4185
Exploring the discrepancy of hippocampal subfield vulnerability and connectivity pattern between cognitive decline in PD and MCI patients1Radiology, Huashan Hospital, Fudan University, Shanghai, China, 2GE Healthcare, Beijing, China
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease
Motivation: Different vulnerabilities of hippocampal subfields in PD and MCI have been reported.
Goal(s): To explore the discrepancy of hippocampal subfield atrophy and its FC pattern in HC, PDNCI, PDMCI, and MCI patients.
Approach: Volume of hippocampal subfields, and FC between impaired subfields and cortical regions were calculated to assess group differences.
Results: PD groups had reduced volumes in CA2/3, CA4, and GC-DG subfields and increased FC in the visual network.MCI group exhibited decreased right CA4 volume and increased FC in the widespread visual network.PDMCI displayed enhanced FC in the DMN compared to PDNCI and decreased FC in the visual network relative to MCI.
Impact: As cognitive decline advances in PD, FC alterations are prominent between the GC-DG+CA4 subfield and the DMN. Smaller hippocampal subfield and its widespread FC abnormalities in MCI relative to PDMCI may underscore the different progression mechanisms of the two diseases.
Introduction
Parkinson's disease (PD) is the second most common neurodegenerative disorder after Alzheimer’s disease (AD), which manifests with many motor and non-motor symptoms1. Cognitive impairment (CI) is one of the most clinically prominent non-motor