4282
Differential Diagnosis of Borderline and Malignant Epithelial Ovarian Tumors: Insights from 3D APTWI to DKI1Radiolgy, Liaocheng People’s Hospital, Liaocheng, China, 2Liaocheng People’s Hospital, Liaocheng, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Pelvis, fMRI, Amide Proton Transfer Weighted Imaging,Diffusional Kurtosis Imaging,Borderline epithelial ovarian tumors,Malignant epithelial ovarian tumors
Motivation: Accurate diagnosis of BEOT and MEOT is crucial but remains challenging.
Goal(s): To investigate the diagnostic ability of APTWI and DKI in differentiating BEOT from MEOT and their correlation with the Ki-67 LI.
Approach: Those who had solid or solid-cystic lesions on one or both sides of the adnexal area on US and/or CT with a suspicion of malignancy were selected and underwent an MRI scan.and The parameters originate from them are analyzed
Results: The sMTRasymmax, cMTRasymmean , MDmean , and age displayed excellent diagnostic ability for BEOT and MEOT. Significant and positive correlations exist between sMTRasymmax and MKmean variables with Ki-67 LI.
Impact: This research is innovative and will promote the application of APT imaging technology in other soft tissue tumors. Researchs can be conducted in various aspects such as differential diagnosis and treatment responsiveness.
Introduction
The primary objective in managing ovarian cancer is to achieve optimal outcomes while minimizing unnecessary invasive surgeries1. BEOT predominantly occurs in women of reproductive age, with approximately one-third of cases affecting individuals under forty2. Consequently, fertility-sparing surgery is a desired approach2. Accurate diagnosis is crucial to facilitate surgical decision-making, if BEOT is diagnosed, fertility-sparing procedures and minimally invasive surgery can be performed for young patients3, and timely referral of the MEOT patients to expert centers should be done. Distinguishing between BEOT and MEOT remains challenging. The apparent diffusion coefficient (ADC) values of BEOT are higher than those of MEOT4, but clear cell carcinomas exhibit higher ADC values, overlapping those of BEO5. To date, reliable radiological or clinical features for preoperative diagnosis are lacking. Neither Ovarian-Adnexal Reporting and Data System (O-RADS) US 6 nor O-RAS MRI 8 involves differential diagnoses of BEOT and MEOT, even frozen section analysis has proven to be inadequate for precisely and rapidly diagnosing BEOT in many hospitals, with only 61.5% (8/13) of patients being correctly diagnosed6. This study aimed to investigate the diagnostic ability of APTWI and DKI in differentiating BEOT from MEOT and their correlation with the Ki-67 LI.Methods
From June 1, 2023, to January 31, 2023, those who had solid or solid-cystic lesions on one or both sides of the adnexal area on US and/or CT with a suspicion of malignancy were selected and underwent an MRI scan. The SAGITAL TSE-T2WI, CORNAL FS TSE-T2WI, AXIAL FS TSE-T2WI, TSE-T1WI, SS-EPI DWI, SS-EPI DKI, and 3D TSE APTWI sequences were performed and the parameters originate from them are analyzed.Results
In total, 21 BEOT and 78 MEOT patients were collected consecutively, whose ages are 50.8±13.16 years and 61.12±11.26 years, respectively ( P =0.016). Serum CRP (P=0.02), FIGO surgical stage (P=0.001), CA125 level (P=0.013), Ki-67, P53, P16, ER, and PR LIs were significantly lower in the BEOT group. The parameters of the solid lesion components were denoted with the prefix 's', and the parameters of the cystic lesion components were marked with the prefix 'c'. The minimum value of magnetization transfer ratio with asymmetric analysis at 3.5 ppm (sMTRasymmin)(P=0.005),sMTRasymmax(P=0.01), and cMTRasymmean (P=0.001) were significantly lower in the BEOT group, and the sADCmean(P=0.001) and sADCmin (P=0.011), as well as MDmean (P=0.009), MKmean (P=0.012), and MKmin (P=0.048) were significantly higher in the BEOT group. After simple and multiple logistic regression analysis, sMTRasymmax (P=0.015), cMTRasymmean (P=0.030), MDmean(P=0.014), and age (P=0.018) were screened out. Receiver operating characteristic (ROC) curve analysis showed that MDmean + sMRTasymmax, MDmean + age, with any two of MDmean, age, and sMRTasymmax selected as the diagnostic basis were chosen as the best variable combination. The linear regression analysis showed that sMTRasymmax (P=0.049) and MDmean (P<0.001) were significantly correlated with Ki-67 LI.Discussion
