4216
The hemodynamic and geometric mechanisms of carotid artery atherosclerotic plaques formation1Lanzhou University Second Hospital, Lanzhou, China, 2Philips Healthcare, Xi’an, China
Synopsis
Keywords: Vessels, Atherosclerosis, Carotid artery, Hemodynamic, Geometric
Motivation: Carotid artery geometry and hemodynamics are considered as potential imaging markers of atherosclerotic plaque formation risk.
Goal(s): 4D flow MRI has been widely used in large blood vessels of the heart, with relatively few applications in head and neck blood vessels.
Approach: This study, 4D flow MRI was used to evaluate the carotid artery hemodynamics, and the geometric characteristics were fused to explore the hemodynamic and geometric mechanism of carotid plaque formation.
Results: The large bifurcation angle and the low tortuosity are geometric risk factors for carotid bifurcation plaque formation. Low PG and low WSS are hemodynamic factors promoting plaque formation.
Impact: 4D flow MRI can directly measure very comprehensive hemodynamic parameters in vivo from any direction and angle during different cardiac cycles, and can visualize blood flow direction and status. However, it is not widely accepted in clinical practice.
The latest data from the Global Burden of Disease Study (GBD) shows that stroke is the primary cause of death and disability in adults in China, bringing a huge economic burden to patients and society[1]. Atherosclerosis is the most common cause of ischemic stroke. Systemic arteries are exposed to systemic risk factors of atherosclerosis, such as age, gender, hyperlipidemia, hypertension, hyperglycemia, smoking and obesity, but atherosclerosis plaque has specific predilection sites[2].The bifurcation of the common carotid artery is the most common location of carotid atherosclerotic plaque[3]. In this study, 4D flow MRI was used to evaluate the carotid artery hemodynamics, and the geometric of the carotid artery was fused to explore the hemodynamic and geometric mechanism of carotid atherosclerotic plaque formation.
Methods
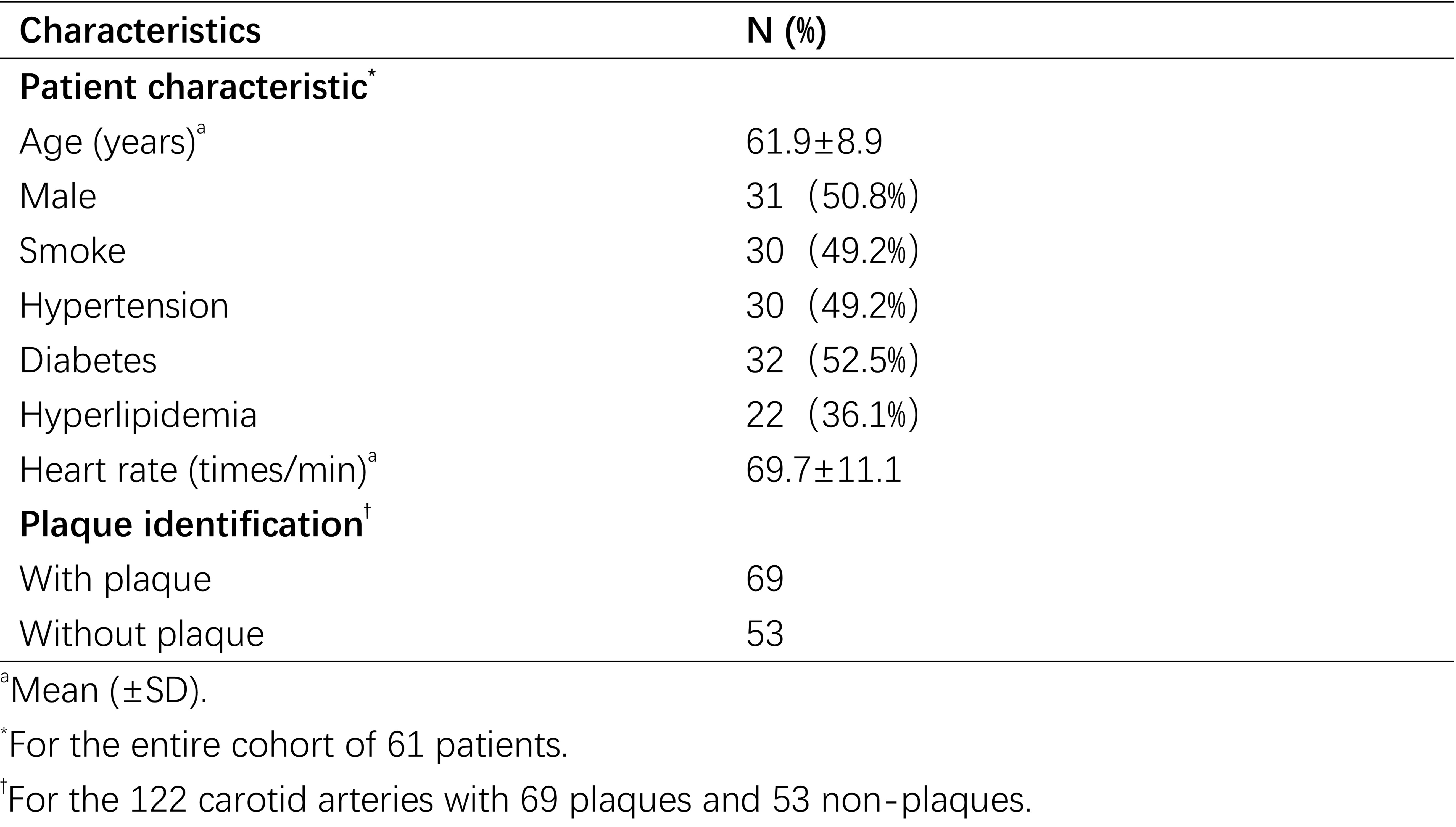
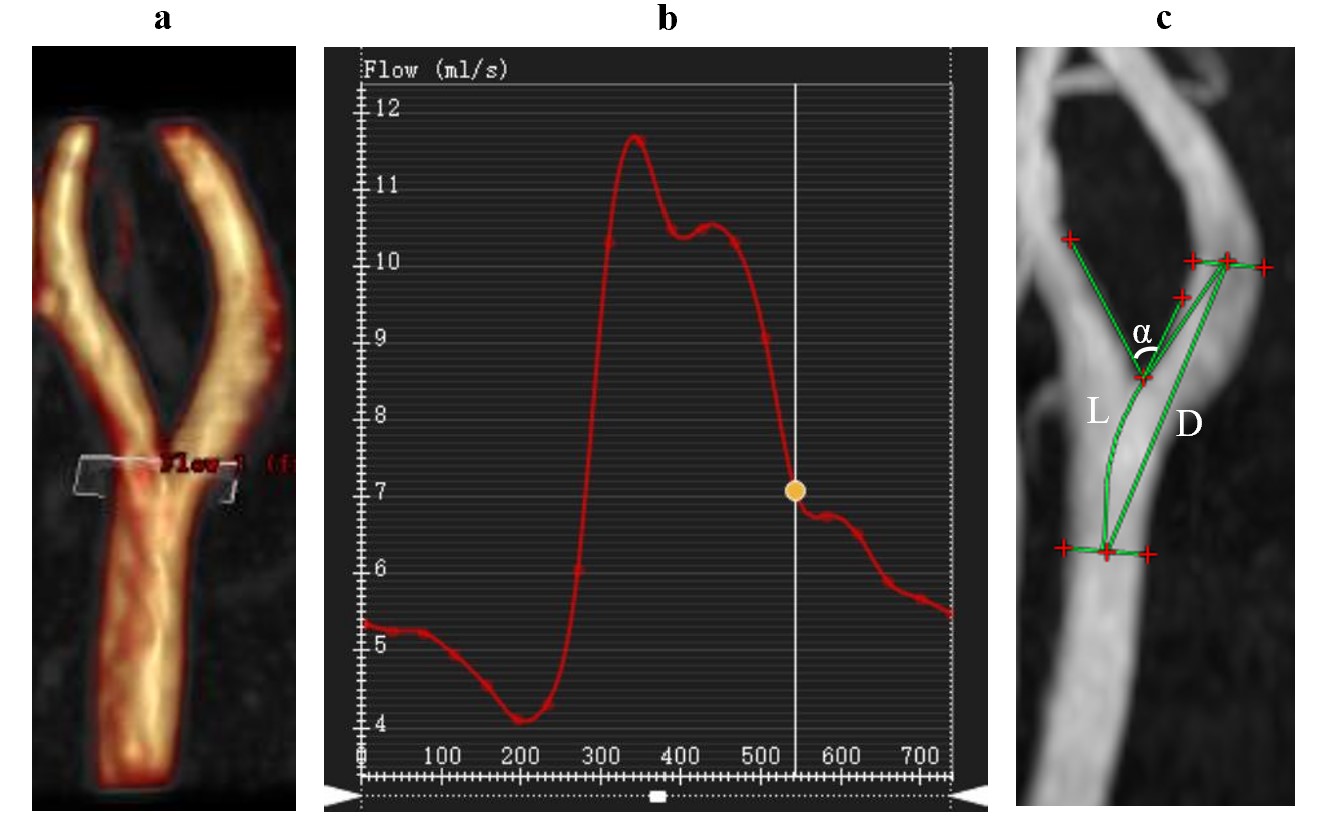
122 carotid arteries of 61 patients were included and divided into plaque group(N=69) and non-plaque group(N=53). The 4D flow MRI scans were performed using a 3.0T MRI scanner (Ingenia CX, Philips Healthcare, the Netherlands) with a tirty-two channel head–neck coil. The 4D