4274
Automated patient registration in low field MRI using deep learning-based height and weight estimation with 3D camera1Siemens Healthineers GmbH, Erlangen, Germany, 2Department of Radiology, Neuroradiology and Nuclear Medicine, Johannes Wesling University Hospital, Ruhr University Bochum, Bochum, Germany
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Machine Learning/Artificial Intelligence, Patient auto-positioning in low-field MRI
Motivation: Automated patient positioning and Specific Absorption Rate (SAR) estimation in MRI is crucial for optimized image quality. Achieving these objectives necessitates precise patient parameter estimation. Typically, manual estimation of patient parameters, such as height and weight, is error-prone and time-intensive.
Goal(s): To assess the 3D camera's potential for acquiring depth images suitable for deep learning (DL)-based estimation of patient height and weight.
Approach: We employed 3D camera technology to capture depth images of patients on MRI tables, enabling DL-based height and weight estimation.
Results: Our evaluation study demonstrated the 3D camera's effectiveness in acquiring depth images for accurate patient height and weight estimation.
Impact: Current deep learning-driven 3D camera methods enhance MR imaging workflows with the goal of achieving standardized and higher-quality image acquisition by accurately predicting patient height and weight.
INTRODUCTION
Accurate and efficient estimation of patient height and weight is crucial in ensuring patient safety and optimizing the quality of magnetic resonance imaging (MRI) procedures. Currently, patient height and weight rely on estimates from patients or medical technologists for radiology (MTR). The aim of this study was to compare a novel deep learning (DL)-based three-dimensional (3D) camera estimation method to MTR staff in terms of estimation accuracy during routine 0.55T MRI exams. We anticipate that the 3D camera provides accurate estimates compared to MTR.METHODS
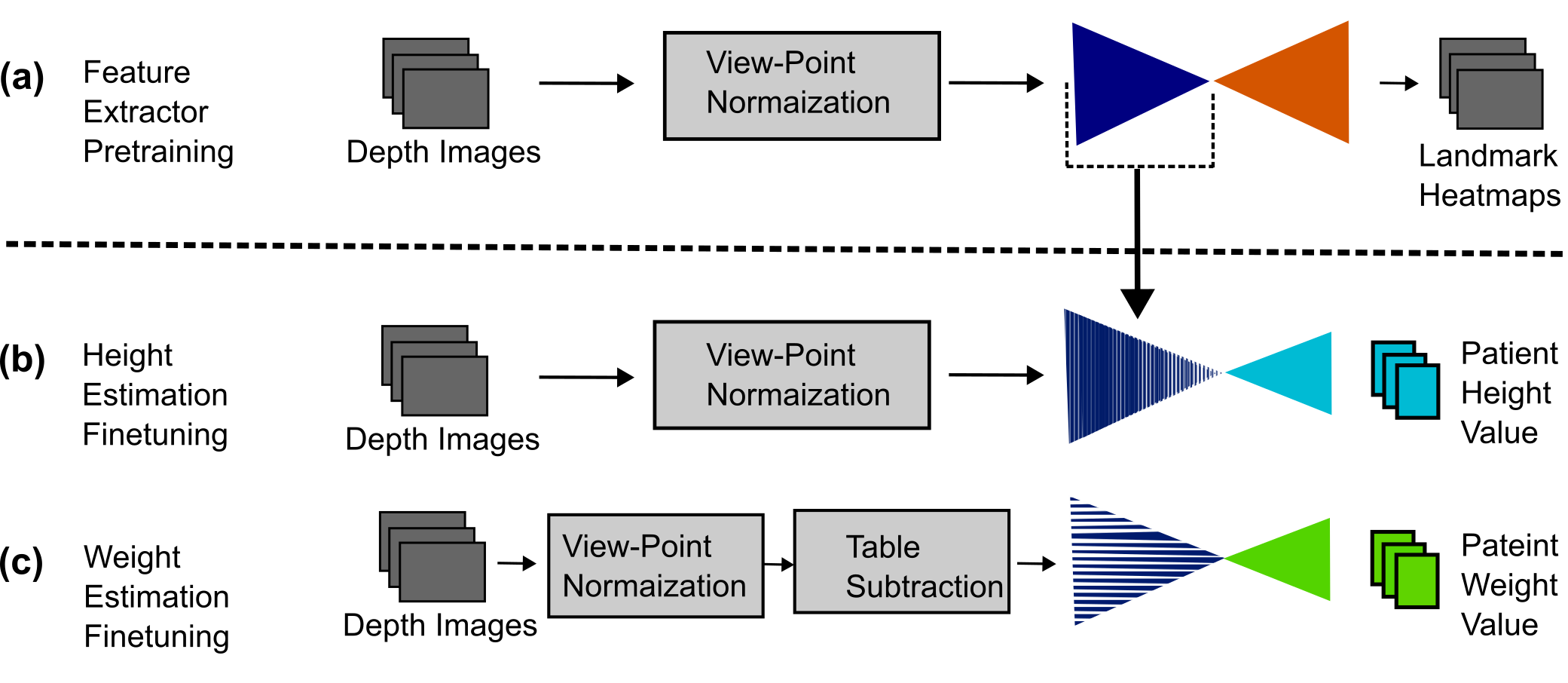