SMTRasymmax is an independent diagnostic parameter, which may represent the measurements from the voxel(s) containing cancer cells with higher secretory capacity, cellularity, cytosolic protein density, and fresh blood supply7. So the values may reflect the dynamic nature of tumor areas with the highest biological activity and aggressive ability.CMTRasmymean emerges as another independent diagnostic parameter (P=0.03). The cystic fluid is a complex mixture originating from tumor parenchymal cells, blood, and exfoliated cancer cells, exhibiting comparable P53 and Ki-67 LI expression levels as tissue cells8. Cancer cells may secrete immune factors, antibodies, and amino acids into the cystic fluid, leading to increased concentrations of mobile proteins and peptides and higher cMTRasymmean values 9. Second, hemorrhage and necrosis commonly occur in malignant tumors, causing a continuous influx of fresh blood into the cystic fluid, which manifests higher signal intensity on APTWI26. MDmean is the only independent diagnostic parameter. DKI takes the non-Gaussian diffusion distribution resulting from the complex tissue intracellular and internal environment, including cell membranes and organelles, as well as rapid proton exchange into consideration10.MD values can more accurately represent the actual water diffusion in tumor tissue than conventional ADC values 11. Contrary to previous studies12,13, our analysis revealed a significant correlation between Ki-67 LI and MDmean (rather than MKmean). This discrepancy may be explained by the extent of diffusion restriction reflected by MDmean exceeding the degree of heterogeneity reflected by MKmean concerning the increasing malignancy of ovarian tumors.Conclusion
The combination of DKI and APTWI displayed excellent diagnostic ability for BEOT and MEOT. Significant and positive correlations exist between sMTRasymmax and MKmean variables with Ki-67 LI.Acknowledgements
No acknowledgement found.References
1 Andreotti RF, Timmerman D, Strachowski LM, et al O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 2020;294(1): p. 168-185.
2 Sun H, Chen X, Zhu T, et al. Age-dependent difference in impact of fertility preserving surgery on disease-specific survival in women with stage I borderline ovarian tumors. J Ovarian Res 2018;11(1): p. 54.
3 Thomassin-Naggara I, Belghitti M, Milon A, et al. O-RADS MRI SCORE: An Essential First-Step Tool for the Characterization of Adnexal Masses. Journal of Magnetic Resonance Imaging 2023; https://dx.doi.org/10.1002/jmri.289474 Ono T, Kishimoto K, Tajima S, Maeda I, Takagi M, Suzuki N, et al. Apparent diffusion coefficient (ADC) values of serous, endometrioid, and clear cell carcinoma of the ovary: pathological correlation. Acta Radiol. 2020;61(7):992-1000
5 Zhao SH, Qiang JW, Zhang GF, Ma FH, Cai SQ, Li HM, et al. Diffusion-weighted MR imaging for differentiating borderline from malignant epithelial tumours of the ovary: pathological correlation. Eur Radiol. 2014;24(9):2292-9
6 Gaballa K, Abdelkhalek M, Fathi A, Refky B, Belal K, Elaraby M, et al. Management of borderline ovarian tumors: A tertiary referral center experience in Egypt. Front Surg. 2022;9:962820.
7 Guo H, Liu J, Hu J, Zhang H, Zhao W, Gao M, et al. Diagnostic performance of gliomas grading and IDH status decoding A comparison between 3D amide proton transfer APT and four diffusion-weighted MRI models. J Magn Reson Imaging. 2022;56(6):1834-44
8 Harlozińska A, Bar JK, Sedlaczek P, et al. Expression of p53 protein and Ki-67 reactivity in ovarian neoplasms. Correlation with histopathology. Am J Clin Pathol 1996;105(3): p. 334-40.
9 Harłozińska A, Bar JK, Gawlikowski W, et al. CA 125 and carcinoembryonic antigen levels in cyst fluid, ascites, and serum of patients with ovarian neoplasms. Ann Chir Gynaecol 1991;80(4): p. 368-75.10 Van Cauter S, Veraart J, Sijbers J, Peeters RR, Himmelreich U, De Keyzer F, et al. Gliomas: diffusion kurtosis MR imaging in grading. Radiology. 2012;263(2):492-501.
