4233
The effect of total sleep deprivation on brain activity in medical staff during routine clinical work: A resting-state functional MR imaging study1Chongqing Hospital of Traditional Chinese Medicine, Chongqing, China, 2Army Medical University (Third Military Medical University), Chongqing, China, 3GE Healthcare MR Research, Beijing, China
Synopsis
Keywords: fMRI Acquisition, fMRI (resting state)
Motivation: Understanding the neuropathological mechanisms through which total sleep deprivation (TSD) leads to cognitive impairments is crucial for developing effective cognitive protection strategies and treatment measures.
Goal(s): Assess the effects of TSD on the brain functioning of medical staff. By investigating the impact of TSD on the brain, we aim to gain insights into the specific changes that occur and their potential implications for cognitive performance.
Approach: Thirty-six primary medical staff were enrolled, and each participant underwent resting-state functional Magnetic Resonance Imaging (rs-fMRI) to assess brain activity patterns.
Results: Our findings revealed significant enhancements in rs-fMRI features across multiple brain regions following sleep deprivation
Impact: Enhanced rs-fMRI features might be potential imaging biomarkers for distinguishing between RW and TSD states. Such distinctions can contribute to early detection and intervention, ultimately improving the management of sleep deprivation-related cognitive impairments among medical staff.
Introduction
Sleep deprivation (SD) has emerged as a global health concern 1, affecting individuals across various professions, including medical staff. SD can significantly impact cognitive functions 2,3 and pose risks to both the well-being of medical staff and the quality of patient care 4–6. Understanding how total SD (TSD) alters brain activity and leads to cognitive impairments remains an ongoing challenge 2. Resting-state Functional Magnetic Resonance Imaging (rs-fMRI) holds promise as a noninvasive imaging technique to explore how SD affects cognition. Most previous TSD studies were performed under controlled laboratory conditions, where subjects were usually instructed to do low-intensity activities during TSD, such as reading, watching movies 7. However, the working conditions of medical staff during night shifts differ significantly from these controlled conditions 8. Medical professionals are required to operate in fast-paced and high-pressure environments, which may lead to different effects of TSD on the brain 9. Given that medical work is a matter of life and death, it is important to investigate the potential harm of TSD to medical staff.Methods:
ParticipantsThirty-six medical staff were recruited.
MRI Acquisition
The rs-fMRI scans were conducted twice: once during rested wakefulness (RW) after a normal sleep period, and again after 24 hours of acute TSD.
Data Analysis
The acquired rs-fMRI data were processed using Data Processing and Analysis for Brain Imaging (DPABI). The features of interest included the mean fractional amplitude of low-frequency fluctuation (mfALFF), z-score transformed regional homogeneity (zReHo), and functional connectivity (zFC). Correlation coefficients between significantly altered rs-fMRI features and scores of neuropsychological tests after TSD were calculated. Receiver operating characteristic (ROC) and logistic regression analyses were performed to evaluate the diagnostic efficacy of significantly altered rs-fMRI features in distinguishing between RW and TSD states. DeLong’s test was used to compare the differences between the AUCs of different ROC curves.
Results:
Brain regions including right superior temporal gyrus, bilateral postcentral gyrus, left medial superior frontal gyrus, left middle temporal gyrus, right precentral gyrus, left precuneus showed significantly enhanced rs-fMRI features after TSD (Figure 1-3, Table 2,3). Additionally, rs-fMRI features of right superior temporal gyrus, right postcentral gyrus, left medial superior frontal gyrus were significantly correlated with scores of several neuropsychological tests (Table 4).Furthermore, the combination of mfALFF (bilateral postcentral gyrus) and zFC (left medial superior frontal gyrus and left precuneus) showed the highest area under curve (0.870) in distinguishing RW from TSD (Figure 4, Table 5).
Discussion
Our results revealed increased mfALFF in bilateral postcentral gyrus after TSD. Postcentral gyrus is the hub of the somatosensory network (sense of touch and kinesthesia) 10,11. Somatomotor network sends orders, and somatosensory network receives feedback messages to form a closed loop 12. Our results also found increased spontaneous brain activity in right superior temporal gyrus after TSD. The superior temporal gyrus includes auditory and language cortices, and is associated with social cognition 13,14. Our results also showed that score in DST declined after TSD (Table 1), and right superior temporal gyrus was negatively correlated with scores of DST. DST test asking participants to match symbols with corresponding numbers. As language server as a symbol system, language ability also affects the individual's ability to convert between different symbols to a certain extent 15.Then, we found enhanced functional connectivity after TSD. These hints suggested that after TSD, not only the activity of some brain regions altered, but also the FC between these brain regions and other brain regions strengthened. We speculated that these alterations may be part of functional damage or a compensatory mechanism of the brain.
