4215
MRA Derived Cerebral Arterial Flow Features Associated with White Matter Hyperintensity1Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 2Key Laboratory of Computational Neuroscience and Brain-Inspired Intelligence (Fudan University), Ministry of Education, Shanghai, China, 3Department of Materials Science, Fudan University, Shanghai, China, 4Department of Neurology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, China, 5USC Viterbi School of Engineering, University of Southern California, Shanghai, China, 6Laboratory of FMRI Technology, USC Mark & Mary Stevens Neuroimaging and Informatics Institute, Keck School of Medicine, University of Southern California, Shanghai, China, 7Department of Neurology, Zhongshan Hospital, Fudan University, Shanghai, China
Synopsis
Keywords: Blood Vessels, Blood vessels, White matter hyperintensity, hemodynamic
Motivation: The morphology of cerebral arteries contributes to the development of white matter hyperintensity (WMH), yet the influence of arterial blood flow on WMH remains unclear.
Goal(s): Identify associations of cerebral arterial flow features with WMH.
Approach: 2631 individuals were involved. Arterial flow features were obtained using the individual-specific simplified hemodynamic model. WMHs were quantified from T2-FLAIR images.
Results: Both increased mean flow rate and pressure were associated with increased WMH volume. Adjacent Lesion Terminal Arterial Branches exhibited greater length, tortuosity, lower mean flow rates and pressure drops.
Impact: The hemodynamic features surrounding WMH exhibited significant difference compared to distant arteries. Such morphology and corresponding hemodynamic changes might contribute to the development of WMH.
Introduction
Cerebral small vessel disease is a pathological condition predominantly affecting small vessels in the brain, leading to various physiological and cognitive abnormalities, including white matter hyperintensities (WMH)1,2. As an organ with a profound demand for blood supply, the brain is highly sensitive to variations in blood flow3. Studies have highlighted that subtle alterations in cerebral blood flow could have significant implications on cognitive functions and overall brain health4-6. To investigate the complex nature of cerebral arterial hemodynamics and relations with WMH, the individual-specific simplified hemodynamic model was employed in a large group of patients free of stroke, to identify the association of arterial flow features with WMH.Methods
This study retrospectively enrolled 2631 participants, free of acute stroke and large artery stenosis from Yueyang hospital, Shanghai, China. Brain MRI scans were completed on one 3T MR scanner (Philips). Figure 1 summarized the participants characteristics. The MRI protocol included T1-weigthed imaging (TE = 2.3ms, TR = 250ms, flip angle = 75°, matrix size = 512×512×18, voxel size = 0.45mm×0.45mm×6mm), T2-FLAIR (TE = 120ms, TR = 7000ms, flip angle = 90°, matrix size = 384×384×18, voxel size = 0.6mm×0.6mm×6mm) and TOF MRA (TE = 3.5ms, TR = 23ms, flip angle = 18°, matrix size = 560×560×112, voxel size = 0.375mm×0.375mm×0.8mm). This study was approved by the local ethics committee. WMH lesions were segmented automatically by the lesion prediction algorithm in the LST toolbox (www. statistical-modelling.de/lst.html) from T2-FLAIR images. WMH lesions were divided into PWMH or DWMH according to the distance from the lateral ventricles (>10 mm was considered to be deep WMH)7. The cerebral arterial blood flow was simulated using a patient-specific simplified hemodynamic model with following procedures (Figure 2)8,9: (1) Cerebral vessel segmentation was completed on MRA images using the previously described methods. 