11 Ochiai R, Mukuda N, Yunaga H, et al. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn Reson Med 2005;53(6): p. 1432-40.
12 Yuan L, Lin X, Zhao P, et al. Correlations between DKI and DWI with Ki-67 in gastric adenocarcinoma. Acta Radiol 2023p. 2841851231153035.
13 He P, Wang JJ, Duan W, et al. Estimating the risk of malignancy of adnexal masses: validation of the ADNEX model in the hands of nonexpert ultrasonographers in a gynaecological oncology centre in China. J Ovarian Res 2021;14(1): p. 169.
Figures
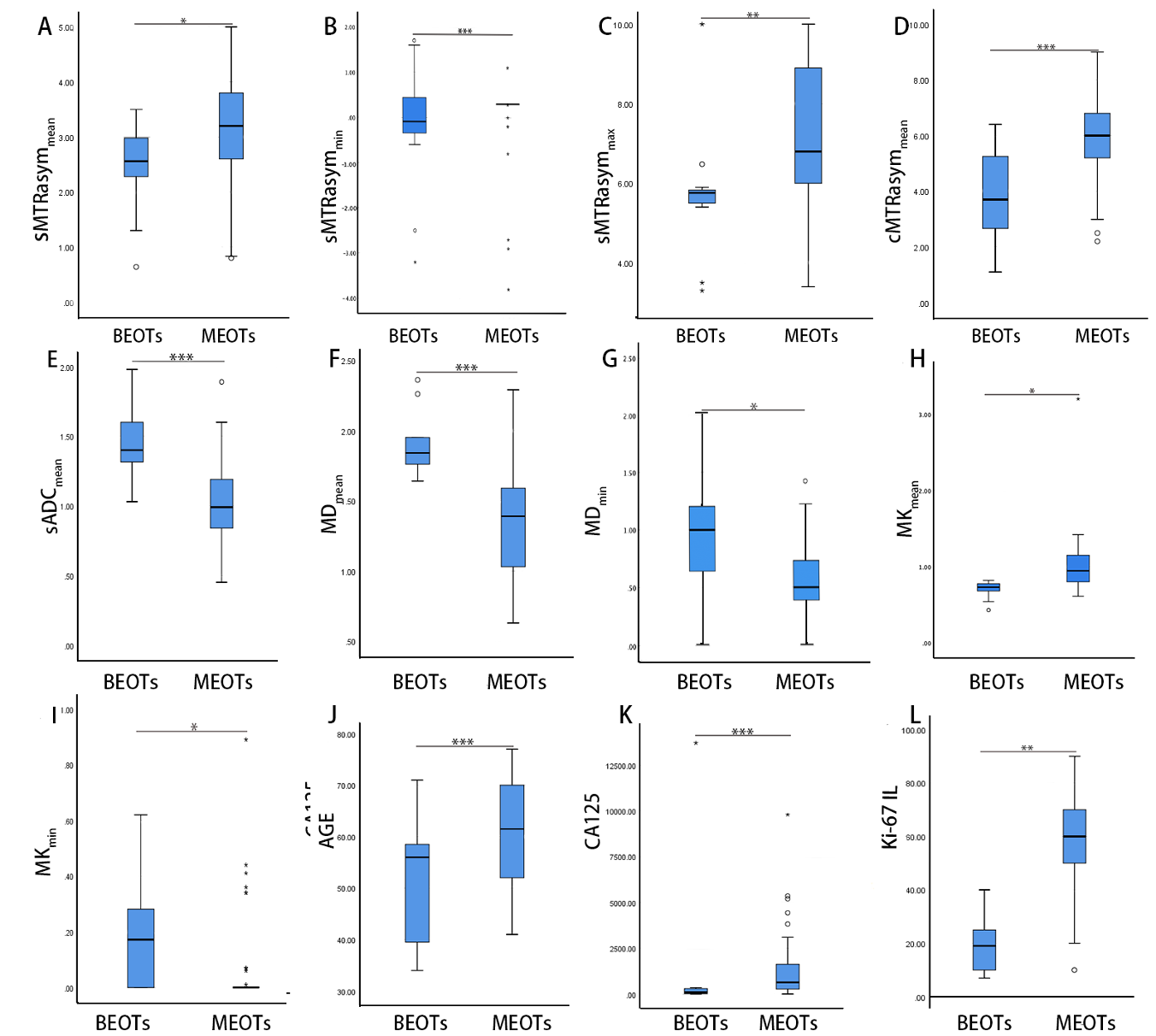
Figure 1. Box and whisker plots showing comparisons of radio-clinical parameters between BEOTs and MEOTs (only the parameters with significant differences are shown here). The sMTRasymmin, MKmin, CA125, and Ki-67 IL were analyzed by the independent-sample Mann-Whitney U Test and the remainder by the independent sample’s t-test.
