4228
Feasibility of Nipah virus-induced lesion detection using 0.05T MRI1Icahn School of Medicine at Mt. Sinai, New York, NY, United States, 2Integrated Research Facility at Fort Detrick, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Fort Detrick, MD, United States, 3Department of Radiology and Imaging Sciences, Clinical Center, National Institutes of Health,, Bethesda, MD, United States
Synopsis
Keywords: Infectious Disease, Infectious disease
Motivation: Portable, low-field MRI systems may represent the only viable strategy to monitor neurological manifestations of infectious diseases, such as Nipah virus (NiV), in vivo, and in low-resource settings.
Goal(s): To determine the optimal resolution for lesion detection at 0.05T and compare texture and area markers between 3T and 0.05T
Approach: We acquired 3T MR images of three NiV-exposed NHPs, simulated corresponding low-field images for lesion segmentation.
Results: We determined a minimum resolution requirement of 1.5 x 1.5 x 2 mm3 at 0.05T to manually segment NiV-induced brain lesions on T2w images and that 0.05T texture matches better with 3T data than lesion area.
Impact: The study determined the optimal resolution and textural feature required to monitor NiV-affected patients through prospective imaging at 0.05T to track lesions caused by NiV. It showed that textural was more consistent between the two field strengths than lesion area.
Introduction
High-consequence pathogens, such as Ebola, Lassa, and Nipah viruses (EBOV, LASV, NiV), are associated with acute or long-term neurological manifestations that can be visualized using MRI. However, high-field (HF) MRI scanners (3T or higher) commonly used for brain imaging are extremely difficult to deploy in geographic areas where disease outbreaks naturally occur or in their immediate proximity, for long-term monitoring of human survivors. Portable, very low-field (VLF) MRI systems may represent the only viable strategy to characterize and monitor neurological manifestations of infectious diseases in humans, in vivo, non-invasively, and in low-resource settings. In this work, we explore the feasibility of segmenting focal lesions detected in the brain of NiV-exposed NHPs using 3T MRI, and compare it to corresponding results from VLF-simulated images. We also demonstrate the feasibility of acquiring VLF in vivo data at the simulation-directed resolutions for lesion detection. This study will help develop methods to facilitate VLF MRI deployment in challenging settings to profile neurological sequelae of various infectious diseases.Methods
