4188
Investigating the Impact of Subthalamic Nucleus DBS Frequency on Motor Networks in Parkinson's Disease: An fMRI Study1Cleveland Clinic, Cleveland, OH, United States, 2Milwaukee School of Engineering, Milwaukee, WI, United States
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease
Motivation: Limited information is available on the impact of different deep brain stimulation (DBS) frequencies on motor task-related brain activity in Parkinson's disease (PD) patients with DBS implants in the subthalamic nucleus (STN).
Goal(s): To investigate DBS frequency effects on brain activity during a motor task (force-tracking, FT).
Approach: Using fMRI, we assessed FT-task-related brain activity in four PD patients with STN-DBS under three DBS conditions: off, high-frequency, and low-frequency. MDS-UPDRS-III scores measured motor impairment.
Results: High-frequency DBS increased brain activation during FT and reduced MDS-UPDRS-III scores in PD patients compared to low-frequency DBS and DBS-off.
Impact: These findings suggest that DBS in the STN has the potential to disrupt abnormal neural activations and restore the brain's capacity to generate and regulate normal patterns that are compromised in PD.
Introduction
Parkinson's disease (PD) is a progressive neurodegenerative disorder characterized by motor symptoms such as tremor, rigidity, and bradykinesia. Deep brain stimulation (DBS) has emerged as a promising therapeutic approach for managing these symptoms, particularly when targeting the subthalamic nucleus (STN) 1. However, the specific effects of DBS, especially at different stimulation frequencies, on the brain networks underlying motor control remain a subject of ongoing research. Functional Magnetic Resonance Imaging (fMRI) allows for the exploration of how the brain responds to varying stimulation frequencies 2, 3. This study aimed to shed light on the impact of STN-DBS at varying frequencies on brain activation patterns during a motor task, specifically a force-tracking (FT) task using fMRI, and its therapeutic implications for PD patients.Methods