symptoms in PD2. Mild cognitive impairment (MCI) and PD with MCI (PDMCI) are respectively transitional periods in the AD and PD continuum, with a high risk of progression to dementia3-4. The hippocampus is the most widely studied target in MCI. Also, there is a general agreement that hippocampal atrophy is associated with CI in PD in recent years. Moreover, AD pathology in patients with PD may go on to develop more advanced CI5. However, different vulnerabilities of hippocampal subfields in PD and MCI have been reported. Exploring the differential role of the hippocampal subfields could help to understand the progression mechanisms of CI in the two diseases. Despite no clear consensuses on atrophy patterns, recent advancements applying structural MRI showed specific hippocampal subfields were impaired in PD and MCI patients3,6-10. Previous evidence found the GC-DG, CA4, CA2/3, CA1, subiculum, and presubiculum associated with CI in PD7-9. Several studies reported that the CA1 and subiculum are the most central subfields in the progression of MCI10, other studies suggested that the GC-DG and fimbria are sensitive in detecting MCI3. Besides, what section of the hippocampus is connected with other important cerebral regions and involved in CI progression in PD and MCI is barely investigated. Therefore, we aimed to explore the shared and distinct alteration of hippocampal subfields atrophy and its functional connectivity (FC) pattern between PD with cognitive decline and MCI patients.Materials and Methods