Note: *, **, and *** indicate p < 0.05, 0.01, and 0.001, respectively
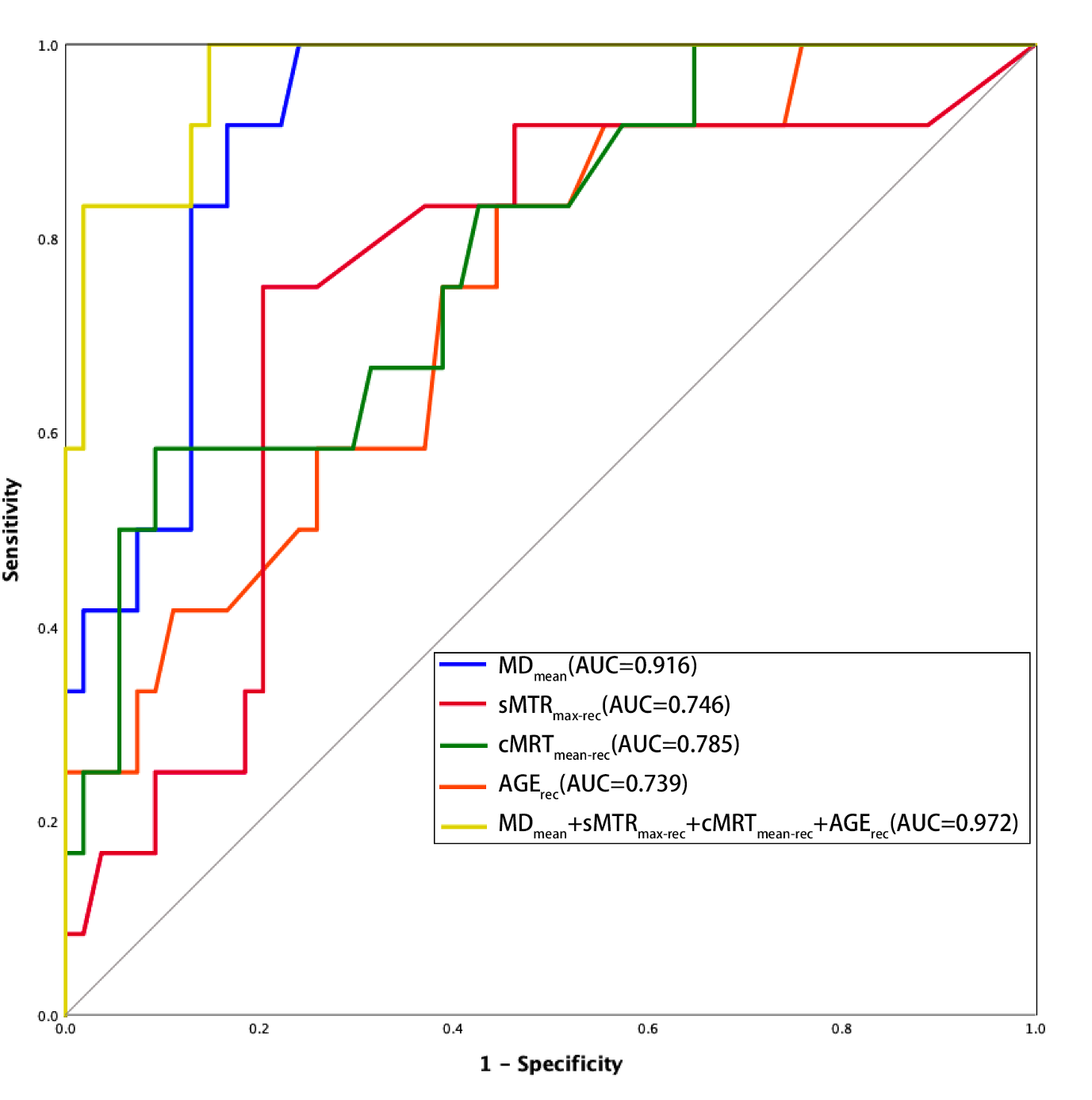
Figure 2. ROC curves of the independent diagnostic parameters and their combination diagnos
