4194
7 Tesla MRI in routine surgical planning for Deep Brain Stimulation for Parkinson’s Disease1Spinoza Centre for Neuroimaging, Amsterdam, Netherlands, 2Computational Cognitive Neuroscience and Neuroimaging, Netherlands Institute for Neuroscience, KNAW, Amsterdam, Netherlands, 3Department of Radiology and Nuclear Medicine, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Netherlands, 4Department of Neurosurgery, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Netherlands, 5Department of Biomedical Engineering and Physics, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Netherlands, 6Department of Neurology, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam Neuroscience, Amsterdam, Netherlands
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease, Deep Brain Stimulation; Subthalamic Nucleus; Ultra-High Field MRI
Motivation: Identifying the dorsolateral subthalamic nucleus (STN) for deep brain stimulation (DBS) in Parkinson’s disease (PD) can be challenging due to the size and double-oblique orientation.
Goal(s): To evaluate the influence of 7T T2w-TSE and probabilistic tractography on STN target planning, micro-electrode recordings and motor improvement.
Approach: We describe the implementation of 7T T2w-TSE and probabilistic tractography in 182 PD patients undergoing STN DBS at our centre from 2015-2022.
Results: Implementation of 7T T2w-TSE for STN DBS enabled a refinement in targeting which can be used as basis for adding probabilistic subthalamic connectivity, in order to enhance clinical outcome of STN DBS.
Impact: The extensive evaluation of 360 STNs has not been described previously and shows 7T T2w-TSE and probabilistic tractography can refine STN targeting and surgical efficiency in DBS for PD.
Background
