4172
Non-rigid motion-compensated MR Multitasking for free-breathing low-dose dynamic contrast-enhanced MRI in the abdomen1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 3Department of Bioengineering, University of California, Los Angeles, CA, United States, 4Karsh Division of Gastroenterology and Hepatology, Cedars-Sinai Medical Center, Los Angeles, CA, United States
Synopsis
Keywords: Sparse & Low-Rank Models, DSC & DCE Perfusion, Pancreas, Abdomen, Quantitative Imaging, Image Reconstruction, Free-breathing
Motivation: Efficient image models are needed to enable low-dose, free-breathing quantitative dynamic contrast-enhanced (DCE) imaging in the abdomen.
Goal(s): Integrate non-rigid motion compensation (MoCo) into the MR Multitasking framework and evaluate its impact on low-dose, free-breathing abdominal DCE.
Approach: Non-rigid MoCo was incorporated into MR Multitasking by directly applying motion fields to eigenimages. This was tested on n=5 healthy volunteers who received 0.02 mmol/kg Gd, only 20% of the standard dose.
Results: Non-rigid MoCo of eigenimages was compatible with MR Multitasking. MoCo more efficiently modeled respiratory motion and minimized intra-bin motion, demonstrating potential for improved DCE quantification.
Impact: Non-rigid motion compensation reduces intra-bin respiratory motion in low-dose free-breathing, whole-abdomen quantitative dynamic contrast-enhanced (DCE) MR Multitasking. Low-dose quantitative DCE may benefit longitudinal monitoring of neoadjuvant treatment in patients with borderline resectable/locally advanced pancreatic ductal adenocarcinoma.
INTRODUCTION
Quantitative dynamic contrast-enhanced (DCE) MRI is a powerful diagnostic and monitoring tool for treatment response of cancers such as pancreatic ductal adenocarcinoma (PDAC). MR Multitasking has shown that a low-rank tensor image model can achieve high spatial and temporal resolution for imaging PDAC1,2 at the standard Gd dose. Low-dose imaging is attractive for longitudinal monitoring, but reduced signal-to-noise ratio warrants more efficient image models than low-rank tensors alone. Non-rigid motion compensation (MoCo) can complement low-rank image models to more efficiently represent respiratory motion3-5, but computation is challenging for large-scale problems. To address these limitations, we integrated non-rigid MoCo into the MR Multitasking framework, directly applying motion fields to spatial factors (eigenimages) to reduce computational cost by 3,000×.METHODS