sMTRmax-rec= reciprocal of MDmean value
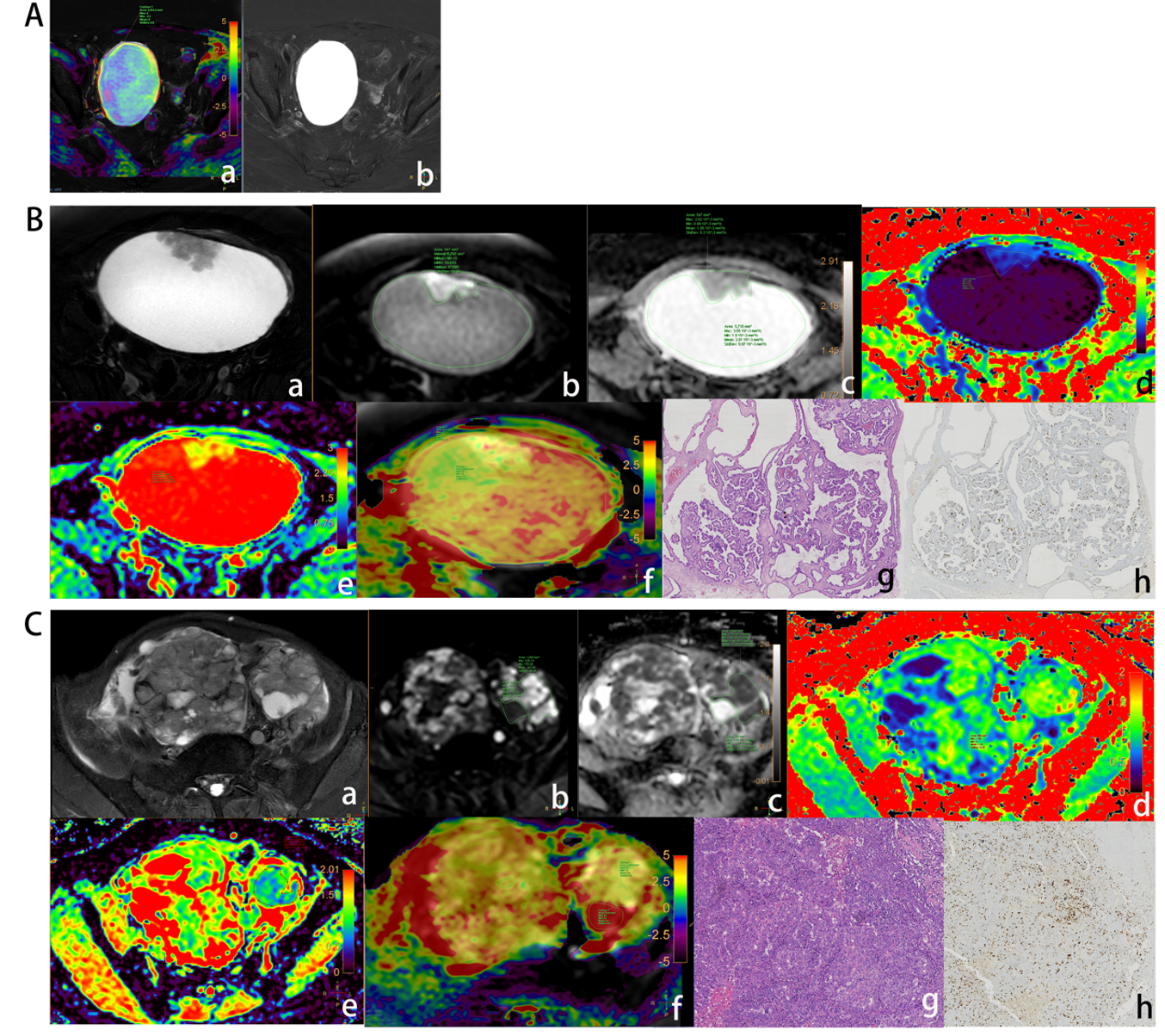
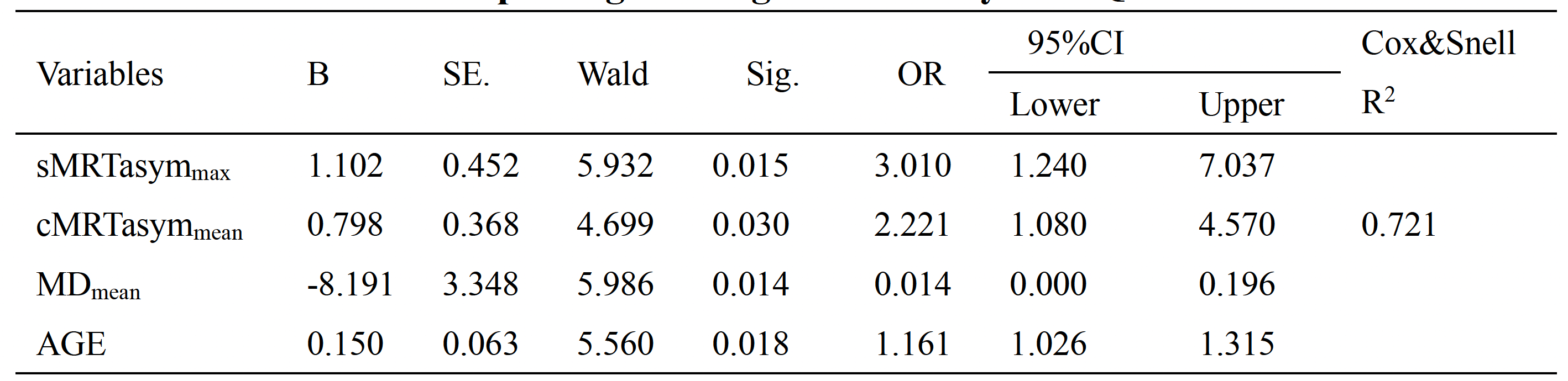
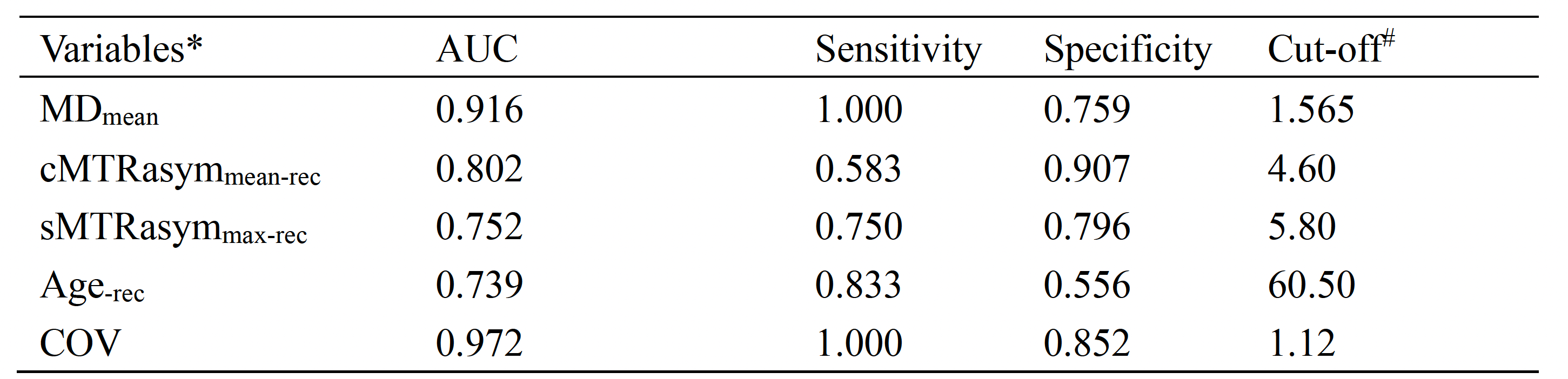
Table 2. Results of the ROC Analysis of Independent Diagnostic Variables
*The MTRasym unit is %, the ADC and MD units are mm2/s*10-3, and the age is recorded in years. # Cut-off value is the actual value of the variables.