Identifying the dorsolateral subthalamic nucleus (STN) for deep brain stimulation (DBS)1 in Parkinson’s disease (PD) can be challenging due to the size and double-oblique orientation. Since 2015 we implemented 7-Tesla T2-weighted (7T T2w) turbo-spin-echo (TSE) magnetic resonance imaging for improving visualization and targeting of the dorsolateral STN. In addition to T2-weighted imaging, we recently implemented 7T diffusion weighted (DWI) sequences for enabling probabilistic tractography-derived 7T segmentation and succeeded in visualizing the motor STN. It remains unclear if DBS electrodes placed in the 7T segmented motor STN achieve superior motor improvement and whether microelectrode recording (MER)2 can accurately distinguish the motor subdivision.Methods
1. By comparing two cohorts of STN DBS patients in different time periods we evaluated the influence of 7T T2w-TSE on STN target planning, the number of microelectrode recording (MER) trajectories, length of STN activity and the postoperative motor (UPDRS) improvement.2. For 25 PD patients 7T DWI was additionally obtained, enabling probabilistic segmentation3 of motor, associative and limbic STN sub-regions based on their probabilistic connectivity to the corresponding cerebral regions. Left- and right-sided motor outcome scores were used for evaluating the correspondence between the active electrode contacts and the clinical DBS effect4. The Bejjani lined was reviewed for crossing of segments.
3. Multi-unit activity (MUA) and single-unit activity (SUA) acquired during MER were compared between STN and (probabilistic segmented) motor-STN.
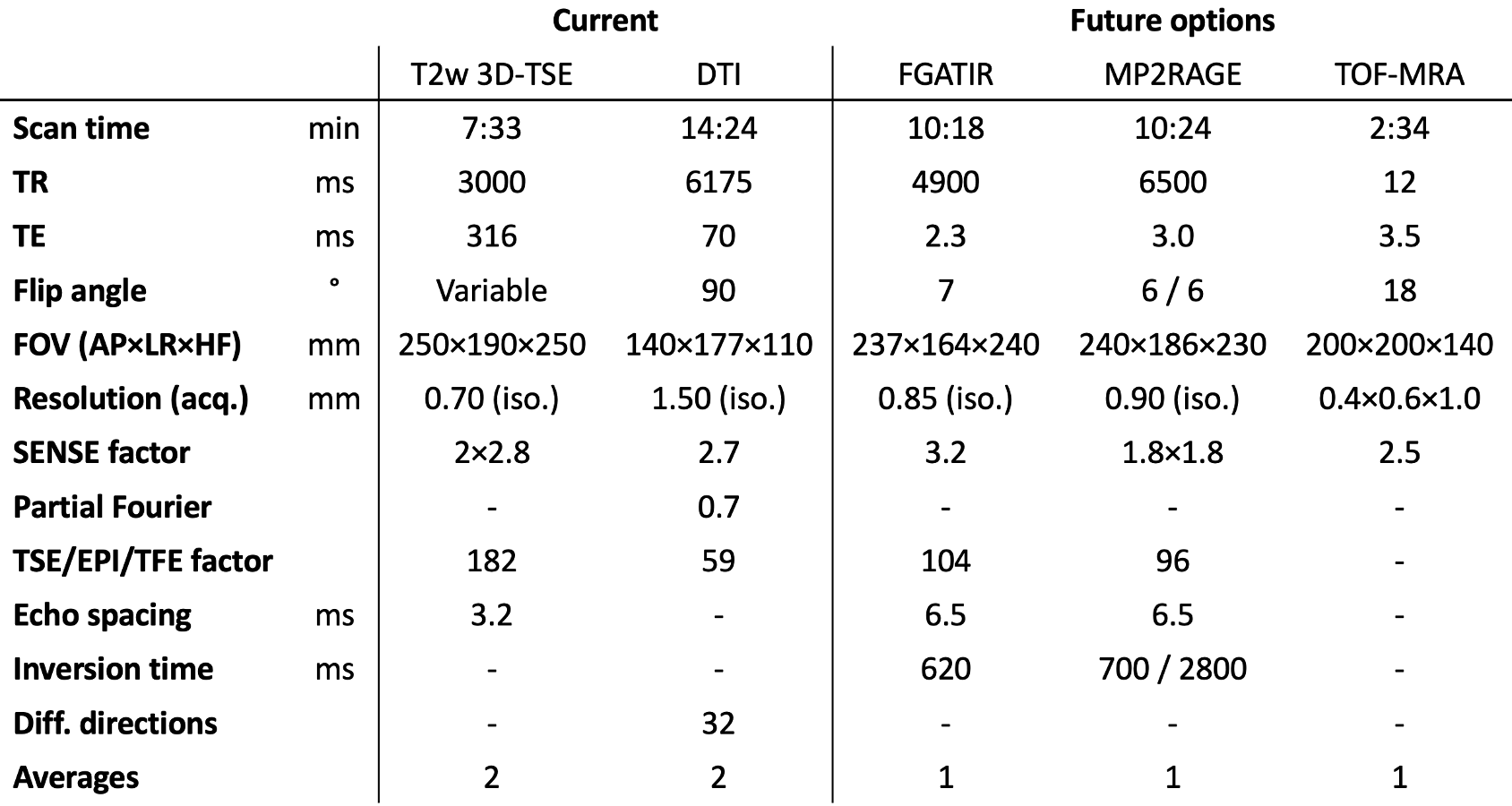
An overview of the acquisition parameters for each of the protocols can be found in Table 1.
Results
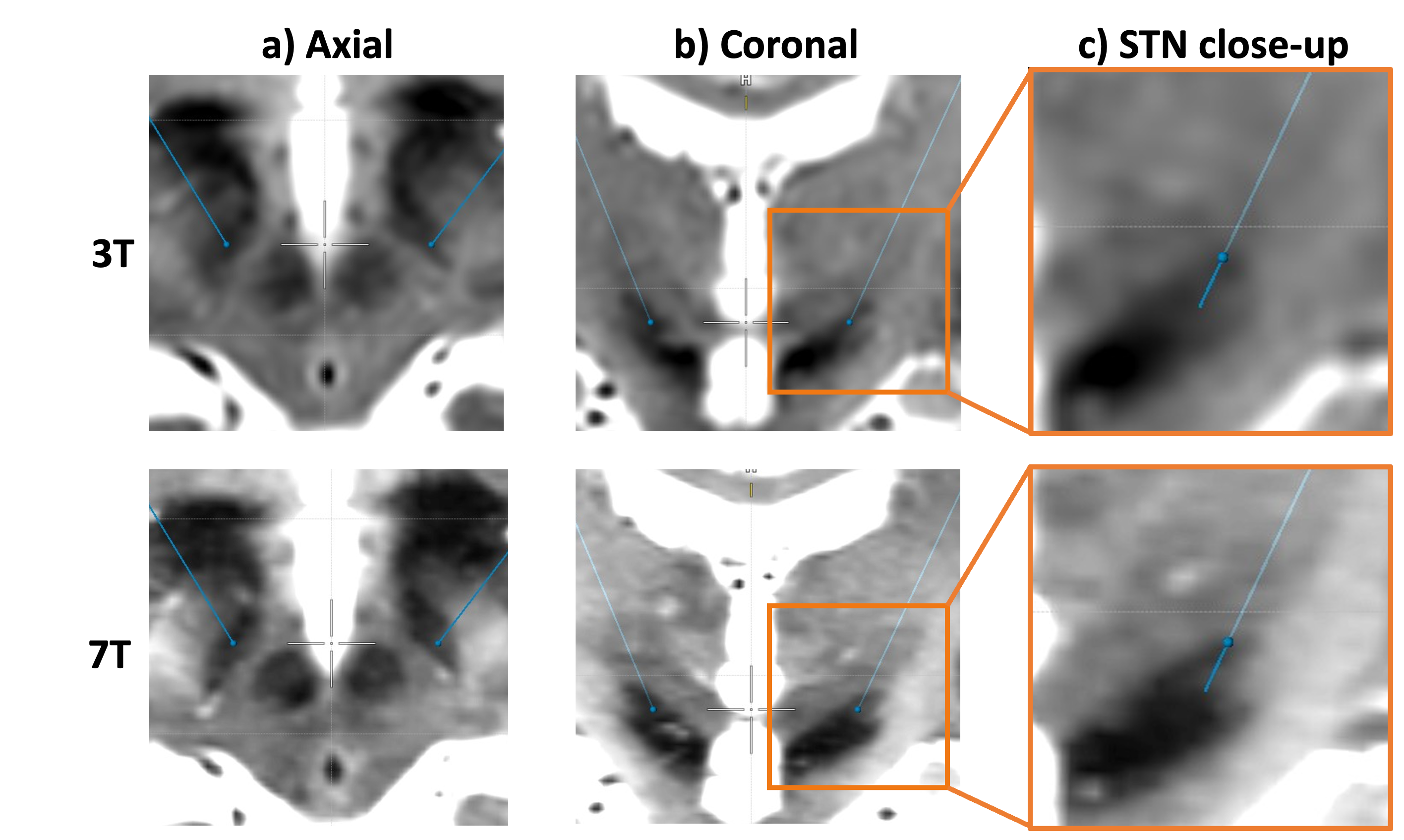
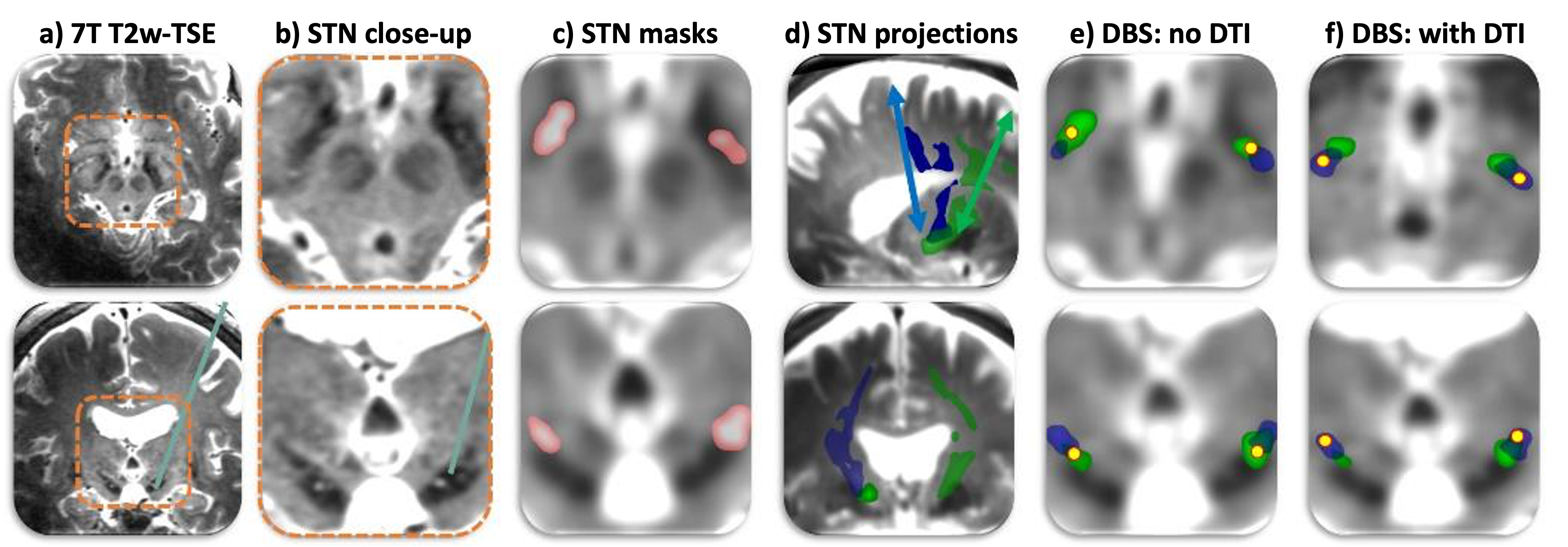