This study involved the participation of four patients who had been diagnosed with PD and had undergone bilateral STN-DBS (Medtronic Sensight™ B33005 leads connected to Percept PC IPG). Informed consent was obtained for each patient. The demographics, clinical, and DBS parameters of these 4 patients are shown in Figure 1. We collected fMRI data using a 3T Siemens scanner equipped with a T/R head coil. The fMRI data was obtained through an EPI sequence with the following parameters: repetition time/echo time = 2800/2.9 ms, a flip angle of 80o, a slice thickness of 4 mm, and a matrix size of 64x64. We implemented a standard fMRI block-design paradigm, wherein FT periods were alternated with periods of rest. During the FT periods, patients continuously pinched a force transducer between their dominant (right) thumb and index finger to follow a sinusoidal wave. The target sine wave has a range equivalent to 10%–30% of the patient’s maximum pinch grip force. To evaluate the performance of the FT task, we calculated the relative root mean square error (RRMSE) between the target force and the measured output (grip) force over time. RRMSE values close to zero indicate highly accurate grip force control 4. In contrast, during the rest periods, patients were directed to keep their hands at rest. Each cycle of FT and rest lasted 33.6 seconds, and in total, the task had 11.5 cycles (i.e., 12 FT periods, and 11 rest periods), resulting in a total duration of 386.4 seconds. fMRI scans were collected under three different STN-DBS conditions: DBS turned off, DBS turned on at the high (optimal) frequency, and DBS turned on at a lower (40 Hz) frequency. It's worth noting that during the DBS "on" conditions (high and low frequencies), when patients used their right hand for the task, we activated the left DBS while deactivating the right stimulation. This choice was made to observe the effects of the left DBS on the performance of the right-hand task without any influence from the right DBS. Subsequently, fixed-effect fMRI analyses were performed using Statistical Parametric Mapping 12 toolbox in MATLAB R2021a. A false discovery rate correction with P < 0.05 was used to identify brain regions that were activated during the FT task. Additionally, we evaluated the severity of motor symptoms in these patients using the MDS-UPDRS-III scales for the same three DBS conditions. A higher score on the MDS-UPDRS-III indicates a greater impairment in motor functioning.Results