10 (2) The centerlines of vessels were extracted using the Skeleton 3D toolbox. The topological connections among vascular branches were organized by evaluating the adjacency of centerline points. The inflow branches were manually identified, while all outflow branches were automatically obtained through the topological connections. (3) The flow and pressure drop of each vascular branch was related according to the Hagen-Poiseuille equation. Both the inflow and outflow pressure of each branch were served as unsolved variables and three sets of boundary conditions were established. For inlet, the mean arterial pressure was served as a boundary condition. For outlet, a patient-specific structured tree was built for each outflow branch until the diameter of the terminal branches in the structured tree was less than 0.1 mm11. For bifurcation, the incoming flow was equal to the outgoing flow and pressure was assuming continuity. Since all the governing equations were linear, the flow features for each vascular branch were directly obtained using matrix inversion methods. Afterwards, three flow features of each vascular branch, including flow rate, mean pressure (the mean of inlet and outlet pressures), and pressure drop (the difference between inlet and outlet pressures), were quantified. Moreover, a threshold was established to define Adjacent Lesion Terminal Arterial Branches (ALTAB), which was defined as a terminal arterial branch visible in TOF images within a certain distance around the WMH lesions.Results and Discussion
In general, higher mean flow rate and pressure were found to be associated with increased total WMH volume after adjusting potential confounding variables as shown in the Figure 3. This relationship might not contradict the negative association between cerebral perfusion blood flow and WMH. Perfusion blood flow quantified the metabolic intensity of small vessel networks. Reduced flow in small vessels might stimulate compensatory dilation in large vessels, leading to increased flow in large arteries12,13. However, WMH lesions might disrupt the metabolic and blood flow accommodation capacity of the small vessel network, failing to ensure effective perfusion of small vessels despite large artery dilation, resulting in increased large artery flow but reduced cerebral perfusion blood flow. A mean value of 13mm from the vascular boundary to the lesion boundary was used as the demarcation for ALTAB. As presented in Figure 4, compared to other terminal arterial branches, ALTABs exhibited greater length (21.7±8.21mm vs 13.3±2.35mm, p<0.001) and tortuosity (1.52±0.39mm vs 1.26±0.11mm, p<0.001). In terms of flow features, ALTABs had lower mean flow rates (0.40±0.09mm vs 0.90±0.25mm, p<0.001) and pressure drops (0.42±0.16mm vs 0.54±0.15mm, p<0.001). Despite ALTABs in this study were only spatially closer to WMH lesions and might not represent the actual arteries supplying the WMH lesions, their spatially proximity might facilitate the transfer of arterial pulsatile damage to the lesion area, potentially influencing the development of the lesion.Acknowledgements