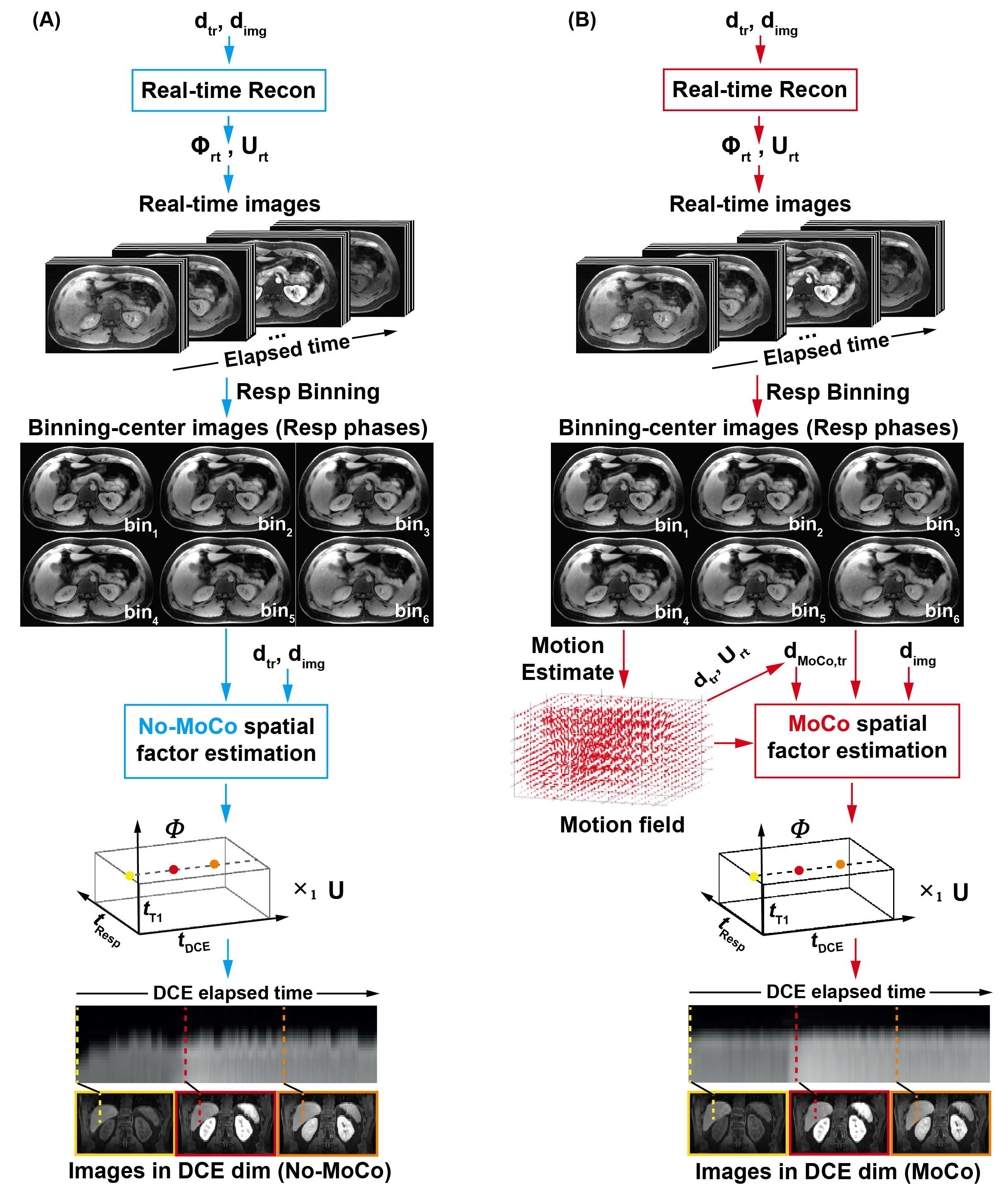
Pulse sequence: A 3D FLASH sequence with periodic nonselective saturation-recovery (SR) preparation used an axial golden-angle stack-of-stars sampling scheme with Gaussian kz density to collect imaging data6. A center k-space line in the superior-inferior direction was acquired every 8 readouts as training data.Image reconstruction: Figure 1 illustrates the reconstruction pipelines for standard Multitasking (No-MoCo) and MoCo Multitasking. In both pipelines, a “real-time” (ungated) basis ($$$\mathbf{\Phi}_{\textrm{rt}}$$$) was generated from the SVD of the training data ($$$\mathbf{d}_{\textrm{rt}}$$$) and used for preliminary estimations of spatial factor $$$\mathbf{U}_{\textrm{rt}}$$$ from the imaging data ($$$\mathbf{d}_{\textrm{img}}$$$). The reconstructed image $$$\mathbf{A}_{\textrm{rt}}=\mathbf{U}_{\textrm{rt}}\mathbf{\Phi}_{\textrm{rt}}$$$ was binned into six respiratory states (bin$$${}_{n}$$$, $$${n}$$$=1,2,…,6).
For MoCo Multitasking, each motion field $$$\mathbf{M}_{n}$$$ mapping the end-expiratory bin (bin1) to bin$$${}_{n}$$$ was estimated from the respiratory bin average images using non-rigid registration in ANTs7. Motion-compensated training data ($$$\mathbf{d}_{\textrm{MoCo,tr}}$$$) were generated by applying the inverse motion fields to $$$\mathbf{U}_{\textrm{rt}}$$$ and re-encoding the central k-space line. A multidimensional tensor subspace basis was then estimated using low-rank tensor completion as in our prior work1, either from $$$\mathbf{d}_{\textrm{tr}}$$$ (for No-MoCo Multitasking) or from $$$\mathbf{d}_{\textrm{MoCo,tr}}$$$ (for MoCo Multitasking). The spatial factor $$$\textbf{U}$$$ was recovered according to
$$ \textbf{U}=\underset{\textbf{U}}{\textrm{argmin}}\sum_{n}^{ }\left\| \mathbf{d}_{\textrm{img},n}-\Omega _{n}\left ( \mathit{\Phi_{n}}\times _{1} \left [ \textbf{FSM}_{n}\mathbf{U} \right ] \right )\right\|_{2}^{2}+R(\textbf{U})$$
where $$$\Omega _{n}$$$ applies (k,t)-space undersampling corresponding to $$$\mathbf{d}_{\textrm{img},n}$$$, the subset of imaging data at motion state $$${n}$$$,$$$\mathit{\Phi}_{n}$$$ is a subtensor the temporal factor at bin $$${n}$$$, $$$\textbf{F}$$$ takes the Fourier transform, $$$\textbf{S}$$$ applies coil sensitivities, and R(·) is wavelet sparse regularization. No-MoCo Multitasking solved the same problem with $$$\mathbf{M}_{n}=\mathbf{I}$$$. The final multidimensional image tensor $$$\textit{A}$$$ was computed as $$$\textit{A} = \mathit{\Phi}_{n}\times_{1}\mathbf{U}$$$.