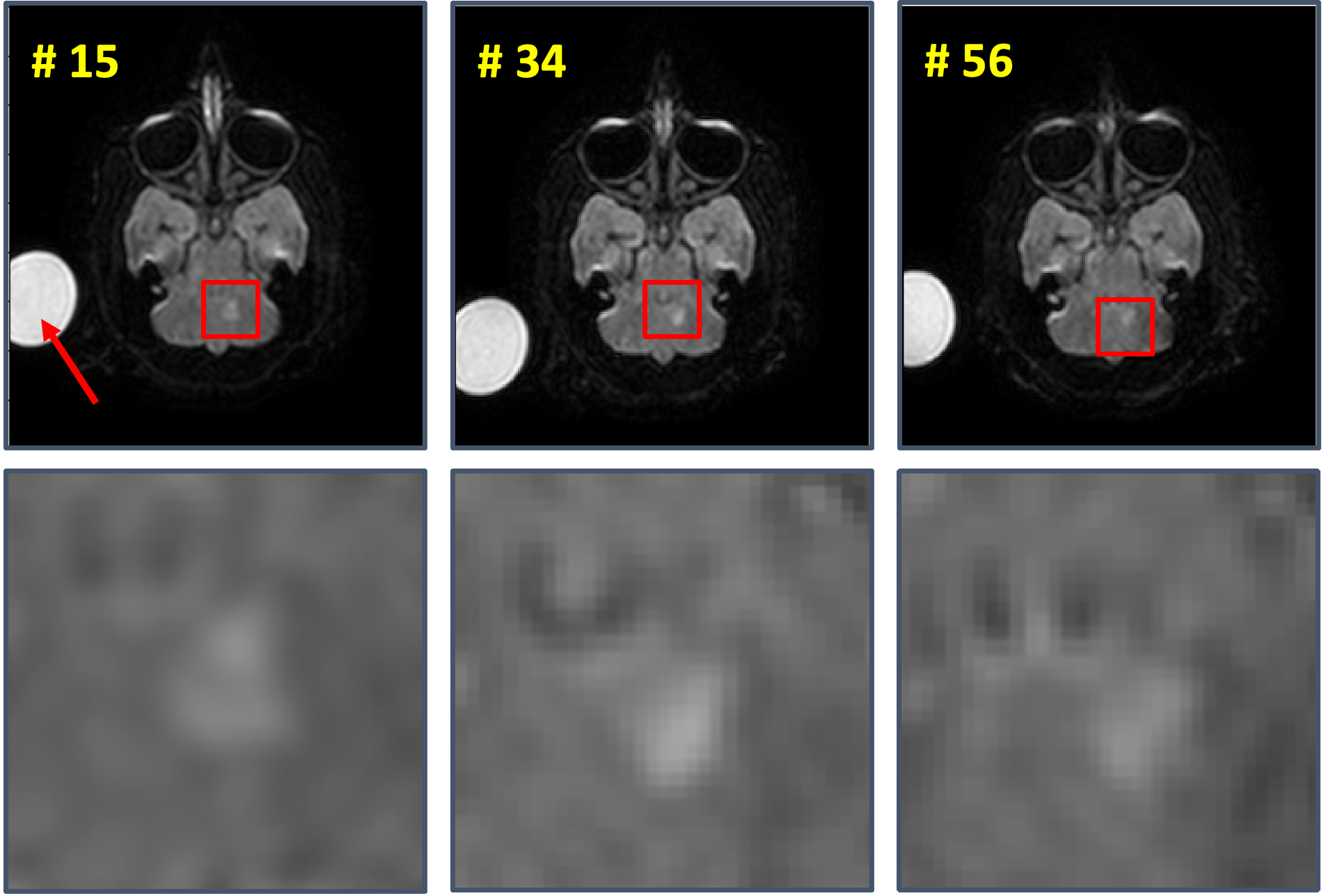
Animal model and study design: Three NHPs were exposed to a large-particle aerosol (12 µm) challenge of NiV (Malaysia isolate) at the target dose of approximately 500 plaque-forming units (confirmed by back-titration). Animals underwent brain MRI before and at several time points after virus exposure.MRI acquisition: Animals were imaged on a 3T Philips Achieva scanner. The acquisition parameters were: TR/TE = 10000/100 ms; field of view (FOV) = 112 x 112 x 60 mm3, with a flip angle (FA) of 90°, resolution of 0.5 x 0.5 x 2 mm3. All NHPs were subjected to imaging twice before the NiV exposure. Subsequent imaging was performed every 3 days after exposure for 2 weeks and then weekly until week 8 after exposure to track lesions. A representative lesion from NHP 3 for three chosen time points is shown in Figure 1.
VLF Simulation: We implemented a VLF simulation pipeline to translate 3T lesion analysis to 0.05T. Figure 2 shows the two steps of the VLF simulation of spatial resolution down-sampling and signal-to-noise ratio (SNR) reduction. VLF noise was then compiled based on cropping 16 voxel-wide corner signal intensities found in ten datasets of 3D Turbo Spin Echo acquired at 0.05T (Multiwave Technologies SA, France) after they had been normalized to the range of 0 to 1 and scaled by a factor of 5 to match VLF SNR, similar to the works on native noise in refs (6-8). This noise (σVLF acquired) was then scaled and added iteratively to the simulated data until the standard deviation of the simulated noise matched that of the acquired 0.05T data (σVLF Practical).
Validation of VLF simulation: We acquired a T2w image of the pro-MRI phantom on a 3T Siemens Skyra with a 0.75 x 0.75 x 5mm3 resolution. The same phantom was acquired on a 0.05T (Multiwave Technologies SA, France) using a 3D Turbo spin echo sequence. We passed the HF data into our LF simulator to mimic the 0.05T data for resolution and SNR. In the resize step of our simulations, we defined a target of 1.5mm x 1.5mm x 5mm in line with the 0.05T data resolution.
Lesion analysis: We used the simulator to investigate the effect of resolution at 0.05T required for lesion detection and characterization. We manually segmented the lesions at 3T and 0.05T simulated data, computed their areas and texture (variance of the gray level cooccurrence matrix)
Results
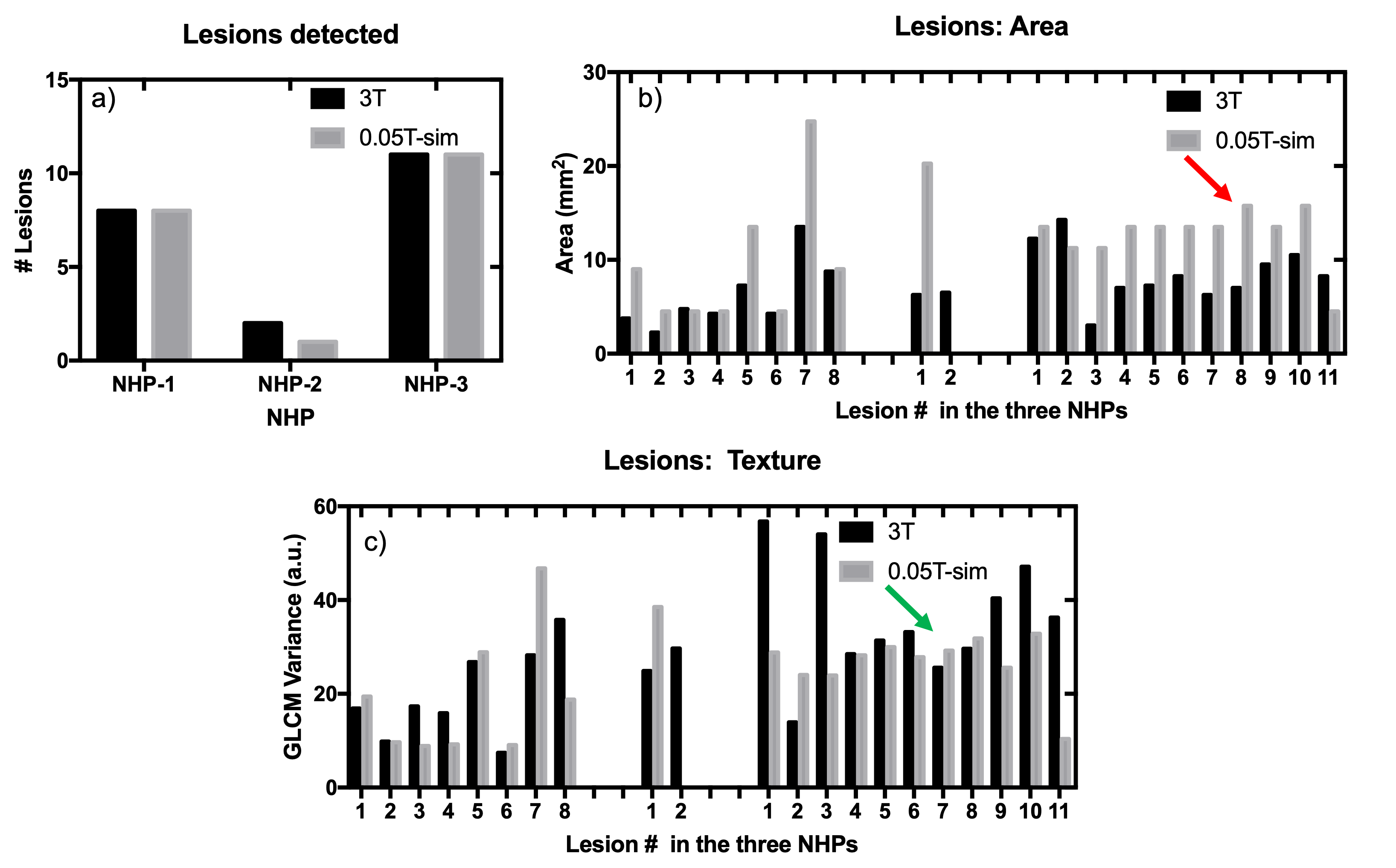