The mean ± standard deviation of RRMSE during FT for DBS-off, low-frequency DBS, and high-frequency DBS were 1.66 ± 0.30, 1.21 ± 0.31, and 1.10 ± 0.17, respectively. Figure 2 illustrates the mean RRMSE across 12 different FT periods. Group-level fMRI analysis revealed increased activation in various brain regions, including the bilateral motor, somatosensory, supplementary motor areas, parietal, occipital, basal ganglia, thalamus, and cerebellum during the FT-periods when patients had high-frequency DBS, compared to both low-frequency DBS and the DBS-off condition (see Figure 3). Additionally, the assessment of motor symptoms using the MDS-UPDRS-III scale indicated a significant reduction during high-frequency DBS, in contrast to both low-frequency DBS and the DBS-off state (refer to Figure 4).Discussion
The increased brain activation coupled with improved motor scores indicates that high-frequency DBS likely exerts its effects by modulating and enhancing the functioning of motor networks in the brain and basal ganglia-thalamocortical circuits. In contrast, low-frequency DBS does not seem to yield the same level of benefit, underscoring the frequency-dependent nature of these effects.Conclusion
High-frequency DBS enhances neural recruitment and processing for motor control when compared to low-frequency stimulation or DBS off, emphasizing its potential as an effective therapeutic intervention. However, further validation in a larger sample is warranted to confirm and generalize these findings.Acknowledgements
No acknowledgement found.References
1. Groiss SJ, Wojtecki L, Sudmeyer M, Schnitzler A. Deep brain stimulation in Parkinson's disease. Ther Adv Neurol Disord 2009;2(6):20-28.
2. DiMarzio M, Madhavan R, Hancu I, et al. Use of Functional MRI to Assess Effects of Deep Brain Stimulation Frequency Changes on Brain Activation in Parkinson Disease. Neurosurgery 2021;88(2):356-365.
3. Shen L, Jiang C, Hubbard CS, et al. Subthalamic Nucleus Deep Brain Stimulation Modulates 2 Distinct Neurocircuits. Ann Neurol 2020;88(6):1178-1193.
4. Confalonieri L, Pagnoni G, Barsalou LW, Rajendra J, Eickhoff SB, Butler AJ. Brain Activation in Primary Motor and Somatosensory Cortices during Motor Imagery Correlates with Motor Imagery Ability in Stroke Patients. ISRN Neurol 2012;2012:613595.Figures
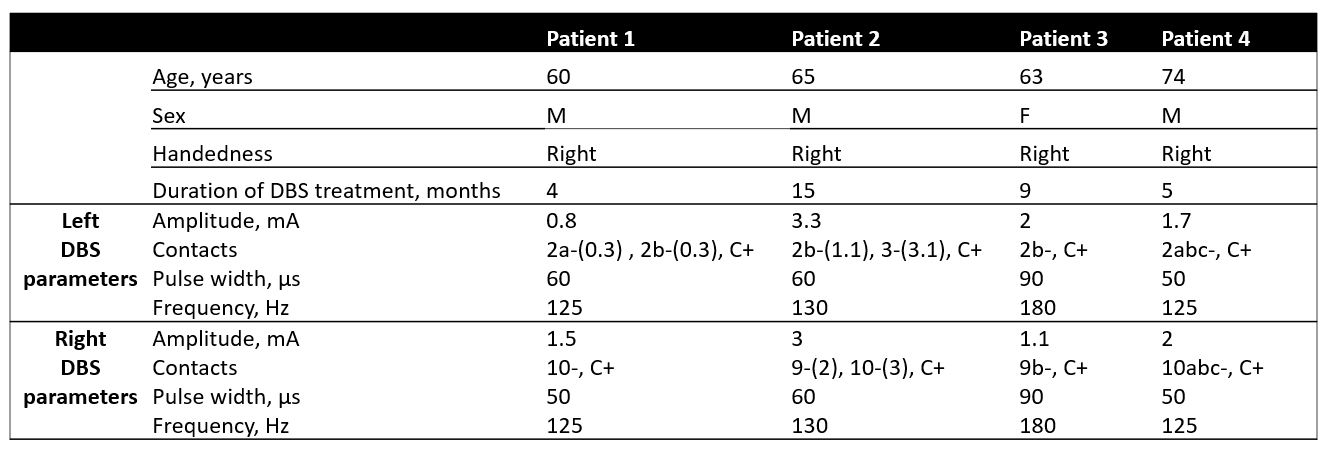
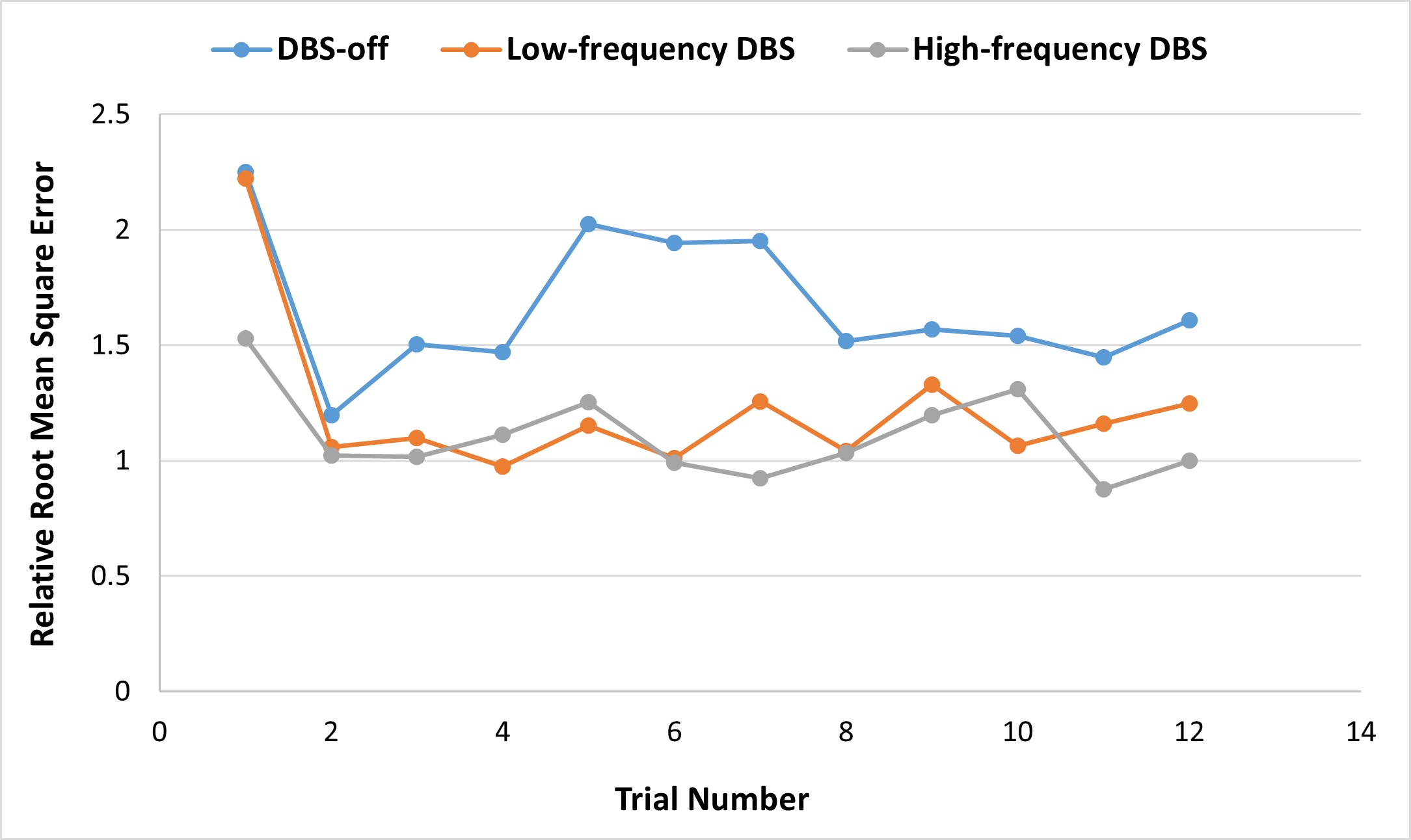
Figure 2. The mean Relative Root Mean Square Error (RRMSE) across 12 different force-tracking periods. The force-tracking periods are represented along the x-axis by trial number. The y-axis shows the average RRMSE value for each period. Lower RRMSE values indicate less error between the measured and target forces.