Imaging experiments: All data were acquired on a 3T scanner (VIDA, Siemens) with the following parameters: TE/TR = 2.2/6.1ms, SR period = DCE temporal resolution=1030ms, Flip angle=8°, scan time=10min, acquisition matrix=224×224×50 with 15% oversampling in kz direction, spatial resolution=1.3×1.3×4.0–1.5×1.5×4.0mm3. A 20%-dose (0.02mmol/kg) of Gadavist contrast agent was administered 2 minutes into the scan at the rate of 2ml/s. Five healthy volunteers were enrolled. Liver-dome positions were tracked across the DCE dimension within the end-expiratory bin (bin1) to measure intra-bin motion. A one-tailed paired t-test tested the hypothesis that MoCo reduced the standard deviation of liver-dome position within bin1.
RESULTS
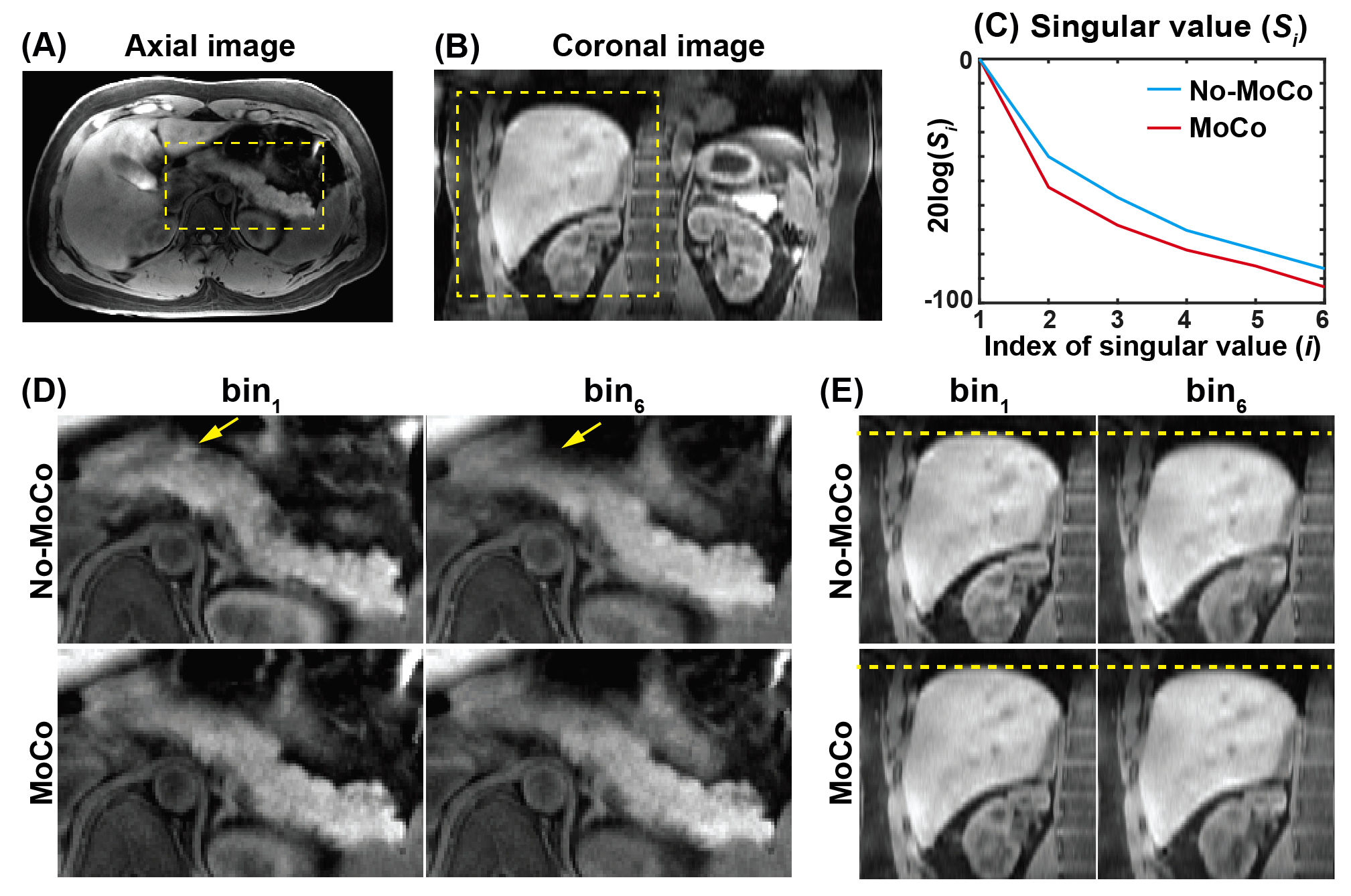
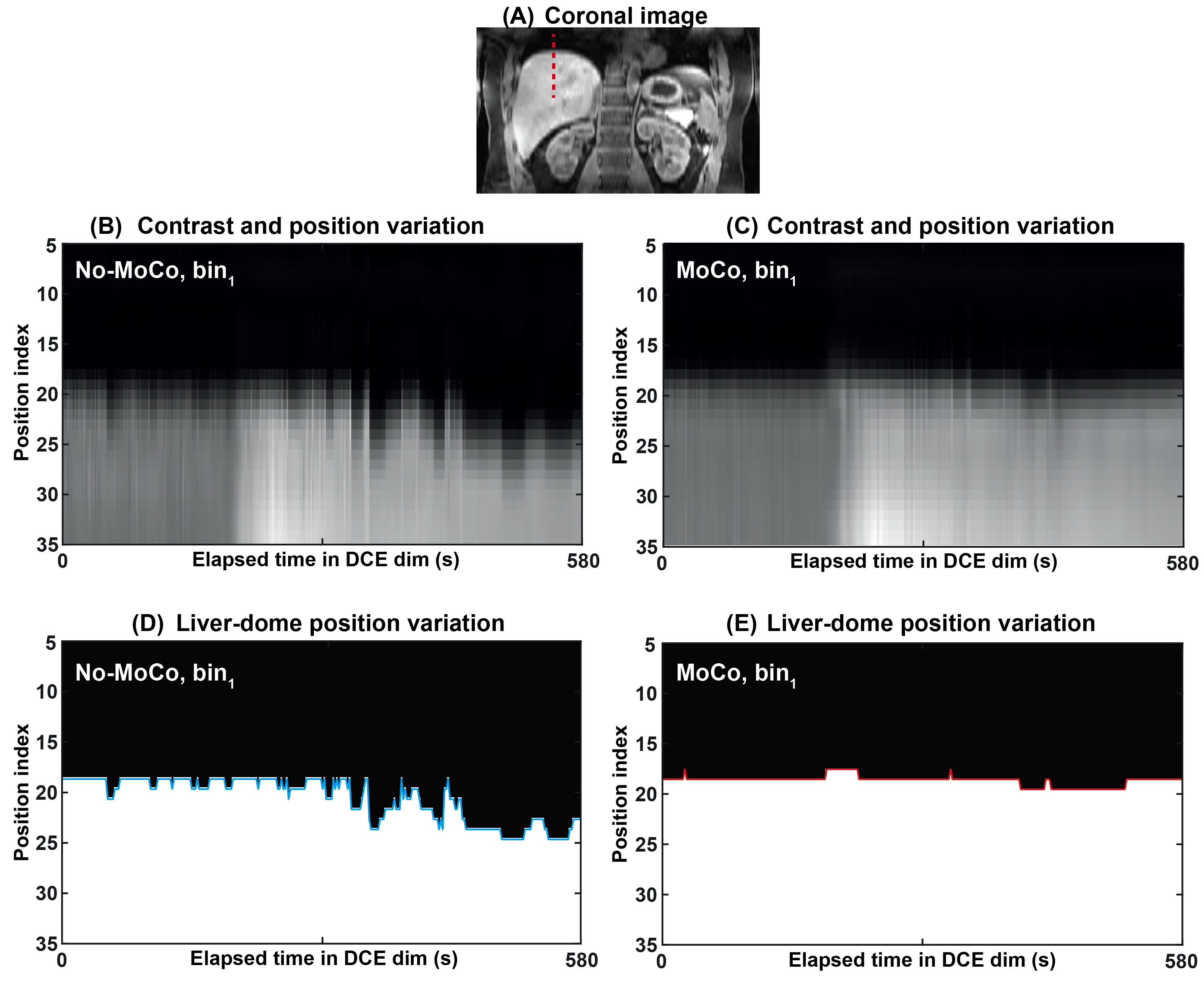
Figure 2 shows the images of the arterial phase (~200s) from No-MoCo and MoCo Multitasking. The MoCo Multitasking high-order singular values along the respiratory dimension decay more quickly than No-MoCo Multitasking, indicating a lower effective rank. MoCo reduced variation between bin1 (end-expiration) and bin6 (end-inspiration) as intended.Figure 3 shows the contrast and position variations of a 1D liver-dome profile along the DCE dimension in bin1. The 1D profile from MoCo Multitasking has a more stable liver-dome position than that from No-MoCo Multitasking.