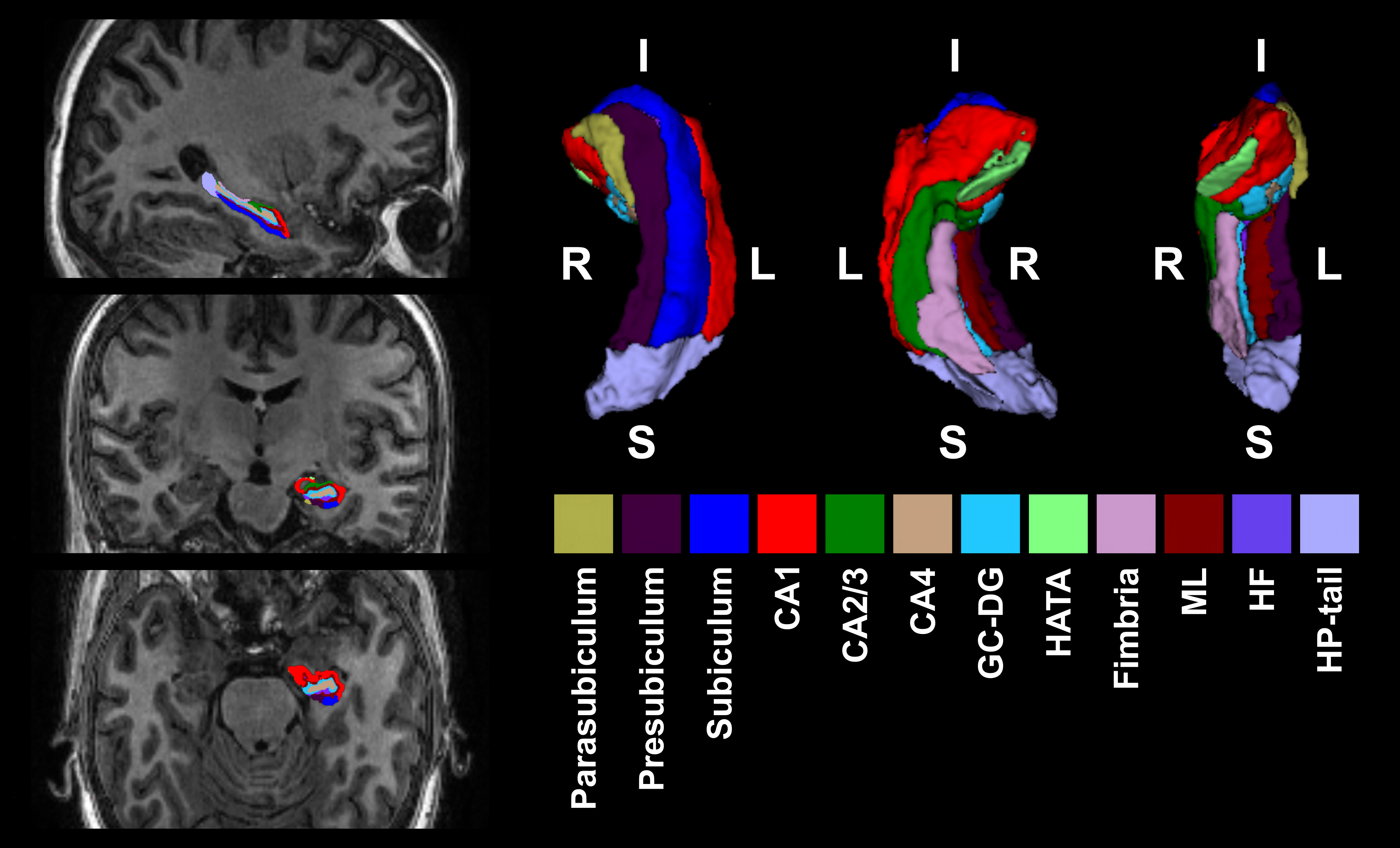
116 PD patients and 178 controls were retrospectively collected from two clinical centers. All patients with PD met the MDS clinical diagnostic criteria. Based on Movement Disorders Society Task Force criteria, four diagnostic groups, PDNCI, PDMCI, MCI, and HC groups were classified. MRI examinations were performed on two 3.0-T MRI scanners (Discovery MR750, GE Healthcare, Milwaukee, WI; Magnetom Verio, Siemens, Erlangen, Germany). 3D T1WI and rs-fMRI images were obtained. Structural image and Rs-fMRI data were preprocessed with FreeSurfer and SPM8 as previously11-12. The Bayesian inference method was used to divide 13 hippocampal subfields (Figure 1). FC analysis was performed between each hippocampal subfields ROI and the whole brain mask in a voxel-wise manner using DPABI. Statistical analyses were performed using SPSS. To compare the hippocampal subfield volume among four groups, MANCOVA followed by post-hoc tests were performed. To explore FC differences among four groups, a voxel-wise one-way ANCOVA was performed. Subsequently, we used post-hoc t-contrasts to analyze between-group differences.Results
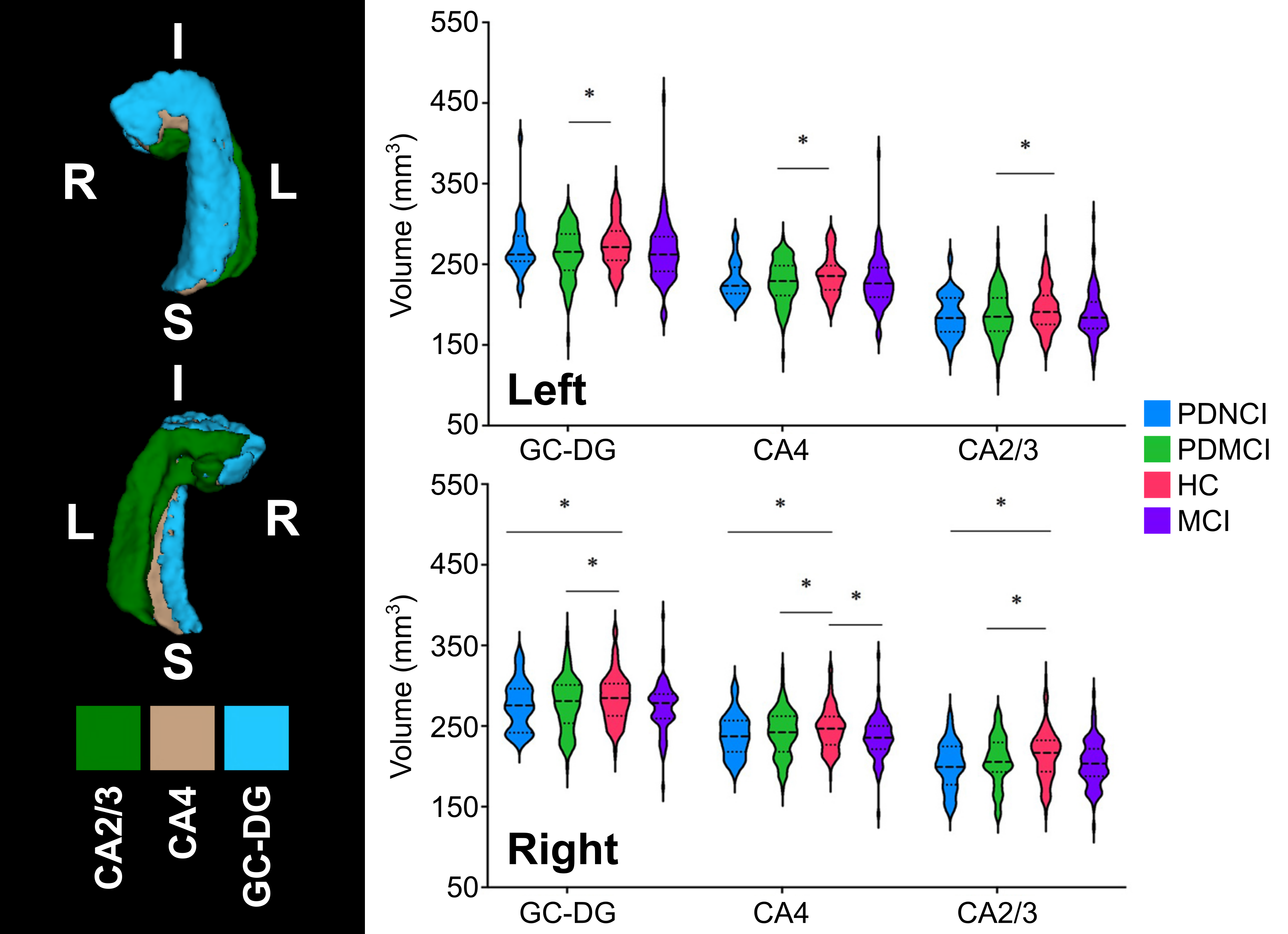
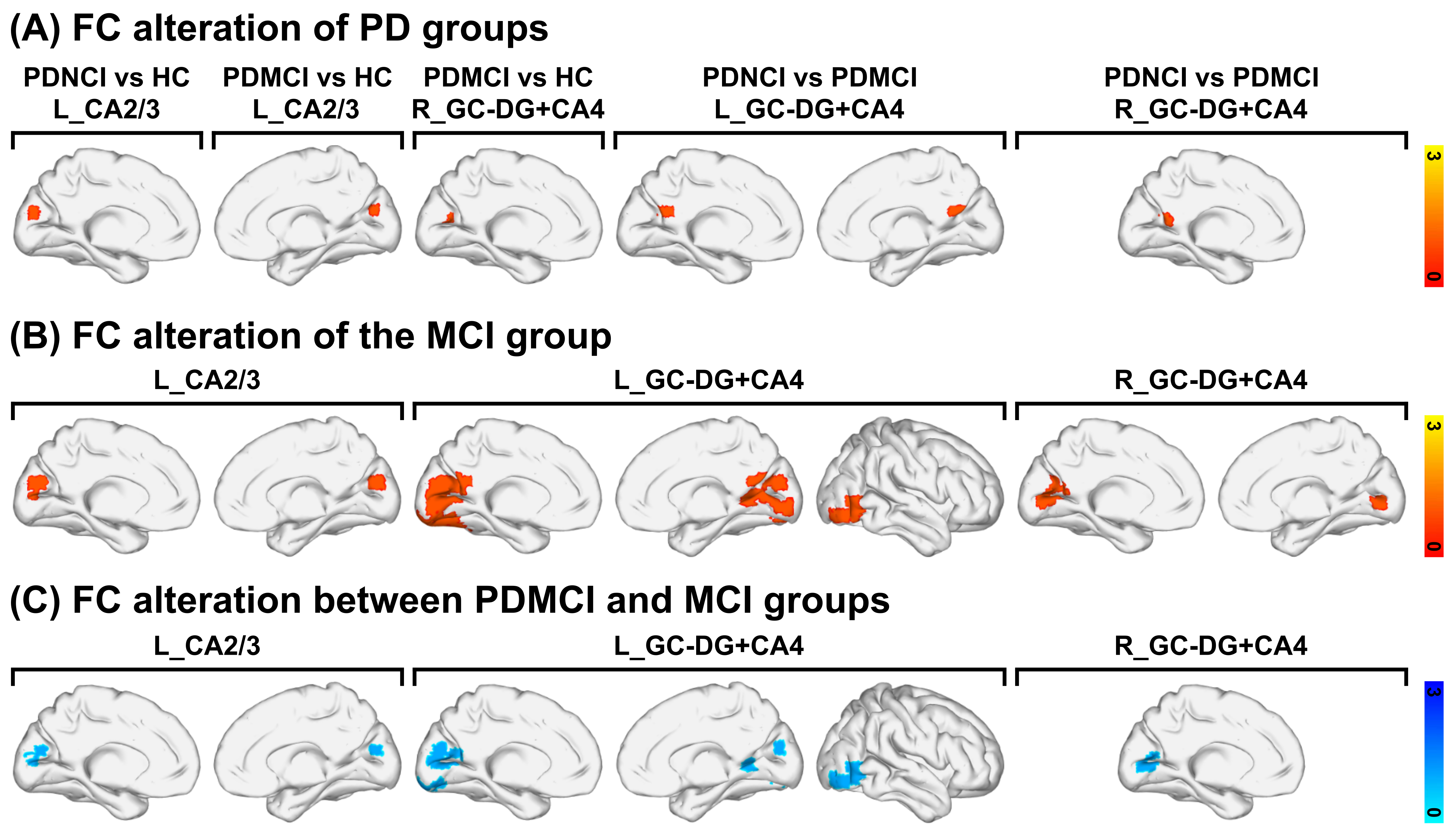
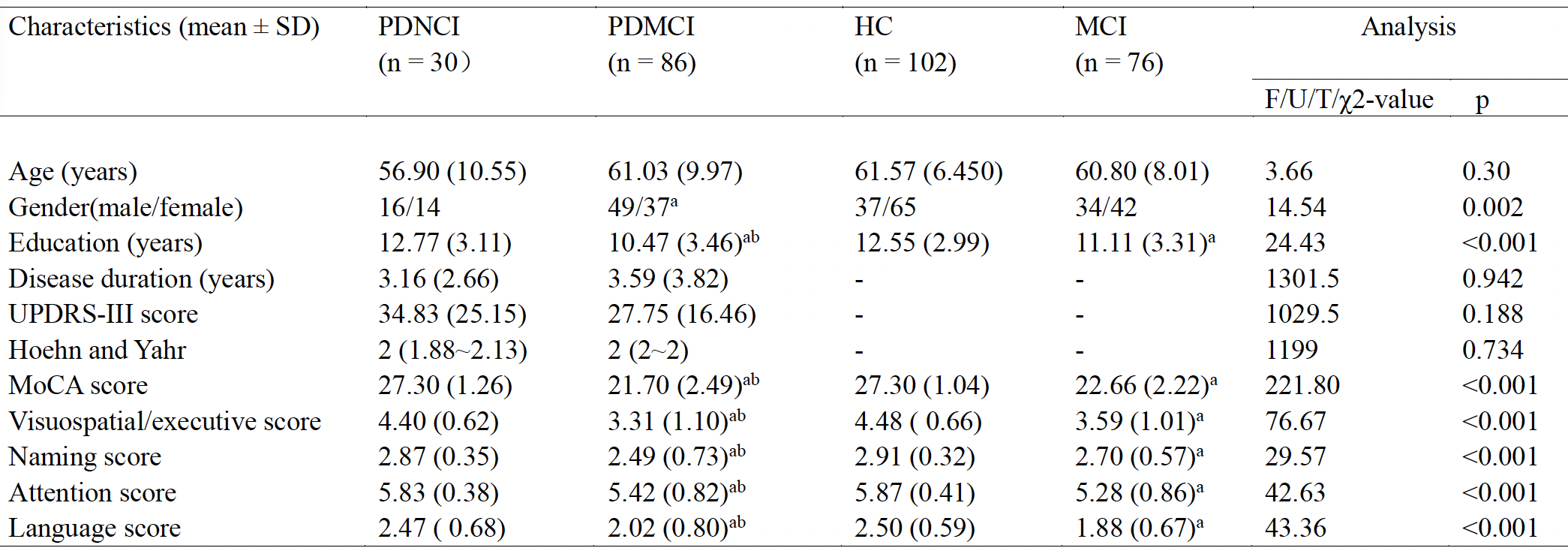
Table 1 displays clinical characteristics comparison results. Significant differences were found in gender, education, MoCA as well as each of six cognitive domains, and TIV. PDNCI group showed volumetric reduction of right CA2/3, CA4, and