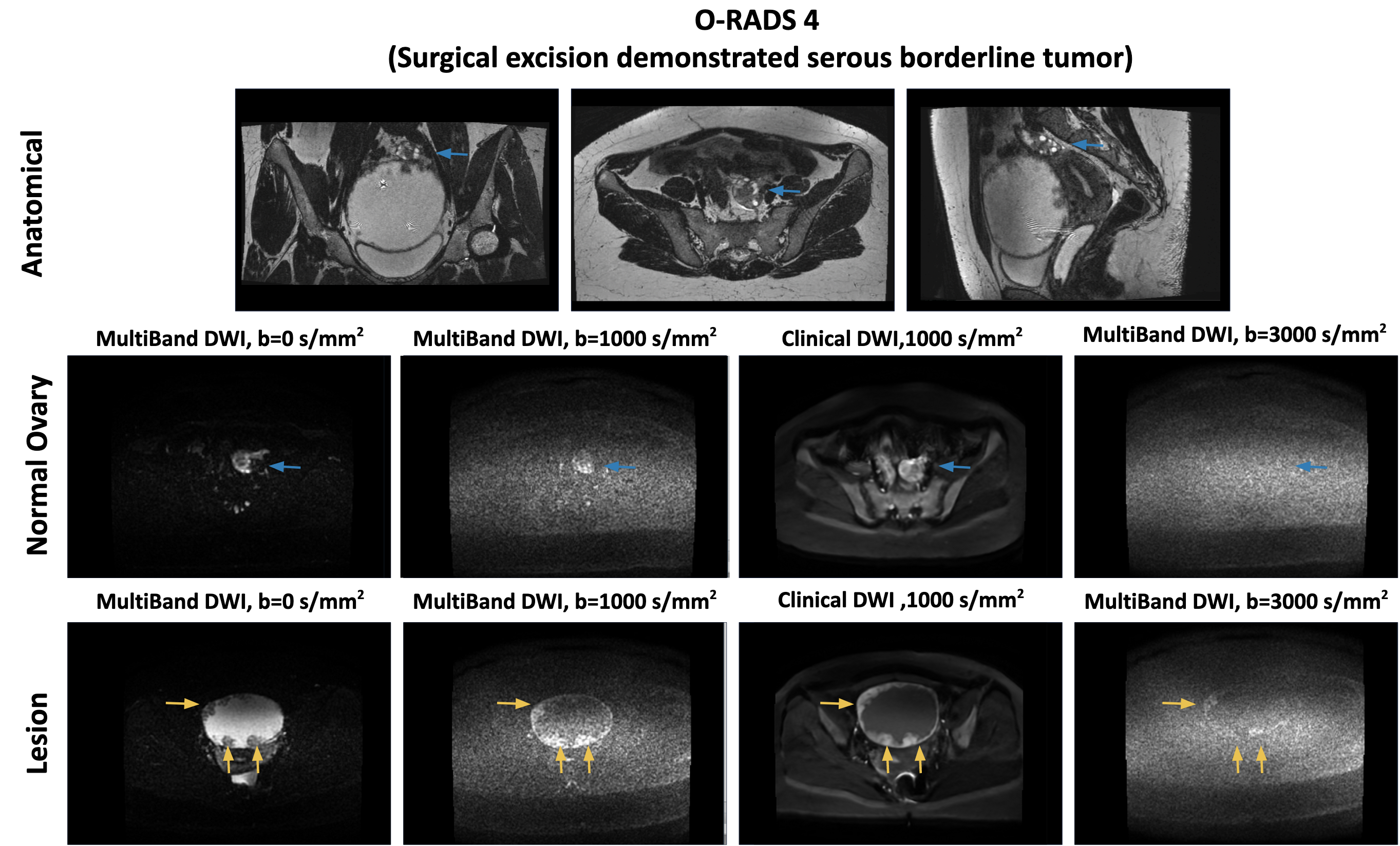
Four subjects were scanned using the proposed protocol. In all patients, moderate to high signal intensity was observed in MB-DWI images in normal ovaries at b=0, b=500 and b=1000. At b-values above 1000 (b=2000 and b=3000), normal ovaries were not visualized. Of note, normal ovaries had an average CNR of 2.5 in these patients when compared to the gluteus muscle. Follicles of normal ovary can still be seen on b=1000 both on ClinDWI and MB-DWI, though MB-DWI displays higher noise level. No signal is left at b=3000 (Figure 1-4).Figure 2 shows an example of a high-risk BRCA 1/2 patient. Main findings include a hemorrhagic cyst, with CNRs of 2.7, 3.4 and 3.9 at b=1000, 2000 and 3000 respectively. Figure 3 shows an example of an O-RADS 2, pathology-confirmed mature cystic teratoma, with CNRs of 2.5, 2.0 and 2.1. Figure 4 shows an example of an O-RADS 4 lesion, with CNRs of 1.4, 0.9 and 1.0. Surgical excision demonstrated a serous borderline tumor.
