4225
Investigation of hippocampal subfield volumes in long COVID and ME/CFS using 7T MRI1National Centre for Neuroimmunology and Emerging Diseases, Griffith University, Gold Coast, Australia, 2The University of Queensland, Brisbane, Australia
Synopsis
Keywords: Infectious Disease, COVID-19, ME/CFS, hippocampus, infectious disease
Motivation: To study hippocampal atrophy in long COVID and Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS patients).
Goal(s): Our goal was to investigate hippocampal atrophy in long COVID and ME/CFS patients.
Approach: We used T1-weighted MP2RAGE data from 7T MRI and used FreeSurfer to estimate hippocampal subfield volumes in long COVID and ME/CFS patients.
Results: We found that hippocampal subfield volumes were larger in long COVID and ME/CFS patients compared to HC.
Impact: Our study showed atypical hippocampal atrophy in long COVID and ME/CFS patients indicating that existing brain research findings in ME/CFS patients may help better understand the neurological dysfunction in long COVID patients.
Introduction
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a complex illness that affects multiple body systems and is characterised by a range of symptoms including post-exertional malaise, neurocognitive impairment, or brain fog 1. Recently, coronavirus 2019 (SARS-COV-2) has infected more than 760 million worldwide causing Severe Acute Respiratory Syndrome Coronavirus 2 (SSARS-CoV-2) syndrome 2. It is estimated that at least 10% of COVID-19 infected people (76 million) develop long COVID 3. Studies show that 13-58% of long COVID patients met ME/CFS criteria 4 and exhibit symptoms of, neurocognitive impairment or brain fog. One of the main causes of neurocognitive impairment in long COVID and ME/CFS patients could be hippocampal atrophy because the hippocampus and its subfields play an important role in cognitive function and are also involved in memory function 5. Therefore, the specific aim of this study was to investigate structural changes of hippocampal subfields using ultra-high field 7T MRI in ME/CFS, long COVID, and healthy controls.Methods and Materials
The study was approved by the Griffith University Human Research Ethics Committee (ID: 2022/666), all the methods were carried out with the relevant guidelines and regulations following the Helsinki Declaration, and written informed consent was obtained from all individuals. We recruited 30 ME/CFS patients fulfilling the CCC and ICC criteria 6, 17 long COVID as defined by the WHO clinical case definition 7, and 15 age-matched HC subjects. MRI was performed on a 7 T whole-body MRI research scanner (Siemens Healthcare, Erlangen, Germany) with a 32-channel head coil (Nova Medical Wilmington, USA). We acquired T1-weighted data using a Magnetisation prepared 2 rapid acquisition gradient echo sequence (MP2RAGE). MP2RAGE data were acquired sagittally using the following parameters: repetition time (TR) = 4300 ms, echo time (TE) = 2.45 ms, inversion times: first (TI1) = 840 ms, second TI2 = 2370 ms, flip angles (FA1) = 5o, FA2 = 6o and spatial resolution = 0.75 mm3 with matrix size = 256 × 300 × 320. MP2RAGE images were anatomically segmented using FreeSurfer version 7.4.18 (https://surfer.nmr.mgh.harvard.edu/) using the default FreeSurfer command ‘recon-all’ on a Macintosh computer (Operating system: Catalina, RAM=36GB, and core: 8). Hippocampus subfields were segmented using the FreeSurfer 7.4.1 hippocampus subfield module. Using this module, the left and right hippocampal subfields: head, body, and tail; parasubiculum, presubiculum, subiculum, coronis ammonis (CA1, CA3, and CA4) head and body; granular cell layers of the dentate gyrus (GC-ML-DG), molecular