GC-DC subfields compared to HC group (Figure 2). Volumetric reductions of bilateral CA2/3, CA4, and GC-DC subfields were found in PDMCI relative to HC group. We also observed significantly decreased volume of right CA4 subfield in MCI as compared to HC group. Compared with HC group, the PDNCI group showed increased FC between the left CA2/3 subfield and visual network (Figure 3A). The PDMCI group showed increased FC between left CA2/3 subfield and visual network, as well as increased FC between right GC-DG+CA4 subfield and visual network. Relatively to PDNCI group, significantly increased FC between left GC-DG+CA4 subfield and DMN was reported in the PDMCI group, as well as increased FC between right GC-DG+CA4 subfield and visual network, and DMN. Compared with HC group, MCI group showed increased FC between left CA2/3 subfield and visual network (Figure 3B). There was significantly increased FC between left GC-DG+CA4 subfield and visual network, and DMN in MCI group. Additionally, MCI group showed increased FC between right GC-DG+CA4 subfield and visual network. Compared with MCI group, decreased FC between left CA2/3 subfield and visual network was observed in PDMCI group (Figure 3C). There was significant FC reduction between left GC-DG+CA4 subfield and visual network in PDMCI. We also observed significantly decreased FC between right GC-DG+CA4 subfield and visual network in the PDMCI.Discussion