Another important finding is that, some altered rs-fMRI features were correlated to the performance of the neuropsychological tests in TSD state. These evidences confirmed that there may be cognitive impairments in these areas with changed brain activities.
Our results demonstrated that the combined model (mfALFF of the bilateral postcentral gyrus and FC of the left medial superior frontal gyrus and left precuneus) had significantly better diagnostic efficacy than all single-parameter models.
conclusion
Spontaneous brain activity alterations occurred after TSD under workload, which might be associated with the reduced performance of medical staff in neurocognitive tests. These altered rs-fMRI features might be potential imaging biomarkers in distinguishing between TSD and RW brain states. It is hoped that this kind of research can provide a theoretical basis for the evaluation system of cognitive impairment, warn medical staff of the high risk of cognitive decline, promote the development of cognitive protection strategies and treatment measures, in order to better protect the safety of medical staff and the life and health of patients.Acknowledgements
We thank all the participants involved in this study.References
1. Basner M, Rao H, Goel N, Dinges DF. Sleep deprivation and neurobehavioral dynamics. Curr Opin Neurobiol. 2013;23(5):854-863. doi:10.1016/j.conb.2013.02.008
2. Adam J. Krause, Eti Ben Simon, Bryce A. Mander, Stephanie M. Greer, Jared M. Saletin ANGPPW. The sleep-deprived human brain. Nat Rev Neurosci. 2017;18(7):404-418. doi:10.1038/nrn.2017.55
3. Lim J, Dinges DF. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol Bull. 2010;136(3):375-389. doi:10.1037/a0018883
4. Neville K, Velmer G, Brown S, Robol N. A pilot study to examine the relationship between napping and fatigue in nurses practicing on the night shift. J Nurs Adm. 2017;47(11):581-586. doi:10.1097/NNA.0000000000000546
5. Johnson AL, Jung L, Brown KC, Weaver MT, Kathy C. Richards. Sleep deprivation and error in nurses who work the night shift. J Nurs Adm. 2014;44(1):17-22. doi:10.1097/NNA.0000000000000016
6. Yan FX, Lin JL, Lin JH, Chen HJ, Lin YJ. Altered dynamic brain activity and its association with memory decline after night shift-related sleep deprivation in nurses. J Clin Nurs. 2023;32(1314):3852-3862. doi:10.1111/jocn.16515
7. Lei Y, Shao Y, Wang L, et al. Large-scale brain network coupling predicts total sleep deprivation effects on cognitive capacity. PLoS One. 2015;10(7):e0133959. doi:10.1371/journal.pone.0133959
8. Marando I, Matthews RW, Grosser L, Yates C, Banks S. The effect of time on task, sleep deprivation, and time of day on simulated driving performance. Sleep. 2022;45(9):zsac167. doi:10.1093/sleep/zsac167
9. Curtis BJ, Williams PG, Anderson JS. Neural reward processing in self-reported short sleepers: examination of gambling task brain activation in the Human Connectome Project database. Sleep. 2019;42(9):zsz129. doi:10.1093/sleep/zsz129.
10. Fu J, Chen X, Gu Y, et al. Functional connectivity impairment of postcentral gyrus in relapsing-remitting multiple sclerosis with somatosensory disorder. Eur J Radiol. 2019;118:200-206. doi:10.1016/j.ejrad.2019.07.029
11. Zhou L, Tian N, Geng ZJ, Wu BK, Dong LY, Wang MR. Diffusion tensor imaging study of brain precentral gyrus and postcentral gyrus during normal brain aging process. Brain Behav. 2020;10(10):e01758. doi:10.1002/brb3.1758
12. Kato H, Izumiyama M. Impaired motor control due to proprioceptive sensory loss in a patient with cerebral infarction localized to the postcentral gyrus. J Rehabil Med. 2015;47(2):187-190. doi:10.2340/16501977-1900
13. Bigler ED, Mortensen S, Neeley ES, et al. Superior temporal gyrus, language function, and autism. Dev Neuropsychol. 2007;31(2):217-238. doi:10.1080/87565640701190841.
14. Dziobek I, Preissler S, Grozdanovic Z, Heuser I, Heekeren HR, Roepke S. Neuronal correlates of altered empathy and social cognition in borderline personality disorder. Neuroimage. 2011;57(2):539-548. doi:10.1016/j.neuroimage.2011.05.005
15. Hauser MD, Chomsky N FW. The Faculty of Language : What Is It , Who Has It , and How Did It Evolve ? Science (80- ). 2002;298(5598):1569-1579. doi:10.1126/science.298.5598.1569.