DISCUSSION & CONCLUSION
In this abstract we investigate preliminary steps of developing an ovarian cancer screening protocol. Four patients were scanned and Multiband allows collecting isotropic 2mm multishell DWI images. We see here promising results in improving specificity, using high-resolution, high b-value MB-DWI in our pilot cohort of patients. The variability in CNR measurements across lesion types illustrate the variability in their intrinsic diffusion characteristics.Next steps will focus on including more high-risk patients and on developing an ovarian Restriction Spectrum Imaging model13 (O-RSI). This technique relies on multishell DWI and separates signal in pools of diffusion types. It has proven able to distinguish cancers from benign lesions both in prostate14 and breast15, and appears promising for improved specificity.
Acknowledgements
Curebound research awardReferences
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. Jan 2019;69(1):7-34.doi:10.3322/caac.21551
2. Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2014, National Cancer Institute.2017. https://seer.cancer.gov/csr/1975_2014/
3. Menon U, Gentry-Maharaj A, Hallett R, et al. Sensitivity and specificity of multimodal and ultrasound screening for ovarian cancer, and stage distribution of detected cancers: results of the prevalence screen of the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Lancet Oncol. Apr 2009;10(4):327-40. doi:10.1016/S1470-2045(09)70026-9
4. Finch AP, Lubinski J, Moller P, et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol. May 20 2014;32(15):1547-53. doi:10.1200/JCO.2013.53.2820
5. Marchetti C, De Felice F, Palaia I, et al. Risk-reducing salpingo-oophorectomy: a meta-analysis on impact on ovarian cancer risk and all cause mortality in BRCA 1 and BRCA 2 mutation carriers. BMC Womens Health. Dec 12 2014;14:150. doi:10.1186/s12905-014-0150-5
6. Metcalfe K, Lynch HT, Foulkes WD, et al. Effect of Oophorectomy on Survival After Breast Cancer in BRCA1 and BRCA2 Mutation Carriers. JAMA Oncol. Jun 2015;1(3):306-13. doi:10.1001/jamaoncol.2015.0658
7. Manchanda R, Abdelraheim A, Johnson M, et al. Outcome of risk-reducing salpingo-oophorectomy in BRCA carriers and women of unknown mutation status. BJOG. Jun 2011;118(7):814-24. doi:10.1111/j.1471-0528.2011.02920.x
8. Rebbeck TR, Kauff ND, Domchek SM. Meta-analysis of risk reduction estimates associated with risk-reducing salpingo-oophorectomy in BRCA1 or BRCA2 mutation carriers. J Natl Cancer Inst. Jan 21 2009;101(2):80-7.doi:10.1093/jnci/djn442
9. Thomassin-Naggara I, Poncelet E, Jalaguier-Coudray A, et al. Ovarian-Adnexal Reporting Data System Magnetic Resonance Imaging (O-RADS MRI) Score for Risk Stratification of Sonographically Indeterminate Adnexal Masses. JAMA Netw Open. Jan 3 2020;3(1):e1919896. doi:10.1001/jamanetworkopen.2019.19896
10. Sadowski EA, Robbins JB, Rockall AG, Thomassin-Naggara I. A systematic approach to adnexal masses discovered on ultrasound: the ADNEx MR scoring system. Abdom Radiol (NY). Mar 2018;43(3):679-695. doi:10.1007/s00261-017-1272-7
11. Andreotti, R. F., Timmerman, D., Strachowski, L. M., Froyman, W., Benacerraf, B. R., Bennett, G. L., ... & Glanc, P. (2020). O-RADS US risk stratification and management system: a consensus guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology, 294(1), 168-185.
12. Desai, Nikunj & Singh, Abhinav & Valentino, Daniel. (2010). Practical Evaluation of Image Quality in Computed Radiographic (CR) Imaging Systems. Proceedings of SPIE - The International Society for Optical Engineering. 7622. 10.1117/12.844640.
13. Brunsing RL, Schenker-Ahmed NM, White NS, Parsons JK, Kane C, Kuperman J, Bartsch H, Kader AK, Rakow-Penner R, Seibert TM, Margolis D, Raman SS, McDonald CR, Farid N, Kesari S, Hansel D, Shabaik A, Dale AM, Karow DS. Restriction spectrum imaging: An evolving imaging biomarker in prostate MRI. J Magn Reson Imaging. 2017 Feb;45(2):323-336. doi: 10.1002/jmri.25419. Epub 2016 Aug 16.
14. Feng CH, Conlin CC, Batra K, Rodríguez-Soto AE, Karunamuni R, Simon A, Kuperman J, Rakow-Penner R, Hahn ME, Dale AM, Seibert TM. Voxel-level Classification of Prostate Cancer on Magnetic Resonance Imaging: Improving Accuracy Using Four-Compartment Restriction Spectrum Imaging. J Magn Reson Imaging. 2021 Sep;54(3):975-984. doi: 10.1002/jmri.27623. Epub 2021 Mar 31.
15. Rodríguez-Soto AE, Andreassen MMS, Fang LK, Conlin CC, Park HH, Ahn GS, Bartsch H, Kuperman J, Vidić I, Ojeda-Fournier H, Wallace AM, Hahn M, Seibert TM, Jerome NP, Østlie A, Bathen TF, Goa PE, Rakow-Penner R, Dale AM. Characterization of the diffusion signal of breast tissues using multi-exponential models. Magn Reson Med. 2022 Apr;87(4):1938-1951. doi: 10.1002/mrm.29090. Epub 2021 Dec 14.
Figures