A retrospective study was conducted to compare the accuracy of height and weight estimation with a DL-based algorithm to the accuracy of height and weight estimation by the MTR. Patients’ height and weight values were first visually estimated by the MTR. Patients’ true height (cm) and weight (kg) values were measured with a calibrated scale (SECA 220, Seca GmBH, Hamburg, Germany). Depth images of the patients were captured with 3D camera during the regular imaging workflow on low field 0.55T Free.Max MRI scanner (MAGNETOM Free.Max, Siemens Healthineers, Erlangen, Germany) and then processed retrospectively within a DL framework as depicted in Figure 1. First, the depth images were normalized to account for variations in patient tables and camera viewpoints. These normalized images were then passed through an image-in image-out encoder-decoder network 1. The model employs a modified ResNet architecture 2 for feature extraction. This network is trained with landmark localization as an auxiliary task (Figure 1a). Subsequent to the training phase, two separate regression networks were developed (Figure 1b and 1c) to estimate patient height and weight. To achieve this, untrained decoder heads were added to the pre-trained encoder bases and all model parameters were fine-tuned for optimized performance and accuracy. For more in-depth information on this methodology, please refer to Tamersoy et al. 3. Accuracy of each estimation method (i.e. DL and MTR) was evaluated by computing the proportions of the estimates within 5% and 15% of the actual height (PH05, PH15) and within 10% and 20% of actual weight (PW10, PW20). An acceptable accuracy for height estimation was predetermined to be PH05 = 95% and PH15 = 99% and an acceptable accuracy for weight estimation was predetermined to be PW10 = 70% and PW20 = 95% as established by Wells et al. 4. The bias in height and weight estimation was measured by the mean percentage error (MPE). A correlation between ground truth and each method of estimating height and weight was computed using Pearson’s correlation coefficient (r).RESULTS
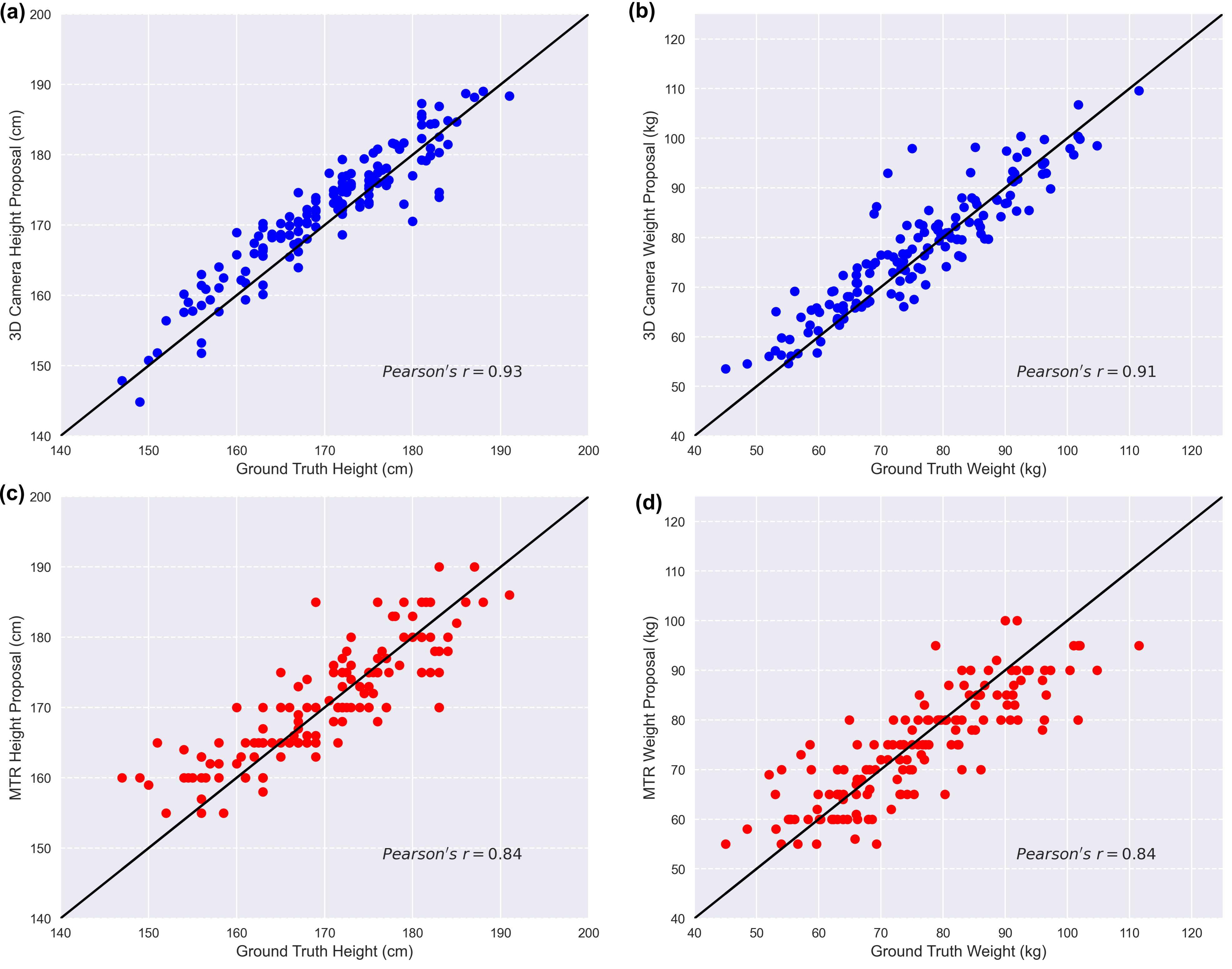
The retrospective study included 162 adult patients. DL-based 3D camera algorithm outperformed the MTR in estimating the patient’s height and weight in terms of accuracy (3D camera: PH05 = 98.6%, PH15 = 100%, PW10 = 85.1%, PW20 = 95.9%; MTR: PH05 = 92.5%, PH15 = 100%, PW10 = 75.0%, PW20 = 93.2%). MTR had slightly less bias in their estimates compared to the DL-based 3D camera algorithm (3D camera: MPE height = 1.1%, MPE weight=2.7%, MTR: MPE height = 0.3%, MPE weight = 0%). The estimation scatter plots, and the computed correlation coefficients are illustrated