1. From February 2007 to January 2014, 1.5 and 3-Tesla T2w-TSE guided STN DBS with 3 simultaneous MER channels was performed in 76 PD patients. The central MER trajectory was chosen for implantation in 39%. Average length of recorded STN activity in the definite electrode trajectory was 3.9 ± 1.5 mm. From January 2015 to January 2022 7T T2w-TSE and MER-guided STN DBS was performed in 182 PD patients. The central trajectory was chosen for implantation in 81%, and the number of used MER channels decreased from 3 to 1. Average UPDRS improvement was comparable. Figure 1 shows an example of the STN visualization at 3T and at 7T.2. The probabilistic segmentation of 50 STNs proved highly feasible (see Figure 2). Although the highest density of motor connections was situated in the dorsolateral STN, exact partitioning of segments differed considerably. For all the active electrode contacts situated within the predominantly motor-connected segment of the STN, the average hemi-body UPDRS motor improvement was 80%; outside this segment 52% (p < 0.01). The Bejjani line was situated in the motor segment for 32 of the 50 STNs.
3. MUA was found slightly higher in the motor-STN versus the STN (p < 0.001, area under the ROC curve 0.63); the SUA did not differ between the groups.
Discussion and Conclusion
Implementation of 7T T2w-TSE for STN DBS enabled a refinement in targeting. Combining classical DBS targeting with dorsolateral STN alignment may be used to determine the optimal trajectory. STN segmentation offers insight into location of the (dorsolateral) motor subdivision. The 7T connectivity-derived motor-STN corresponded well with DBS-outcome, however, MER did not accurately distinguish this subdivision from the remaining STN. Segmentation-guided electrode placement is likely to further improve motor response in DBS for PD, and is part of a pilot study in our centre. We are currently evaluating additional 7T sequences for possible implementation in DBS; 3D time-of-flight MR angiography for vessel depiction and FGATIR5 for visualizing thalamus/globus pallidus (see Table 1 for sequence parameters). Synthetic MP2RAGE-derived FGATIR data is also considered