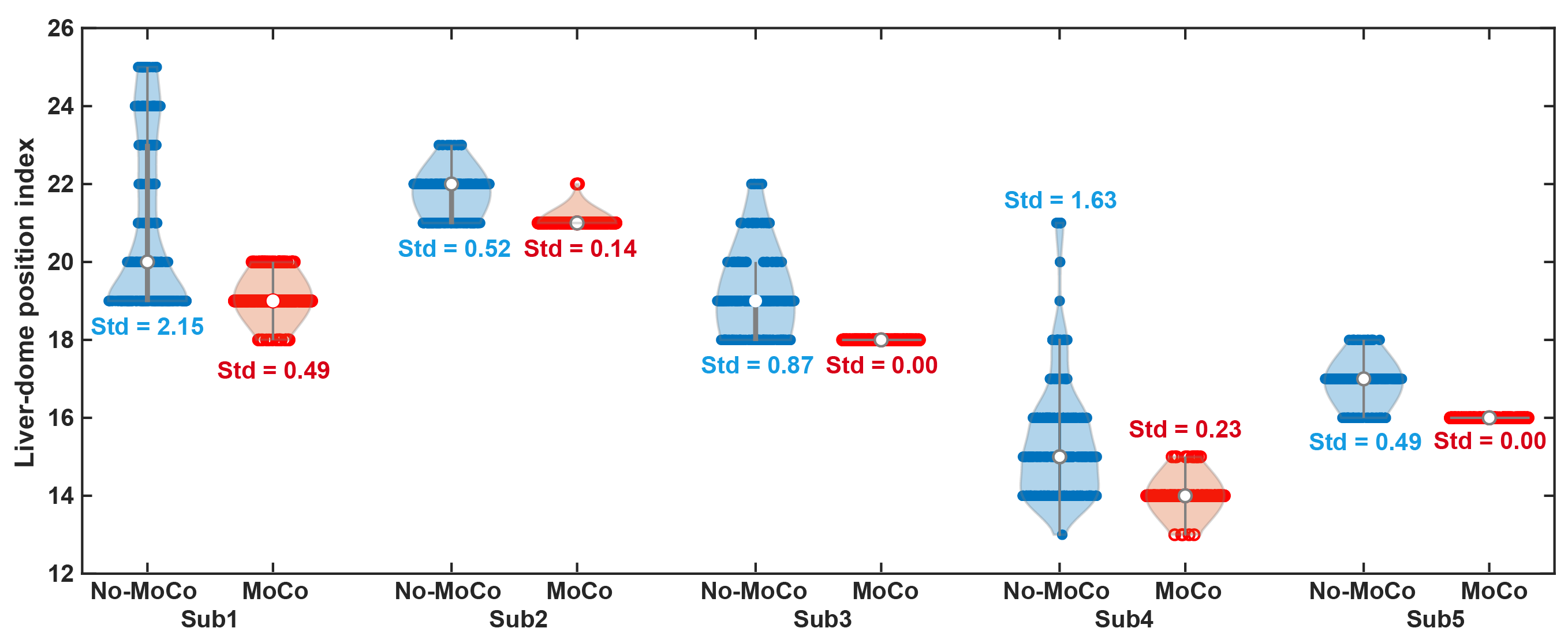
Fig. 4 shows the detected liver-dome position within bin1 for all reconstructions, along with standard deviations. MoCo Multitasking reduced liver-dome position variation (p=0.009), confirming reduced intra-bin motion.
