4283
The feasibility of synthetic MRI using T1- and T2-mapping for the characterization of endometrial cancer.1Fondazione Policlinico Universitario A. Gemelli IRCCS, Roma, Italy, 2Università Cattolica del Sacro Cuore, Roma, Italy
Synopsis
Keywords: Uterus, Tumor, Endometrial cancer, mapping
Motivation: This study seeks to refine diagnostic precision for endometrial cancer, addressing the need for non-invasive biomarkers to improve preoperative assessment and risk stratification.
Goal(s): To evaluate the feasibility of synthetic MRI using T1-, T2- and proton density(PD) mapping for characterization, reflecting underlying tumor biology.
Approach: A pilot study with twenty patients using a 2D fast-spin-echo multi-saturation-delay multi-echo sequence to acquire synthetic MRI data, with analysis of T1, T2, and PD metrics compared with histopathological findings.
Results: The preliminary results suggest differences in T1 relaxation times between endometrioid vs. non-endometrioid subtype and low vs. high grade, suggesting a correlation with histopathological architecture of tumors.
Impact: If confirmed in larger studies, our results could adjust the approach to preoperative planning, allowing non-invasive depiction of tumor characteristics. This opens the door to personalized surgical strategies and streamline the decision-making process for adjuvant therapies, directly benefiting patient care.
Introduction
Endometrial cancer is the most common gynecological malignancy in developed countries and its incidence is rising, reflecting the global burden of the disease and associated healthcare challenges1. The primary treatment for endometrial cancer is surgical, involving hysterectomy with or without adjuvant therapies based on recurrence risk stratification. This stratification incorporates genetic profiling and is essential for guiding the management of the disease, according to ESGO-ESTRO-ESP guidelines2. Despite advances, the genetic diversity and pathophysiological complexity of endometrial cancer necessitate improved diagnostic precision1.Currently MRI is used for the preoperative assessment of endometrial cancer, accurately evaluating the local extent of disease3. Among the prognostic factors of endometrial cancer, myometrial invasion is the sole to be identifiable on routine MRI, and therefore quantitative methods have been investigated in order to create more specific imaging biomarkers.The integration of synthetic MR into this