layer of the hippocampus (HP), fissure, fimbria, and hippocampus-amygdala transition area (HATA) were defined. All hippocampal subfields were visually checked for distortion-free segmentation. One ME/CFS subject and two long COVID patients were excluded from the analysis due to inadequate segmentation. Multivariate general linear model (GLM) statistical analysis was performed to test for hippocampal subfield volume differences of ME/CFS and long COVID patients, relative to HC using SPSS version 29. After confirmation of homogeneity using Levene’s test, the multivariate GLM was used to test for three group differences. Correction for multiple comparisons was implemented using the Bonferroni method. Age, sex, and total intracranial volume were included as nuisance covariates for group comparisonsResults
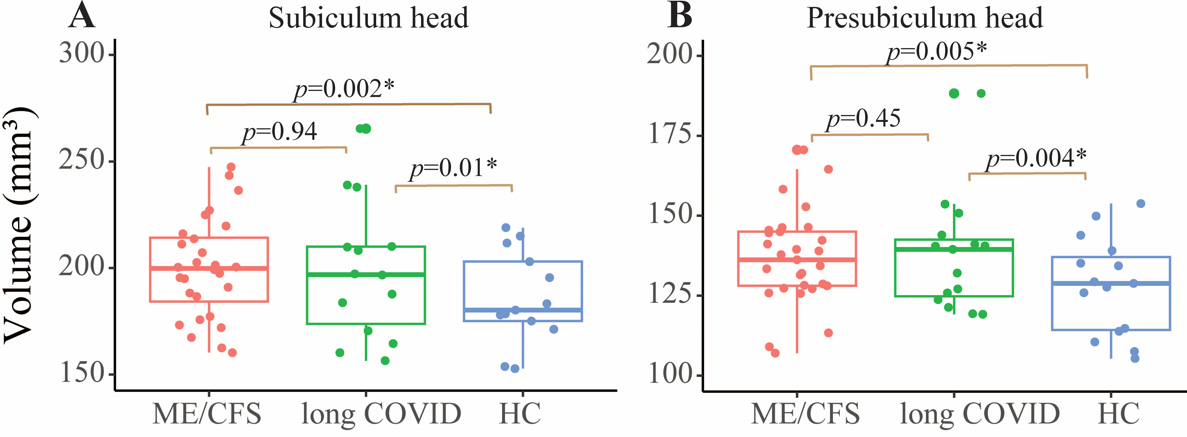
ME/CFS vs HCWe found significantly larger left subiculum head (p=0.002) and pre-subiculum head (p=0.005) volumes in ME/CFS patients compared to healthy controls (see Figure 1).
Long COVID vs HC
Long COVID patients also showed significantly larger left subiculum head (p=0.01) and presubiculum head (p=0.004) volumes compared to HC (see Figure 1).
ME/CFS vs long COVID
We found no significant differences in the hippocampal subfield volumes between ME/CFS and long COVID patients.
Discussion
Increased hippocampal subfield volumes may reflect neurogenesis. An increase in hippocampal neurogenesis could also be a response to the environmental factors and stress 9 that trigger ME/CFS and long COVID symptoms. The estimation of hippocampal subfield volume could also be affected by the implementation of different image processing pipelines. 10Conclusion
In summary, our analysis shows changed hippocampal subfield volumes in ME/CFS and long COVID patients with increments in the same hippocampal subfield volumes compared to HC. Therefore, existing brain research findings in ME/CFS patients may help better understand the neurological dysfunction in long COVID patients. Future research should study ME/CFS and long COVID patients together to get a better understanding of the neurological link between both cohorts.Acknowledgements
We are thankful to Ms. Tania Manning and Kay Schwarz for recruiting participants for this study. All radiographers at the University of Queensland, and the patients and healthy controls who donated their time and effort to participate in this study.References
1.Stussman, B. et al. Characterization of Post–exertional Malaise in Patients With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Neurol. 11, 1025 (2020).
2.WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int.
3.Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/20220622.htm (2022).
4.Twomey, R. et al. Chronic Fatigue and Postexertional Malaise in People Living With Long COVID: An Observational Study. Phys. Ther. 102, pzac005 (2022).
5.Middlebrooks, E. H. et al. The hippocampus: detailed assessment of normative two-dimensional measurements, signal intensity, and subfield conspicuity on routine 3T T2-weighted sequences. Surg. Radiol. Anat. 39, 1149–1159 (2017).
6. Carruthers, B. M. et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 270, 327–338 (2011).
7. A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021. https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1.
8.Fischl, B. FreeSurfer. NeuroImage 62, 774–781 (2012).
9.Toda, T., Parylak, S., Linker, S. B. & Gage, F. H. The role of adult hippocampal neurogenesis in brain health and disease. Mol. Psychiatry 24, 67–87 (2019).
10.Shaw, T. et al. Longitudinal Automatic Segmentation of Hippocampal Subfields (LASHiS) using multi-contrast MRI. NeuroImage 218, 116798 (2020).
Figures