as a scan time-efficient and inhomogeneity-robust solution for conventional FGATIR6.To date, we rarely encountered non-compatible implants. All patients undergo safety screening with a questionnaire and magnetometer, and patient compliance was found to be very high with few reported side-effects. We are convinced that 7T MRI in DBS will enable a safe, impactful and long-term line of clinical application and research. However, the implementation of 7T in routine DBS practise can be challenging and requires close collaboration between neuroscientists, MR-physicist and clinicians.
Acknowledgements
No acknowledgement found.References
1. Lozano AM, Lipsman N, Bergman H, et al. Deep brain stimulation: current challenges and future directions. Nat Rev Neurol 2019;15:148–160 doi: 10.1038/s41582-018-0128-2.
2. Koirala N, Serrano L, Paschen S, et al. Mapping of subthalamic nucleus using microelectrode recordings during deep brain stimulation. Sci Rep 2020;10 doi: 10.1038/s41598-020-74196-5.
3. Behrens T, Johansen-Berg H, Woolrich M, et al. Non-invasive mapping of connections between human thalamus and cortex using diffusion imaging. Nat Neurosci 2003;6:333–339 doi: 10.1038/nn1075.
4. Mathiopoulou V, Rijks N, Caan MWA, et al. Utilizing 7-Tesla Subthalamic Nucleus Connectivity in Deep Brain Stimulation for Parkinson Disease. Neuromodulation 2023;26:333–339 doi: 10.1016/j.neurom.2022.01.003.
5. Sudhyadhom A, Haq IU, Foote KD, Okun MS, Bova FJ. A high resolution and high contrast MRI for differentiation of subcortical structures for DBS targeting: The Fast Gray Matter Acquisition T1 Inversion Recovery (FGATIR). Neuroimage 2009;47 doi: 10.1016/j.neuroimage.2009.04.018.
6. Tao S, Zhou X, Lin C, Patel V, Westerhold EM, Middlebrooks EH. Optimization of MP2RAGE T1 mapping with radial view-ordering for deep brain stimulation targeting at 7 T MRI. Magn Reson Imaging 2023;100:55–63 doi: 10.1016/j.mri.2023.03.007.
Figures