framework could further refine diagnostic and prognostic capabilities. Synthetic MRI is a flexible imaging technique that synthesizes contrast-weighted images from multi-contrast MRI data. Through a 2D multi-dynamic multi-echo sequence (MDME), it has the capacity to quantify T1 and T2 relaxation times and proton density (PD), offering a non-invasive method to characterize tissue properties4. These capabilities have found applications in neuroradiology, where synthetic MRI methods were proposed for brain tissue characterization, aiding in the diagnosis and management of neurological conditions5. In this context, we aim to explore the feasibility of synthetic MRI for simultaneous T1, T2, and PD mapping of endometrial cancer.Methods
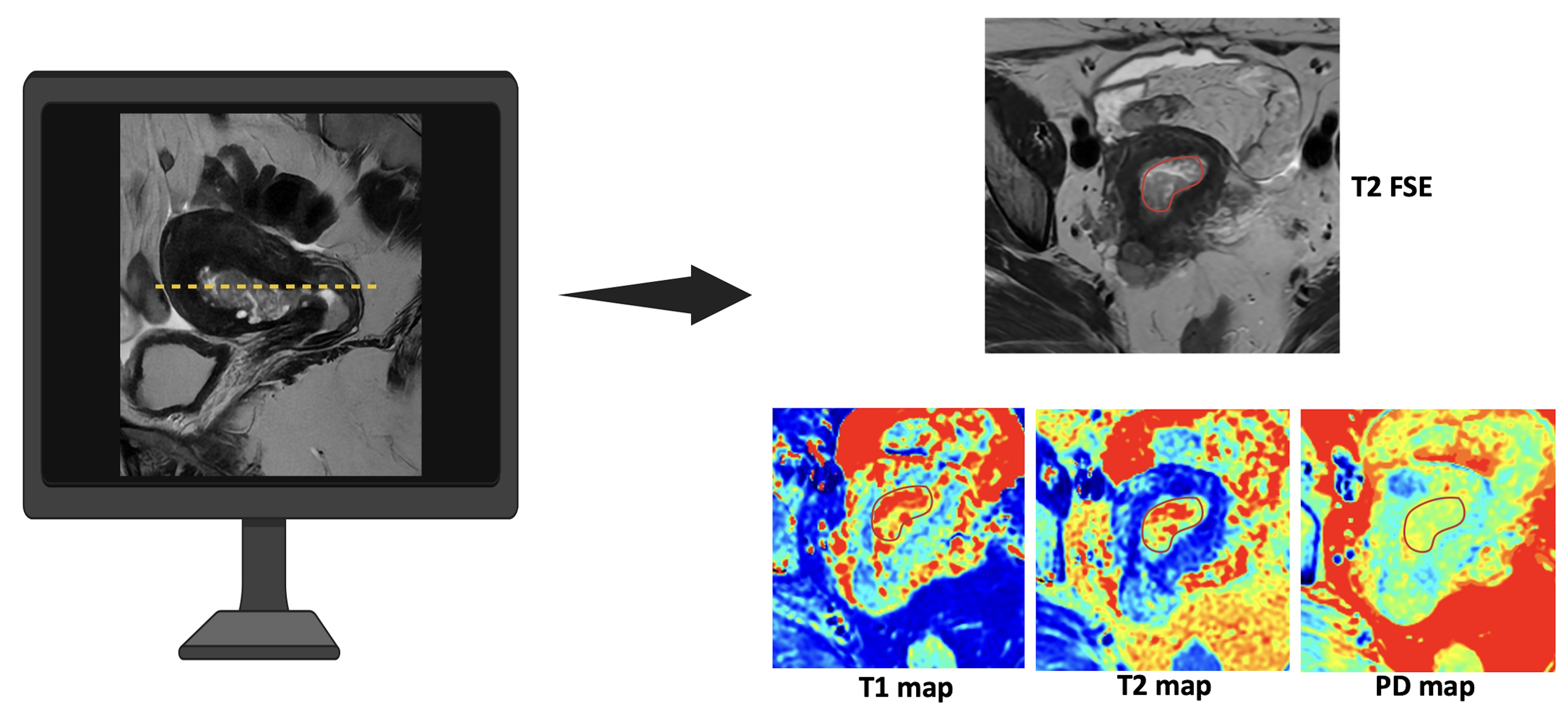
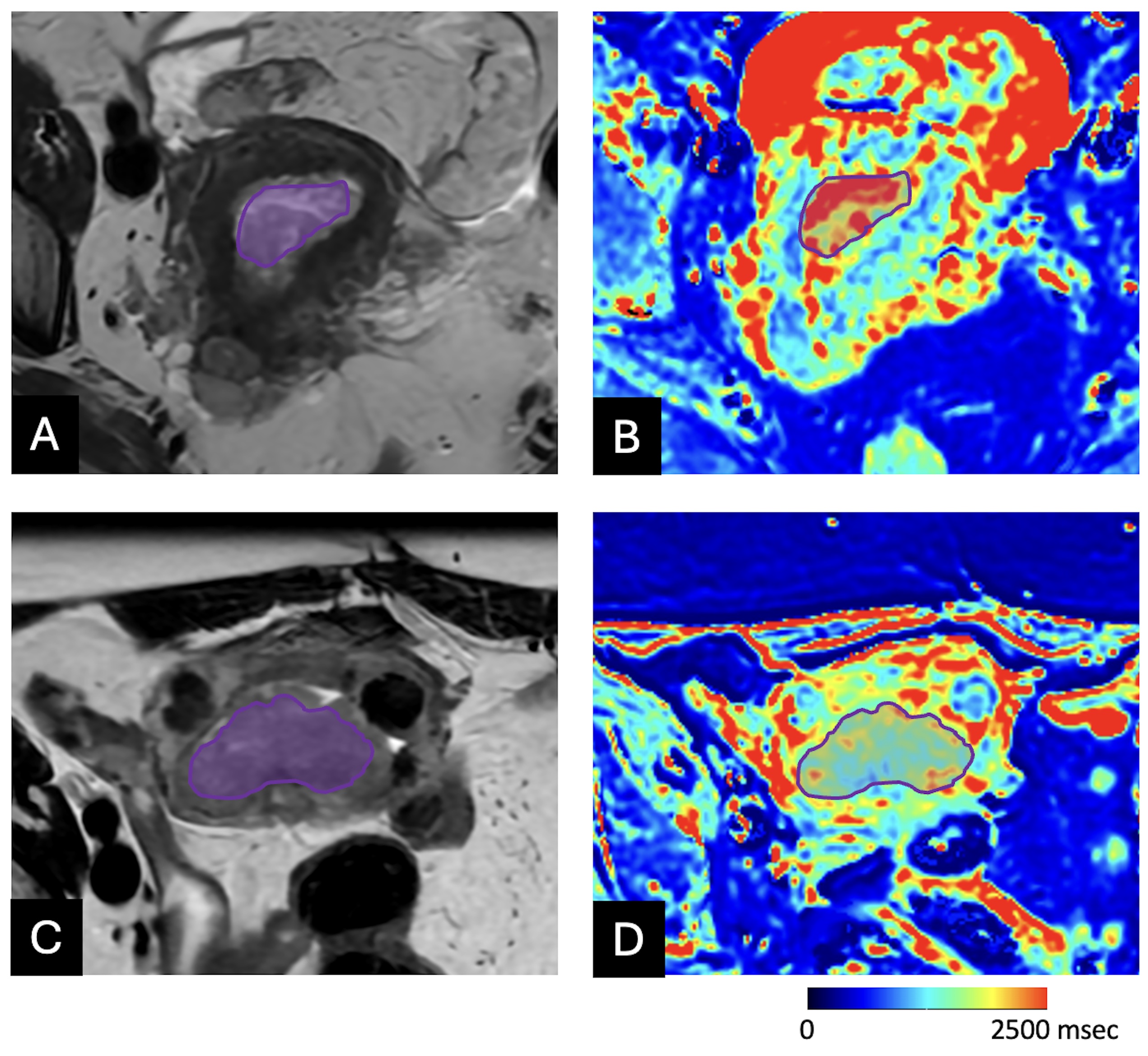
Patients with biopsy-proven endometrial cancer scheduled for MRI were prospectively enrolled in this pilot study. A 1.5T scanner (GE Healthcare Voyager, GE Healthcare, Milwaukee, WI) with AIR coil was used. Synthetic MRI data were acquired using a 2D fast-spin-echo multi-saturation-delay multi-echo named Magnetic Resonance Image Compilation (MAGiC). Synthetic T1-, T2 and PD maps were generated from MDME data using MAGiC software (GE Healthcare, Milwaukee, WI). Using synthetic T2-weighted images as mask, a radiologist with 5 years of experience in gynecologic imaging manually drew region of interests (ROIs) along the tumor margins on three consecutive axial sections including the tumor. Mean value of T1 and T2 relaxation times (msec) and PD (%) were obtained from each ROI and their mean values were calculated for each patient and considered for the statistical analysis. All patients underwent hysterectomy and bilateral salpingo-oophorectomy with or without lymphadenectomy. Histopathologic characteristics (histotype and grading) and risk groups were registered. The measured values (T1, T2 and PD) were presented as median (min-max). A formal statistical analysis was not carried on due to the limited number of cases.Results
Twenty patients were enrolled. At histology, 16/20 patients had an endometrioid adenocarcinoma, while 4/20 had a non-endometrioid adenocarcinoma. In endometrioid group, median T1 and T2 relaxation times and PD were: 1816 msec (1372-2146), 112 msec (70-192) and 83.5% (73.9-91.6). In non-endometrioid, median T1 and T2 relaxation times were 1312 msec (1250-1420) and 115 msec (109-120) respectively, while median PD