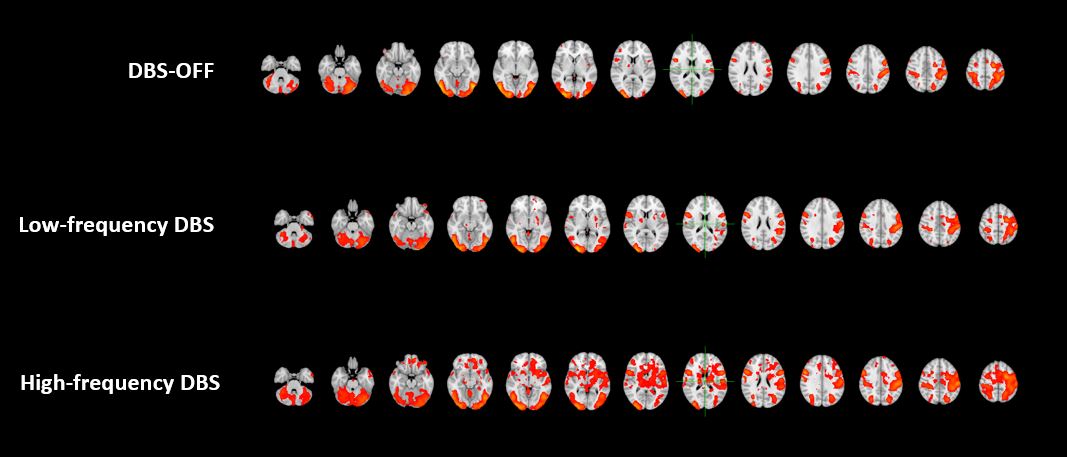
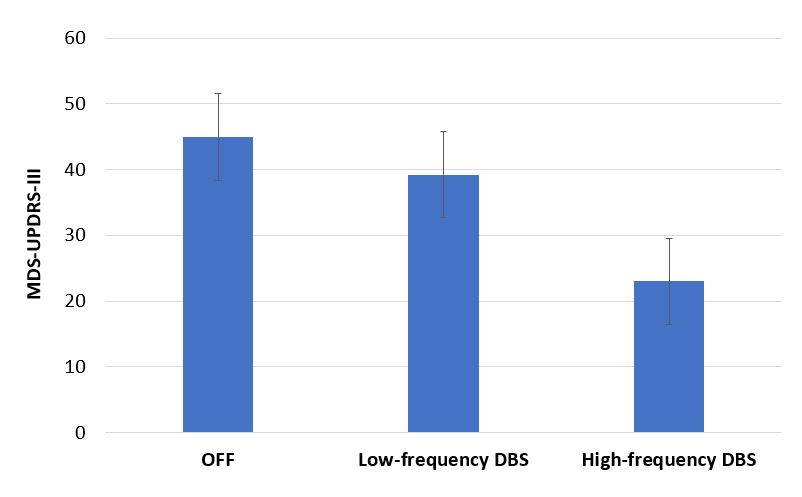
Figure 4. Bar graph displaying the mean UPDRS III scores of PD patients with STN-DBS under various DBS conditions: off, low-frequency DBS, and high-frequency DBS