flow MRI was acquired using a volumetric and a time-resolved PC method. The scanning parameters were as follows:FOV=240×240mm2,TR/TE=5.6/2.9ms,Flip angle=8°, Velocity encoding(VENC)=100cm/s, The total scan time of the 4D flow was approximately 12−15 minutes depending on the heart rate of each subject. The 4D flow datasets were imported into the CVI-42 platform (Version 5.6.6, Circle Cardiovascular Imaging, Canada) for further analysis. As displayed in Fig.1a and b, we placed plane in the bifurcation of common carotid artery to evaluate hemodynamics (Volume, Velocitymax, Axial WSSmean, Circumferential WSSmean, 3D WSSmax, 3D WSSmean, PGmax, PGmean). Measurement of carotid artery geometry based on 3D-TOF MRA as displayed in Fig.1c. The measured geometric parameters include: a) ICA/CCA-ratio: the ratio of ICA maximum inner diameter to CCA maximum inner diameter; b) Bifurcation angle: measured along two tangent lines along the outer wall of internal and external carotid arteries, using α represent; c) Tortuosity: The curvature of the carotid artery is evaluated by the ratio of the straight distance (D) to the distance along the center of the lumen (L) of CCA-ICA. Statistical analysis was performed using GraphPad Prism (version 9.0) software. Independent two sample t-tests were used to detect carotid artery geometry and hemodynamic changes among plaque group and non-plaque group. P<0.05 was considered statistically significant.
Results
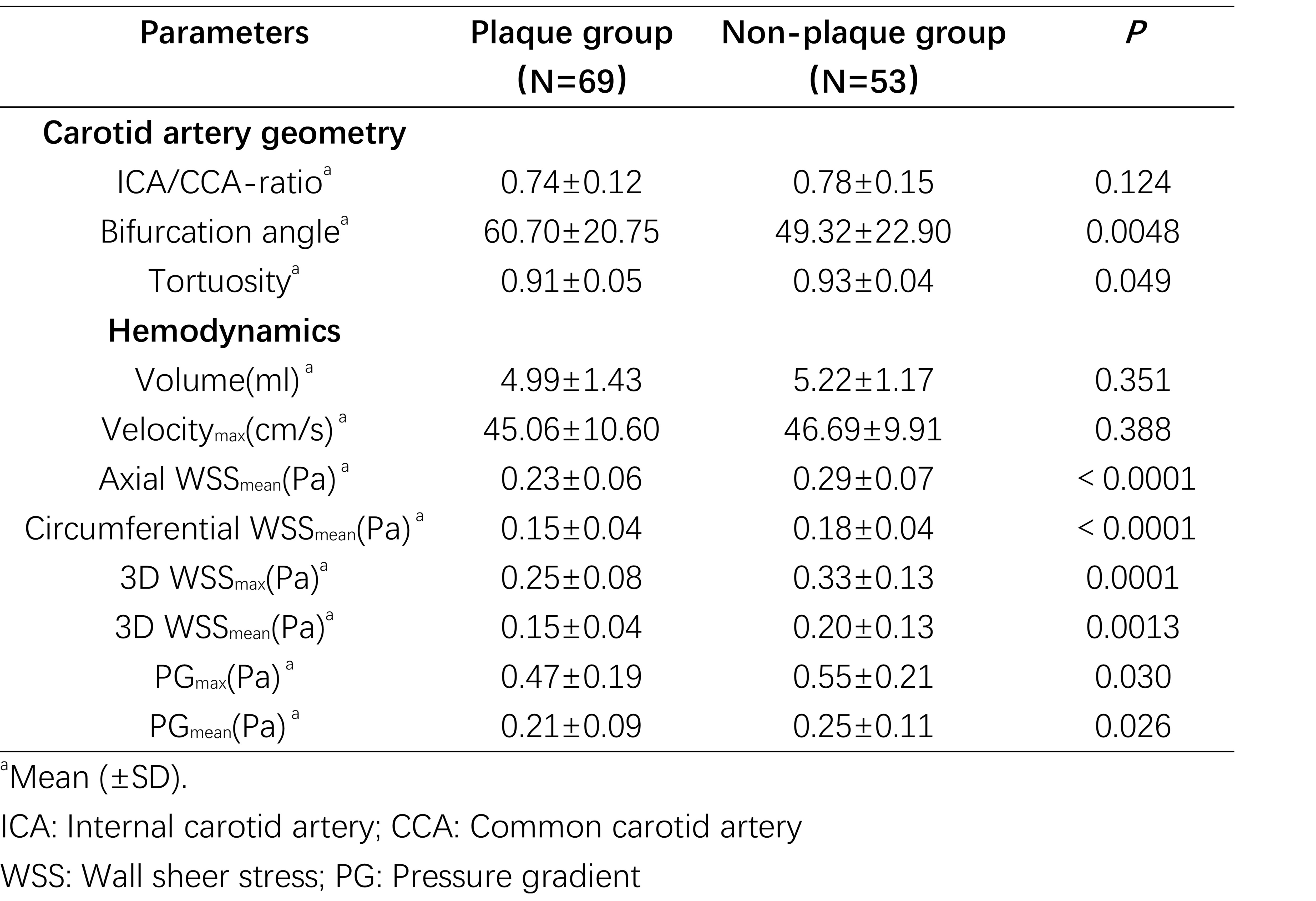
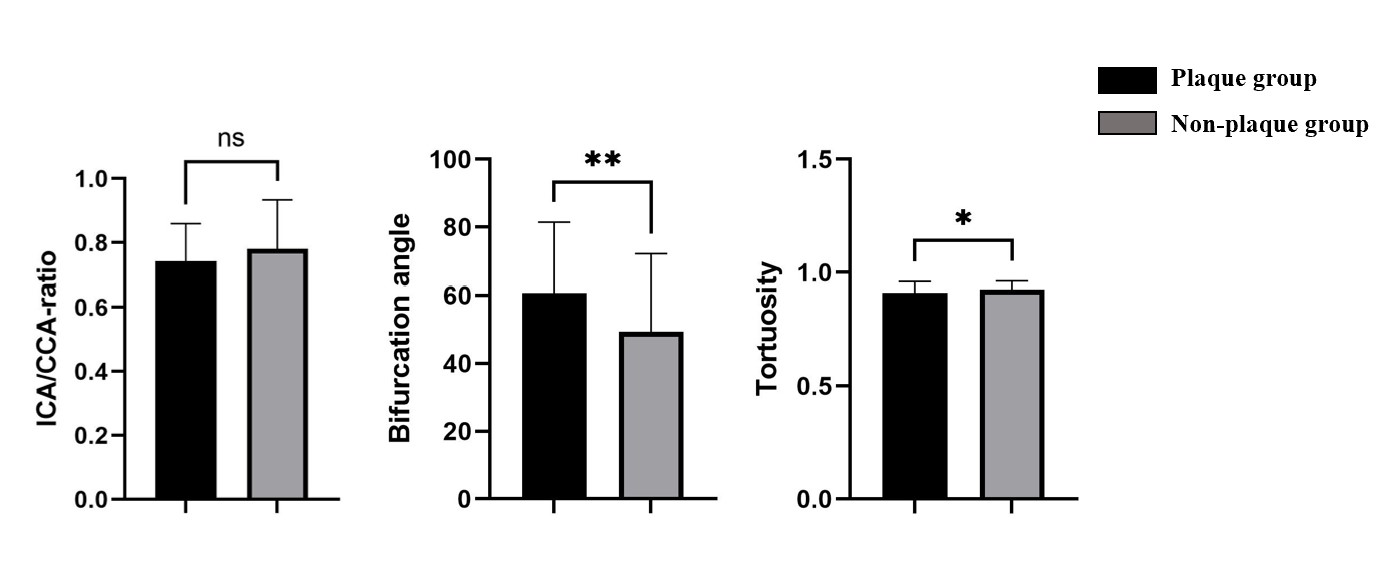
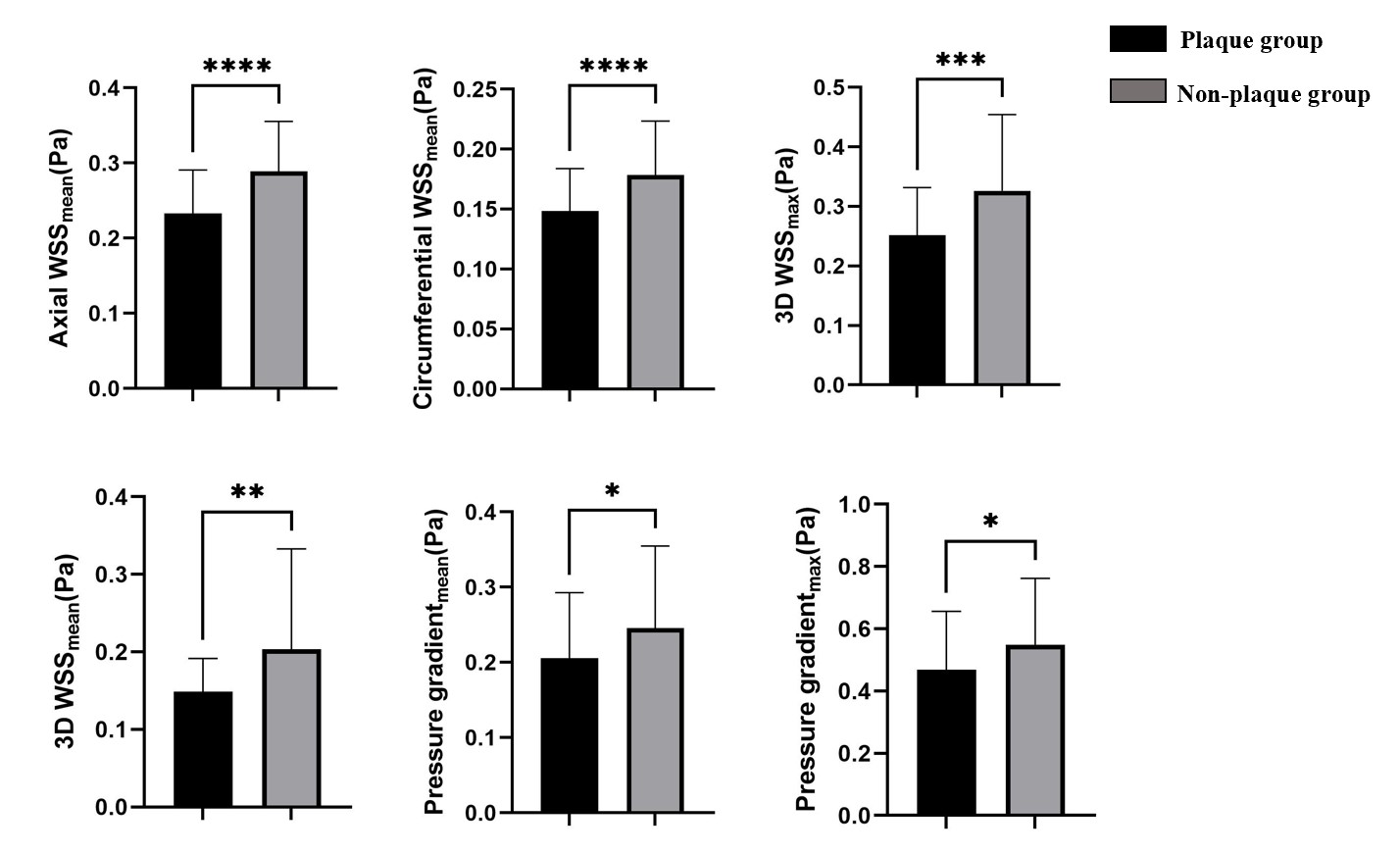
122 carotid arteries of 61 patients were included and divided into plaque group(N=69) and non-plaque group(N=53). The patient demographic data were listed in Table1. Carotid artery geometry and hemodynamic of plaque group and non-plaque group were displayed in Table2. There were statistically significant differences in bifurcation angle, tortuosity, axial WSSmean, circumferential WSSmean, 3D WSSmax, 3D WSSmean, PGmax and PGmean between the two groups(P<0.05),as displayed in Fig.2 and Fig.3.
Discussion
The high tortuosity of the carotid artery has a protective effect on patients with carotid atherosclerosis, because the increase of eddy current inhibits turbulence. A larger bifurcation angle of the CCA, a lower PG and WSS of the carotid artery are more likely to form plaques. Few studies use PG value to detect the formation of