4186
Alterations in Static and Dynamic Functional Brain Connectivity in Drug-naïve Patients with Early Parkinson’s Disease1Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Synopsis
Keywords: Parkinson's Disease, fMRI (resting state), Brain
Motivation: Long-term levodopa treatment can markedly change the brain connectivity network in Parkinson's disease(PD) patients. The changes of static and dynamic brain network in early PD remain unknown.
Goal(s): To investigate the alterations in static and dynamic whole-brain connectivity in early PD patients who have never received dopaminergic therapy.
Approach: A case-control study was performed. The static and dynamic functional connectivity were constructed and analysised.
Results: PD patients showed alterations in the SMN, DGN, LBN, and VSN, which may be relevant to both motor and non-motor symptoms. LEiDA results showed that PD group displayed a shorter lifetime and lower probability than the HC group.
Impact: The study offers neuroimaging evidence of static and dynamic brain functional connectivity changes in drug-naïve early Parkinson's disease patients. It identifies potential biomarkers for clinical Parkinson’s disease diagnosis and assessment.
Introduction
Parkinson’s disease pathology—characterized by the deposition of α-synuclein and formation of Lewy bodies—has confirmed that brain lesions are silently activated prior to the onset of clinical symptoms1. PD has been proposed to be a disconnection syndrome owing to its widely affected brain regions and complicated clinical symptoms2. However, current research on resting-state fMRI for PD mainly focuses on patients with advanced PD and explores the association between specific symptoms, such as motor symptoms or cognitive impairment, and brain connectivity in specific regions; the changes in static and dynamic brain connectivity in early PD remain unknown. The aim of our study was to explore the static and dynamic functional connectivity alterations in the brain in drug-naïve patients with early PD.Methods
A case-control study of 65 PD patients and 80 HC participants were collected. All participants were underwent rs-fMRI and a series of questionnaires such as UPDRS-III, MMSE, MOCA, HAMA and HAMD to assess the severity of disease and the status of psychiatry.Functional images were preprocessed using the Data Processing and Analysis for Brain Imaging(DPABI) software toolbox. Preprocessing steps included slice-timing correction, motion correction, spatial normalization, linear detrending, regressing out nuisance covariates (six head-motion parameters, cerebrospinal fluid, and white matter signals), low-pass filtering with a frequency cut-off of 0.01–0.08 Hz, and smoothing by Gaussian kernel.
The mean time series of 90 cortical or subcortical regions based on anatomical automatic labeling atlas was extracted. The static functional brain connectivity (SFBC) was constructed by Pearson’s correlation. The intra- and internetwork architecture of SFBC were analysed at integrity level, network level and edge level by 8 well-defined functionally brain networks3. The dynamic functional connectome (DFBC) was defined by clustering the BOLD phase-locking patterns obtained using leading eigenvector dynamics analysis (LEiDA) and characterized from a dynamic perspective by the occupancy, lifetime, and transition profiles of DFC patterns4-5. The score of UPDRS-III, MMSE, MOCA, HAMA and HAMD reflecting the motor and non-motor symptoms of PD were collected for further regression analysis with SFC and DFC parameters.