We are greatly thankful to all the members in our research group at Fudan University and Yueyang Hospital who helped to accomplish the study. This work was supported by the National Natural Science Foundation of China (No. 81971583, No. 82271956), Shanghai Municipal Science and Technology Major Project (No. 2018SHZDZX01), National Key R&D Program of China (No. 2018YFC1312900).References
1. Debette S, Schilling S, Duperron MG, Larsson SC, Markus HS. Clinical significance of magnetic resonance imaging markers of vascular brain injury a systematic review and meta-analysis. Jama Neurology. 2019;76:81-94
2. Wardlaw JM, Smith C, Dichgans M. Small vessel disease: Mechanisms and clinical implications. Lancet Neurology. 2019;18:684-696
3. Ma Y, Song A, Viswanathan A, Blacker D, Vernooij MW, Hofman A, et al. Blood pressure variability and cerebral small vessel disease a systematic review and meta-analysis of population-based cohorts. Stroke. 2020;51:82-89
4. Sun YW, Cao WW, Ding WN, Wang Y, Han X, Zhou Y, et al. Cerebral blood flow alterations as assessed by 3d asl in cognitive impairment in patients with subcortical vascular cognitive impairment: A marker for disease severity. Frontiers in Aging Neuroscience. 2016;8
5. Duschek S, Schandry R. Deficient adjustment of cerebral blood flow to cognitive activity due to chronically low blood pressure. Biological Psychology. 2006;72:311-317
6. Claassen J, Thijssen DHJ, Panerai RB, Faraci FM. Regulation of cerebral blood flowin humans: Physiology and clinical implications of autoregulation. Physiological Reviews. 2021;101:1487-1559
7. Griffanti L, Jenkinson M, Suri S, Zsoldos E, Mahmood A, Filippini N, et al. Classification and characterization of periventricular and deep white matter hyperintensities on mri: A study in older adults. Neuroimage. 2018;170:174-181
8. Zhu J, Teolis S, Biassou N, Tabb A, Jabin P-E, Lavi O. Tracking the adaptation and compensation processes of patients’ brain arterial network to an evolving glioblastoma. IEEE transactions on pattern analysis and machine intelligence. 2020;44:488-501
9. Helthuis JH, van Doormaal TP, Amin-Hanjani S, Du X, Charbel FT, Hillen B, et al. A patient-specific cerebral blood flow model. Journal of Biomechanics. 2020;98:109445
10. Zhang B, Wang Y, Wang B, Chu YH, Jiang Y, Cui M, et al. Mri‐based investigation of association between cerebrovascular structural alteration and white matter hyperintensity induced by high blood pressure. Journal of Magnetic Resonance Imaging. 2021;54:1516-1526
11. Olufsen MS, Peskin CS, Kim WY, Pedersen EM, Nadim A, Larsen J. Numerical simulation and experimental validation of blood flow in arteries with structured-tree outflow conditions. Annals of biomedical engineering. 2000;28:1281-1299
12. Sugimori H, Ibayashi S, Irie K, Ooboshi H, Nagao T, Fujii K, et al. Cerebral hemodynamics in hypertensive patients compared with normotensive volunteers. A transcranial doppler study. Stroke. 1994;25:1384-1389
13. Zhang B, Huo Y, Yang Z, Lv H, Wang Y, Feng J, et al. Day to day blood pressure variability associated with cerebral arterial dilation and white matter hyperintensity. Hypertension. 2022;79:1455-1465
Figures
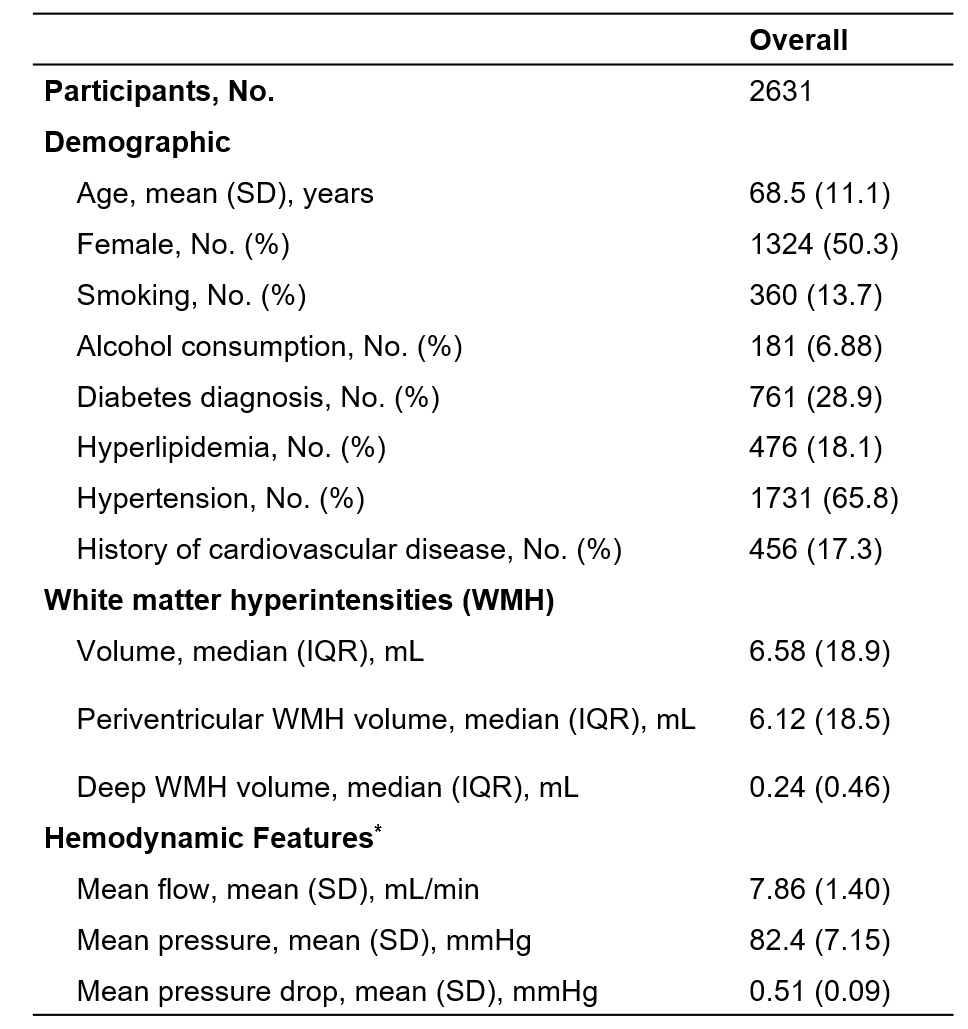
* The hemodynamic features refer to the mean values of the hemodynamic features of all arterial branches visible in MRA images.