Cognitive impairment in PD is associated with severe structural vulnerability of hippocampal subfields in the mossy fiber pathway, leading to altered FC with visual networks and DMN. As cognitive decline advances, FC alterations are prominent between the bilateral GC-DG+CA4 subfield and the DMN. Smaller hippocampal subfields atrophy and widespread FC abnormalities with the visual network in MCI relative to the PDMCI may provide evidence for different progression mechanisms between the two diseases.Acknowledgements
This research was supported by the National Natural Science Foundation of China (No. 82102016 and No. 82102132 ). We also thank all the participants in this study.References
1. Lafontaine A, Mellah S, Belleville S, Monchi O. rate of cortical thinning in patients with Parkinson ’ s disease longitudinally. 2014;1120–9.
2. Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins P V., et al. Current concepts in mild cognitive impairment. Arch Neurol. 2001;58:1985–92.
3. Xu H, Liu Y, Wang L, Zeng X, Xu Y, Wang Z. Role of hippocampal subfields in neurodegenerative disease progression analyzed with a multi-scale attention-based network. NeuroImage Clin [Internet]. Elsevier Inc.; 2023;38:103370.
4. Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sørensen P. Prevalence and characteristics of dementia in Parkinson disease: An 8-year prospective study. Arch Neurol. 2003;60:387–92.
5. Adamowicz DH, Roy S, Salmon DP, Galasko DR, Hansen LA, Masliah E, et al. Hippocampal β-synuclein in dementia with lewy bodies contributes to memory impairment and is consistent with spread of pathology. J Neurosci. 2017;37:1675–84.