Figures
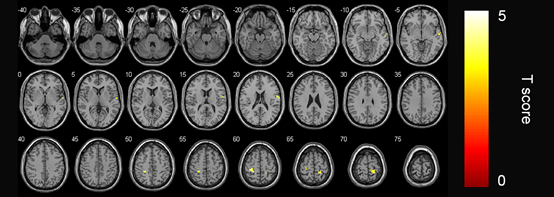
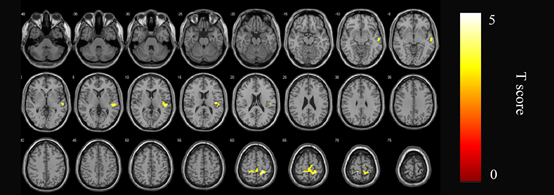
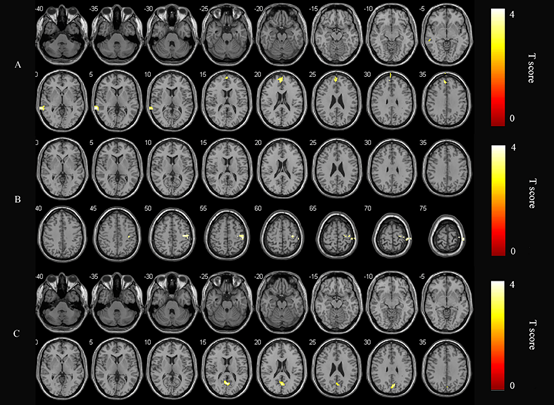

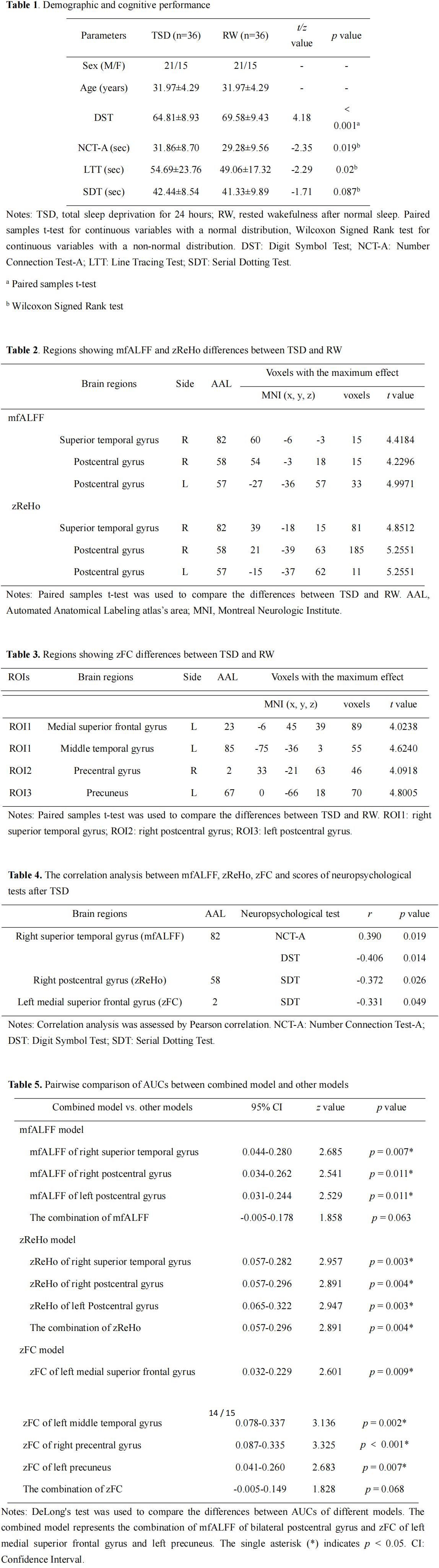
Table 1 summarizes the demographic details and their performance on neuropsychological tests.
Table 2: The analysis of mfALFF and zReHo (p<0.05, FDR corrected at the cluster level, initial voxel-wise threshold p=0.001.
Table 3: The analysis of FC (p<0.05, FWE corrected at the cluster level, initial voxel-wise threshold p=0.001).
Table 4: Pearson correlation analysis revealed significant correlations between rs-fMRI features and cognitive scores after TSD.
Table 5: The AUC of the combined model was higher than single-parameter model (p<0.05).