Figure 3 illustrates the results of the SNR simulation and validation, with the actual (23 a.u.) and simulated SNR (24 a.u.) being similar. The use of B0 mapping (3e) mitigated geometric distortion. The different spatial resolutions at the simulated 0.05T (Figure 4) show that a minimum of 1.5 x 1.5 x 2mm3 is required for manual lesion detection. At this resolution, a graduate student manually segmented 20 out of 21 lesions at the simulated 0.05T compared to 3T (Figure 5a). However, the loss of resolution resulted in increased errors in areas compared to 3T (red arrow, Figure 5b). This difference is reduced by using GLCM variance, as shown by the green arrow in Figure 5c.Conclusion and future work
We have determined an optimal resolution at 0.05T for lesion detection in this preliminary feasibility study. We used textural analysis as a translational imaging marker from 3T to 0.05T, across 21 lesions found in three NHPs. Future work involves prospectively imaging NiV-infected NHPs with more timepoints.Acknowledgements
No acknowledgement found.References
1. Chua, K.B., Bellini, W.J., Rota, P.A., Harcourt, B.H., Tamin, A., Lam, S.K., Ksiazek, T.G., Rollin, P.E., Zaki, S.R., Shieh, W.J. and Goldsmith, C.S., 2000. Nipah virus: a recently emergent deadly paramyxovirus. Science, 288(5470), pp.1432-1435.
2. Sharma, Vikrant, Sulochana Kaushik, Ramesh Kumar, Jaya Parkash Yadav, and Samander Kaushik. "Emerging trends of Nipah virus: A review." Reviews in medical virology 29, no. 1 (2019): e2010.
3. Lim, C.T., 2009. MR imaging in Nipah virus infection. Neurology Asia, 14(1), pp.49-52.
4. Sarji, S.A., Abdullah, B.J.J., Goh, K.J., Tan, C.T. and Wong, K.T., 2000. MR imaging features of Nipah encephalitis. American Journal of Roentgenology, 175(2), pp.437-442.
5. Geethanath, S. and Vaughan Jr, J.T., 2019. Accessible magnetic resonance imaging: a review. Journal of Magnetic Resonance Imaging, 49(7), pp.e65-e77.
6. Geethanath, S., Poojar, P., Ravi, K.S. and Ogbole, G., 2021, May. MRI denoising using native noise. In Proc Intl Soc Mag Reson Med (p. 2405).
7. Qian, E., Poojar, P., Vaughan Jr, J.T., Jin, Z. and Geethanath, S., 2022. Tailored magnetic resonance fingerprinting for simultaneous non‐synthetic and quantitative imaging: A repeatability study. Medical Physics, 49(3), pp.1673-1685.
8. Ravi, K. S., Nandakumar, G., Thomas, N., Lim, M., Qian, E., Jimeno, M. M., ... & Geethanath, S. (2023). Accelerated MRI using intelligent protocolling and subject-specific denoising applied to Alzheimer's disease imaging. Frontiers in Neuroimaging, 2, 1072759.
Figures