was 84 msec (83.3-87.8). Median T1 relaxation time was 1812 msec (1372-2146) in G1 (4/20) and 1411 msec (1138-1920) in G2-G3 (16/20). No difference occurred in T2 relaxation time and PD between low (G1) and high-grade tumors (G2-G3). In low-risk groups -including low and intermediate groups (11/20 patients)- median T1 relaxation time was 1812 msec (1372-2146), while in high-risk groups (intermediate-high, high and advanced groups, 9/20) it was 1412 msec (1250-1753). No differences occurred in T2 relaxation time and PD between low and high-risk groups.Discussion
The preliminary findings of this pilot study suggest that endometrioid and non-endometrioid endometrial adenocarcinomas can be differentiated based on T1 relaxation times. Additionally, G1 tumors showed longer T1 times compared to G2-G3. The observed variance in T1 relaxation times can be attributable to distinct histopathological architectures. Endometrioid adenocarcinomas typically exhibit a higher degree of glandular differentiation and may possess a more complex microenvironment, potentially resulting in longer time of recover to the ground state. Conversely, the non-endometrioid subtype, often more aggressive and less differentiated, may demonstrate a denser cellular arrangement, leading to shorter T1 times.Conclusion
The disparity in T1 relaxation times observed in this study may reflect the underlying tissue heterogeneity of endometrial carcinoma. This suggests that T1 mapping could serve as a non-invasive alternative for histological assessment, contributing to preoperative stratification and management of endometrial cancer. Further research with larger datasets and in-depth statistical analysis is necessary to establish the clinical significance of these findings.Acknowledgements
No acknowledgement found.References
1. Makker V, MacKay H, Ray-Coquard I, et al. Endometrial cancer. Nat Rev Dis Primers. 2021 Dec 9;7(1):88.
2. Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021 Jan;31(1):12-39.
3. Maheshwari E, Nougaret S, Stein EB, et al. Update on MRI in Evaluation and Treatment of Endometrial Cancer. Radiographics. 2022 Nov-Dec;42(7):2112-2130.
4. Warntjes JB, Leinhard OD, West J, Lundberg P. Rapid magnetic resonance quantification on the brain: Optimization for clinical usage. Magn Reson Med 2008;60(2):320-329.
5. Ji S, Yang D, Lee J, et al. Synthetic MRI: Technologies and Applications in Neuroradiology. J Magn Reson Imaging. 2022 Apr;55(4):1013-1025.
Figures