6. Zhang J, Xie L, Cheng C, Liu Y, Zhang X, Wang H, et al. Hippocampal subfield volumes in mild cognitive impairment and alzheimer’s disease: a systematic review and meta-analysis. Brain Imaging Behav. 2023.
7. Low A, Foo H, Yong TT, Tan LCS, Kandiah N. Hippocampal subfield atrophy of CA1 and subicular structures predict progression to dementia in idiopathic Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2019;90:681–7.
8. Foo H, Mak E, Jude R, Ng A, Lok W, Yian Y, et al. NeuroImage : Clinical Associations of hippocampal sub fi elds in the progression of cognitive decline related to Parkinson ’ s disease. 2017;14:37–42.
9. La C, Linortner P, Bernstein JD, Ua Cruadhlaoich MAI, Fenesy M, Deutsch GK, et al. Hippocampal CA1 subfield predicts episodic memory impairment in Parkinson’s disease. NeuroImage Clin. 2019;23.
10. O’shea DM, De Wit L, Tanner J, Mejia Kurasz A, Amofa P, Perez Lao A, et al. Hippocampal Subfields in Mild Cognitive Impairment: Associations with Objective and Informant-Report of Memory Function. Arch Clin Neuropsychol. 2022;37:1502–14.
11. Wang N, Zhang L, Yang HG, Luo XG, Fan GG. Do multiple system atrophy and Parkinson’s disease show distinct patterns of volumetric alterations across hippocampal subfields? An exploratory study. Eur Radiol. 2019.
12. Song Y, Yang J, Chang M, Wei Y, Yin Z, Zhu Y, et al. Shared and distinct functional connectivity of hippocampal subregions in schizophrenia, bipolar disorder, and major depressive disorder. Front Psychiatry. 2022;13.
Figures