in Figure 2. For both height and weight estimation, the 3D camera had a higher correlation with ground truth (Pearson’s r = 0.93 for height estimation and Pearson’s r = 0.91 for weight estimation) (Figure 2 (a,b)), compared to the MTRA estimates (Pearson’s r = 0.84 for height estimation and Pearson’s r = 0.84 for weight estimation) (Figure 2 (c,d)).DISCUSSION
The 3D camera-based method showed significantly better performance in height and weight estimation compared to the estimate provided by MTR. Accurate height and weight estimation have important implications for patient positioning inside the scanner. In MRI, excessive radiofrequency (RF) deposition is a safety concern that can cause undesired patient heating. In order to ensure safe and compliant scanning, MRI scanners are mandated to provide estimated SAR values 5. Accurately estimating patient weight using a 3D camera can serve as a viable alternative for obtaining precise SAR values. By incorporating this technology, healthcare professionals can enhance the accuracy of SAR estimation, contributing to improved safety and adherence to regulatory guidelines during MRI scans.CONCLUSION
This study has demonstrated that the estimation of the patient’s height and weight by a DL-based 3D camera algorithm is accurate and robust. It has the potential to complement the regular MRI workflows, by providing further automation during patient registration.Acknowledgements
No acknowledgement found.References
1. Kingma D.P, Welling M. Auto-encoding variational bayes. arXiv preprint arXiv. 2013;1312.6114.
2. He K, Zhang X, Ren S, et al. Deep residual learning for image recognition. In Proceedings of the IEEE conference on computer vision and pattern recognition. 2016;770-778.
3. Tamersoy B, Pirvan F A, Pai S, et al. Accurate and Robust Patient Height and Weight Estimation in Clinical Imaging Using a Depth Camera. In International Conference on Medical Image Computing and Computer-Assisted Intervention. 2023;337-346.
4. Wells M, Goldstein L.N, Bentley A. The accuracy of emergency weight estimation systems in children—a systematic review and meta-analysis. International Journal of Emergency Medicine. 2017; 10(1):1-43.
5. Zaremba L.A. FDA guidance for magnetic resonance system safety and patient exposures: current status and future considerations. Boca Raton, FL, USA: CRC Press. 2001;183-196.
Figures