Results
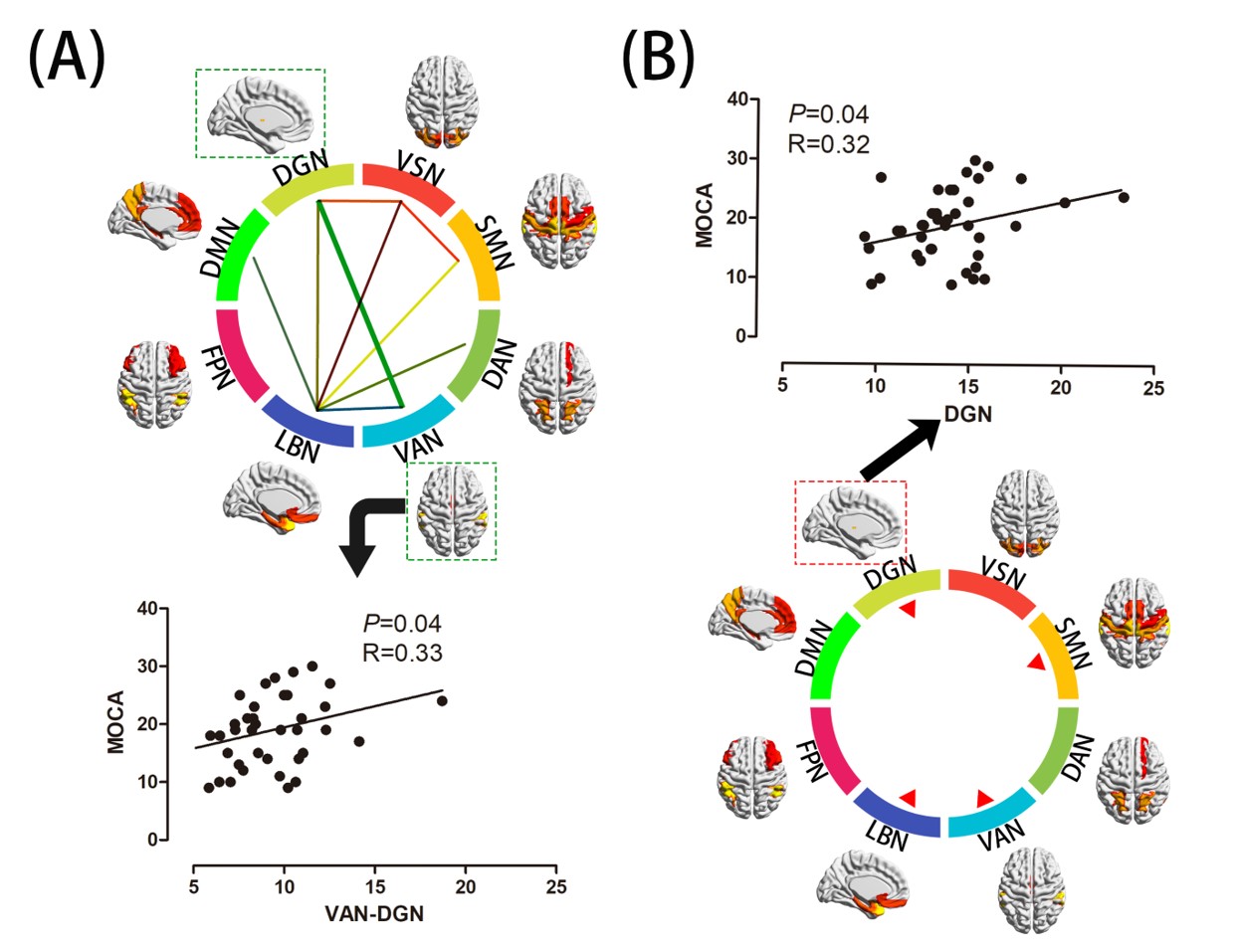
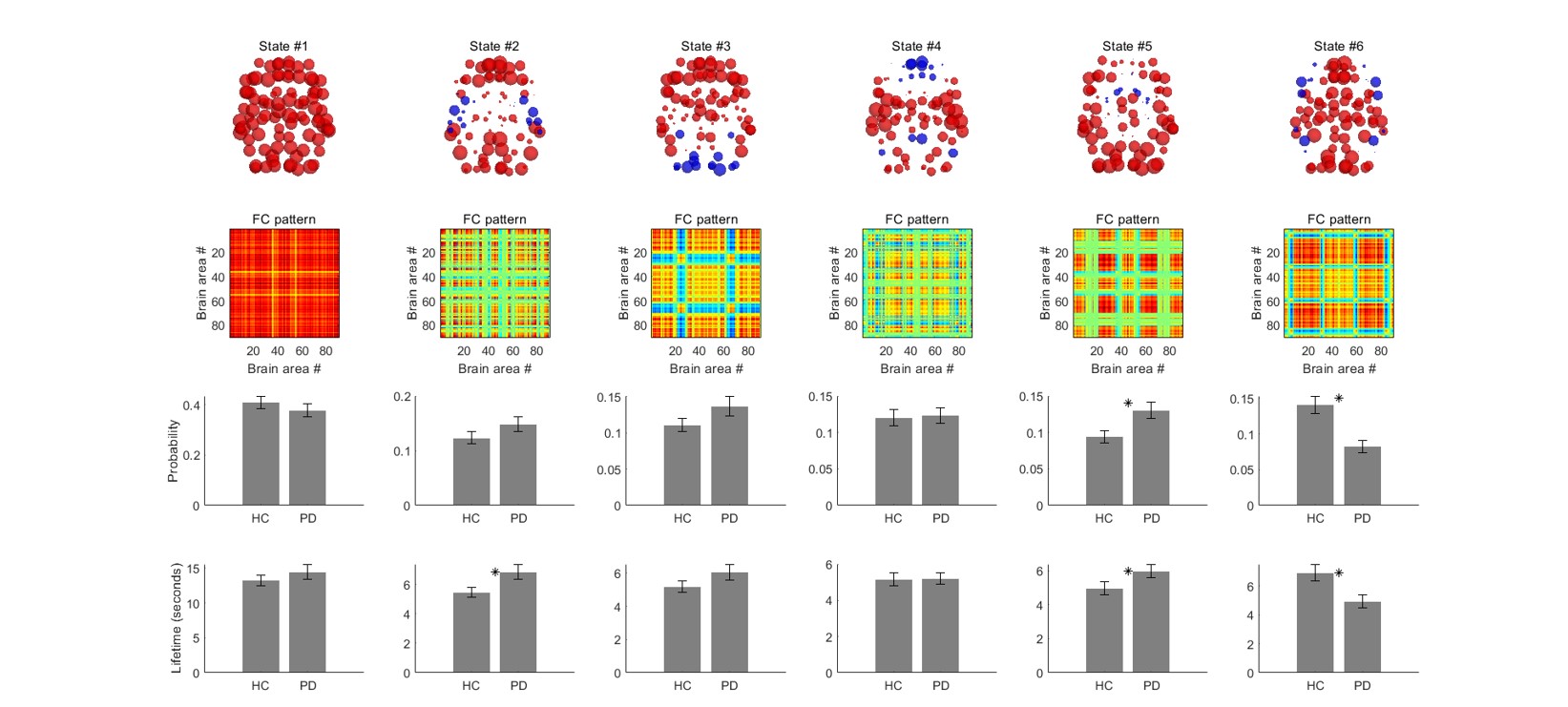
For SFC analysis, reduced degree of functional connectivity were mainly observed in the visual (VSN), somatomotor (SMN), limbic (LBN), and deep gray matter networks (DGN) at integrity level in PD patients. Intra-network analysis indicated decreased functional connectivity in DGN, SMN, LBN, and ventral attention networks (VAN). Inter-network analysis indicated reduced functional connectivity in nine pairs of resting-state networks. At the edge level, the LBN was the center of abnormal functional connectivity (p < 0.05, FDR corrected) (Fig 1).For DFBC analysis, LEiDA results showed that PD group displayed a shorter lifetime (p < 0.05, FDR corrected) and lower probability (P<0.05, FDR corrected) than the HC group in a characteristic of DFC mainly involving the DGN and SMN (Fig 2).
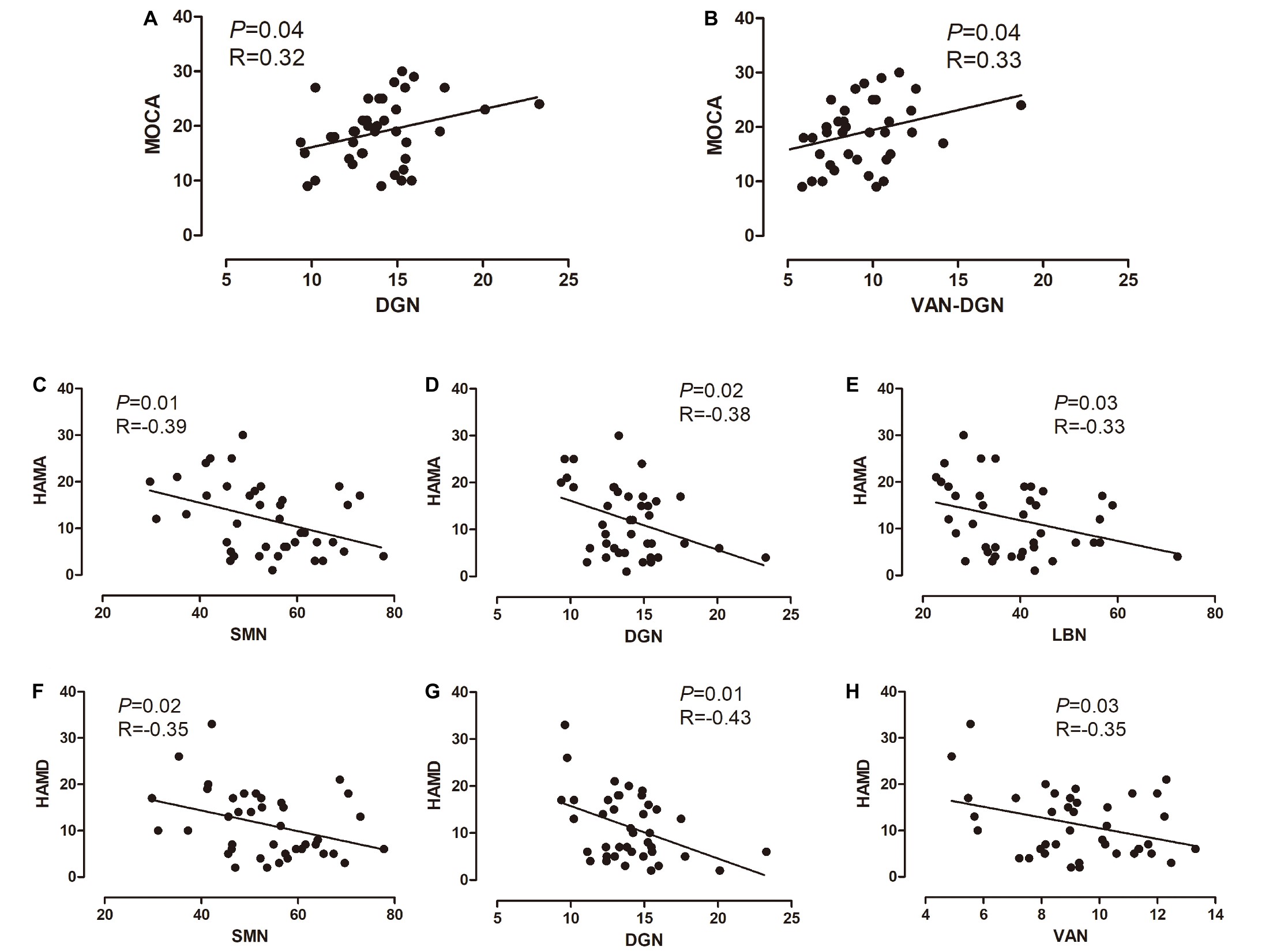