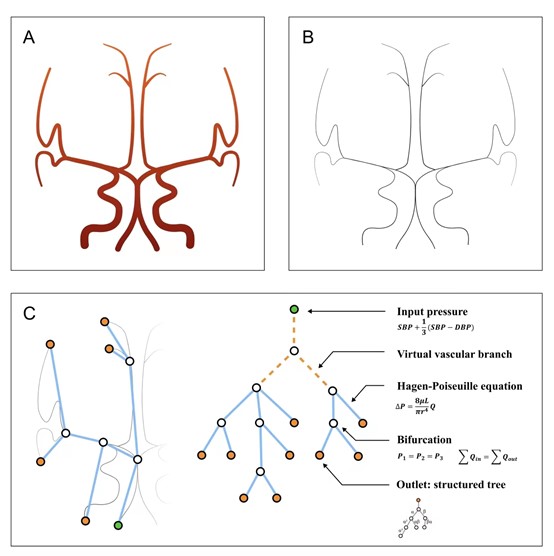
Figure 2. Schematic representation of the simplified hemodynamic model implementation.
A) Cerebral arterial vessel segmentation; B) centerline extraction; C) simplified hemodynamic model.
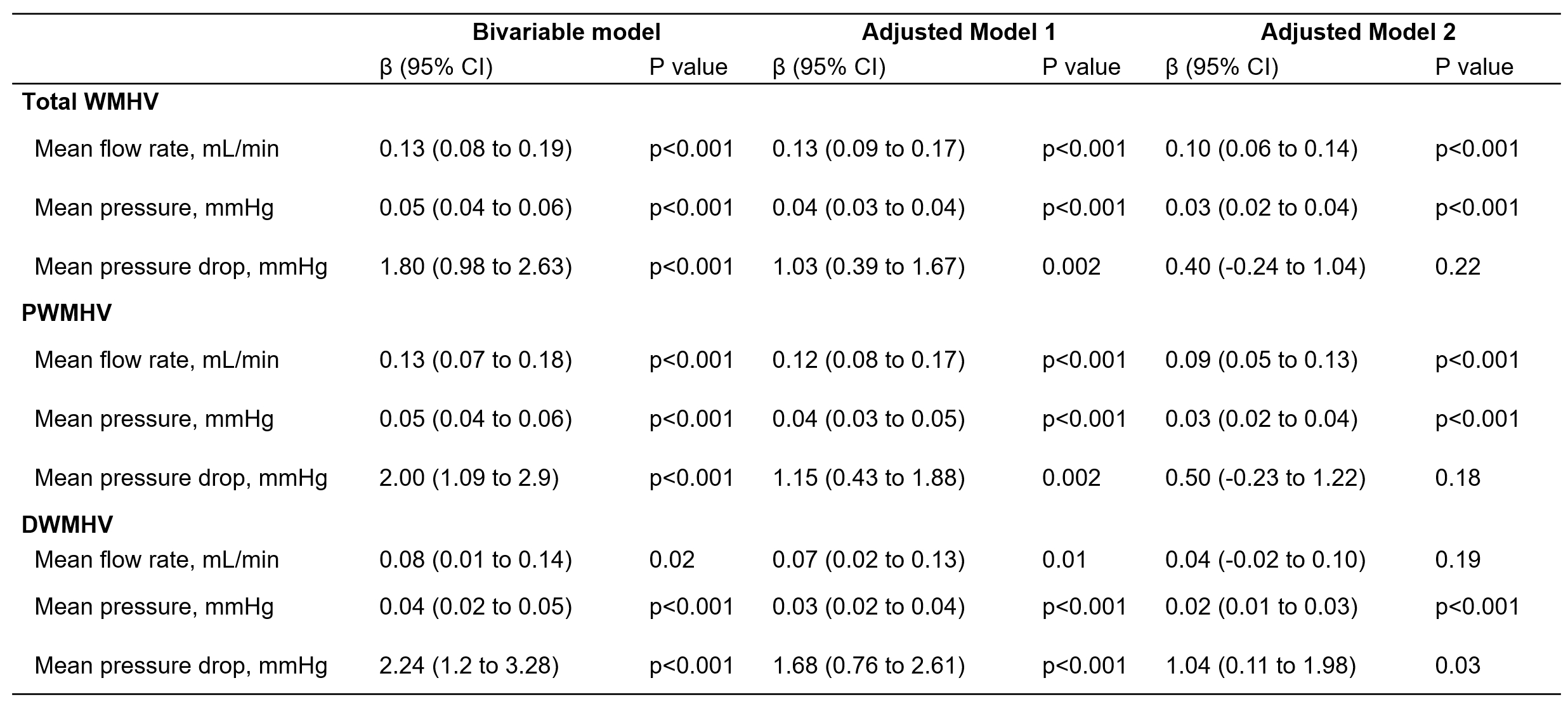
Model 1 adjusted for age and sex; Model 2 adjusted for age, sex and vascular risk factors including cigarette use, alcohol consumption, diabetes, hyperlipidaemia, hypertension and history of cardiovascular disease. DWMHV, deep white matter hyperintensity lesion volume; PWMHV, periventricular white matter hyperintensity lesion volume; and WMHV, white matter hyperintensity lesion volume.