plaque. One study compared the PG value of healthy people and patients with carotid atherosclerotic stenosis, and found that the PG value of patients with stenosis was low[4]. In addition, there are also studies that show that the PG value decreases with age, and old age is one of the risk factors for atherosclerotic plaque formation[5]. Therefore, it indirectly indicates that low PG value can promote plaque formation. Low WSS increases the uptake of low-density lipoprotein, leading to the formation of lipid components in plaques. In addition, low WSS value changes the blood flow pattern of vascular endothelium at the molecular and cellular levels, and all these reactions promote the formation of atherosclerotic plaque[6].
Conclusion
As an initial and exploratory study, this work showed that the large bifurcation angle of the CCA and the low tortuosity of the carotid artery are geometric risk factors for plaque formation in carotid bifurcation. Low PG and WSS are hemodynamic factors promoting plaque formation.
Acknowledgements
Gansu Province Clinical Research Center for Functional and Molecular Imaging (Project Number: 21JR7RA438).
References
[1]Chen Y, Wright N, Guo Y, et al. Mortality and recurrent vascular events after first incident stroke: a 9-year communitybased study of 0.5 million Chinese adults[J]. Lancet Glob Health, 2020, 8(4): e580-e590.
[2]SONG J W, WASSERMAN B A. Vessel wall MR imaging of intracranial atherosclerosis[J]. Cardiovasc Diagn Ther, 2020, 10(4): 982-993.
[3]LU M, ZHANG L, YUAN F, et al. Comparison of carotid atherosclerotic plaque characteristics between symptomatic patients with transient ischemic attack and stroke using high-resolution magnetic resonance imaging[J]. BMC Cardiovasc Disord, 2022, 22 (1): 190.
[4]Zhang G, Wang Z, Zhang S, et al. Age and anatomical location related hemodynamic changes assessed by 4D flow MRI in the carotid arteries of healthy adults[J]. European Journal of Radiology, 2020, 128:109035.
[5]F.M. Callaghan, P. Bannon, E. Barin, D. Celemajer, R. Jeremy, G.Figtree, S.M. Grieve, Age-related changes of shape and flow dynamics in healthy adult aortas: a 4D flow MRI study, J. Magn. Reson. Imaging, 2019, 49 (1) : 90–100.
[6]Zhang, G., et al., Differences in Wall Shear Stress Between High-Risk and Low-Risk Plaques in Patients With Moderate Carotid Artery Stenosis: A 4D Flow MRI Study. Frontiers in Neuroscience, 2021. 15.
Figures