For regression analysis of SFBC parameters, MOCA score was associated with the intra-network functional connectivity strength of the DGN, and inter-network FC of the DGN-VAN. HAMA and HAMD scores were associated with the functional connectivity strength of the SMN and DGN, and either the LBN or VAN, respectively. For regression analysis of DFBC parameters, the lower probability in the PD group was found to be negatively correlated with the HAMA and MOCA in a partial correlation analysis with years of education as a covariate (Fig 3).
Discussion
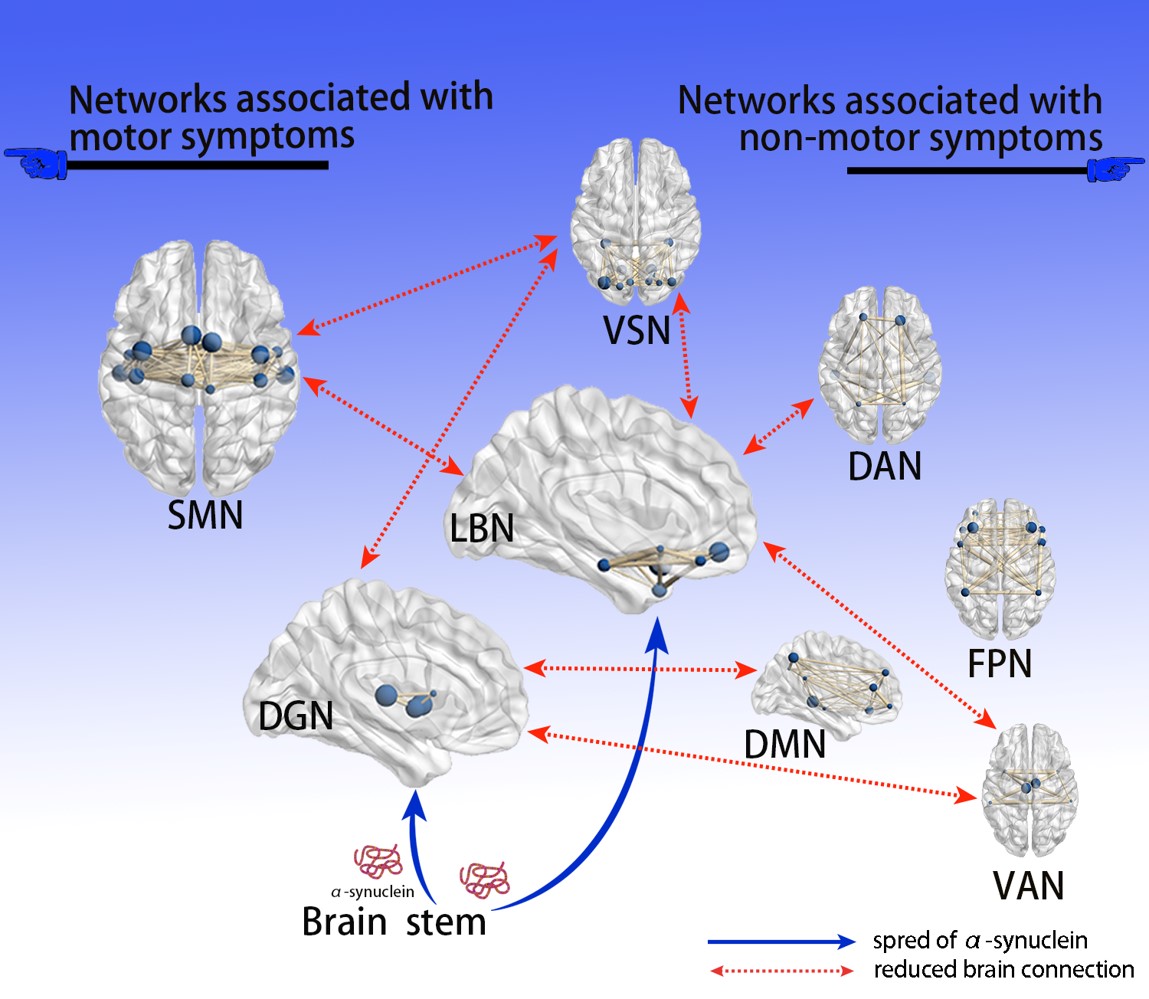
In our study, the brain was divided into 90 regions and eight networks, while the SFBC and DFBC of the two groups were analyzed at three different levels. We identified the first brain connectionsto be affected in the early stages of PD, providing a basis for our understanding of disease occurrence and development. Our results further supported the view that PD is a