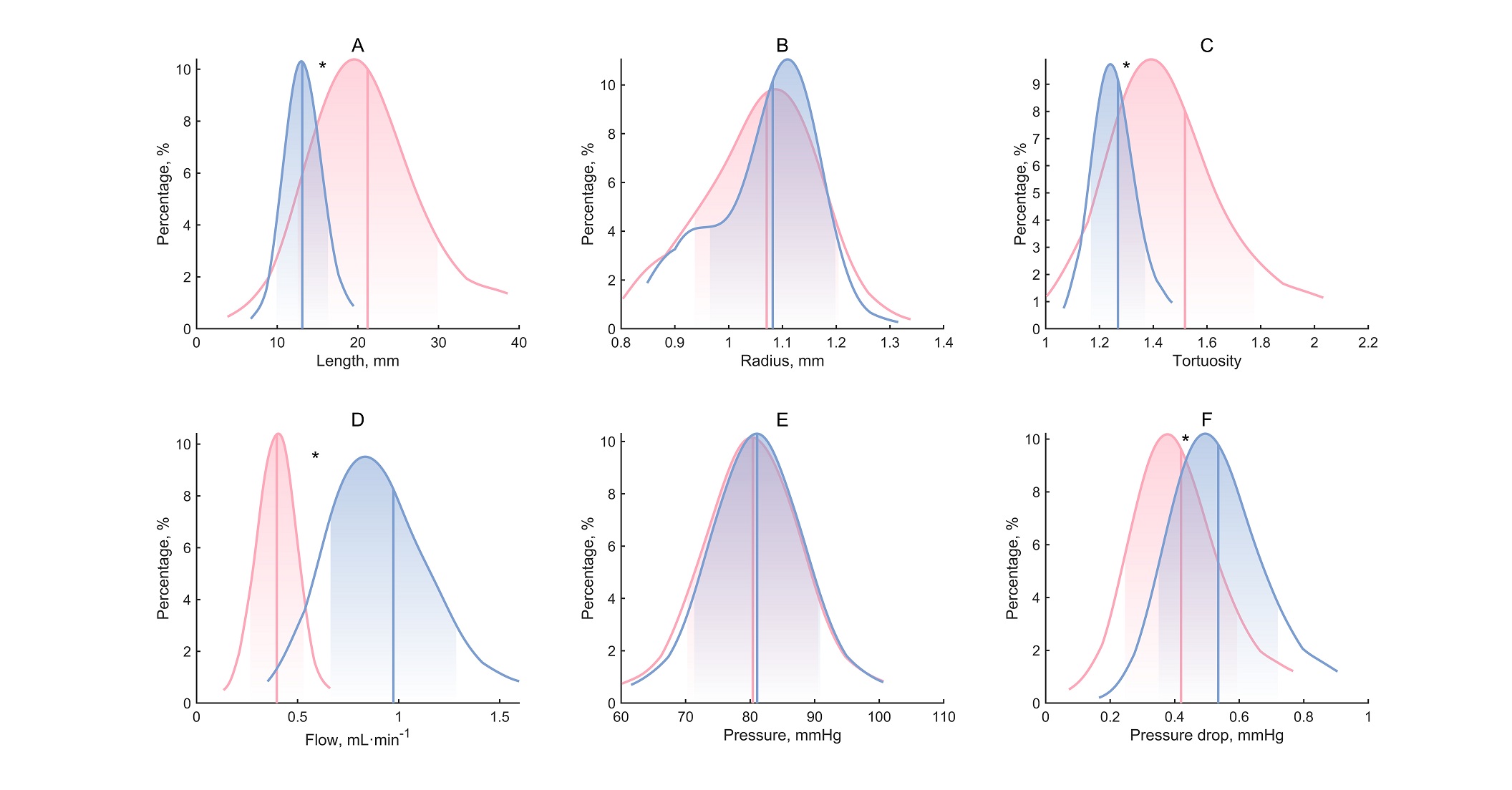
The red section represents Adjacent Lesion Terminal Arterial Branches, while the blue section represents other terminal branches. The vertical solid line represents the median, and the shaded area indicates the interquartile range. The asterisk indicates a significant difference.