disconnection syndrome2: functional disconnection among brain regions resulted in a series of clinical manifestations.Based on Braak’s PD hypothesis6 and our findings, we proposed a hypothetical model to explain how the deposition of α-synuclein affects brain networks (Figure 4).Conclusion
Our study demonstrated the variation of whole brain static and dynamic functional connectivity in drug-naïve patients with early PD compared with age-matched HC. The main changes of SFBC and DFBC focus on SMN, DGN and LBN, which may be relevant to the motor and non-motor symptoms in early PD. Meanwhile, our results indicate that a holistic understanding of brain function can only be gleaned if the temporal dynamics of functional connectivity is included.Acknowledgements
We thank all participants for their help and support in our study.References
1, Schapira, A. H. V., Chaudhuri, K. R., and Jenner, P. (2017). Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 18, 435–450. doi:10.1038/nrn.2017.62.
2, Cronin-Golomb, A. (2010). Parkinson’s disease as a disconnection syndrome. Neuropsychol. Rev. 20, 191–208. doi:10.1007/s11065-010-9128-8.
3, Zhai, H., et al., Convergent and divergent intra- and internetwork connectivity in Parkinson's disease with wearing-off. Neurol Sci, 2023. doi:10.1007/s10072-023-07005-2.
4,Kringelbach, M.L. and G. Deco, Brain States and Transitions: Insights from Computational Neuroscience. Cell Rep, 2020. 32(10): p. 108128. doi:10.1016/j.celrep.2020.108128
5,Magalhaes, R., et al., Habitual coffee drinkers display a distinct pattern of brain functional connectivity. Mol Psychiatry, 2021. 26(11): p. 6589-6598. doi:10.1038/s41380-021-01075-4.
6, Braak, H., Ghebremedhin, E., Rüb, U., Bratzke, H., and Del Tredici, K. (2004). Stages in the development of Parkinson’s disease-related pathology. Cell Tissue Res. 318, 121–134. doi:10.1007/s00441-004-0956-9.
Figures