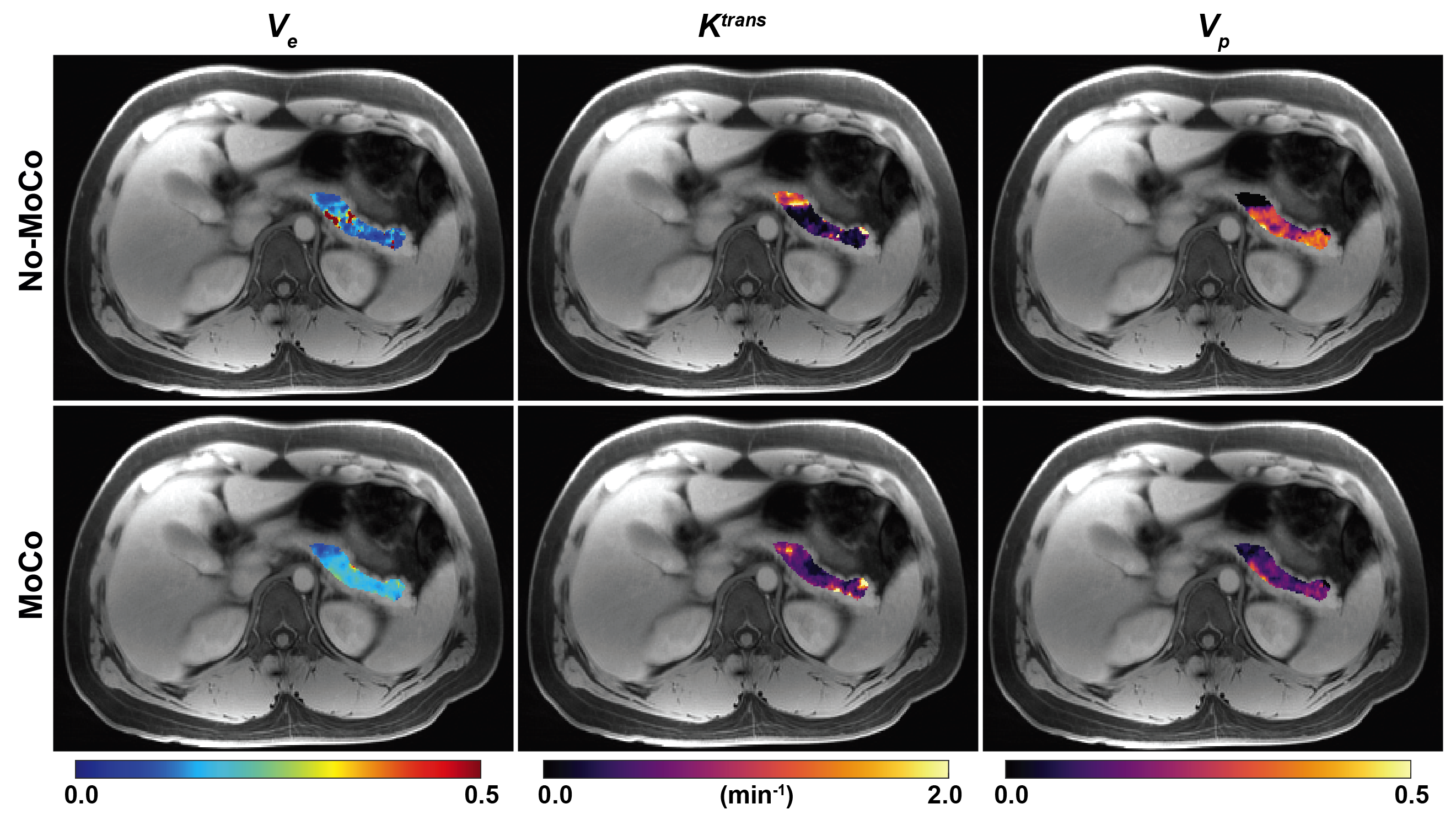
Figure 5 shows quantitative pancreatic DCE maps for a representative subject. Unreasonable values and abrupt changes appear on the DCE maps from No-MoCo Multitasking. The MoCo images are more homogeneous within the pancreas (as expected for healthy subjects) and produced average Ve, Ktrans, and Vp values more consistent with those reported in our previous standard-dose DCE studies1,2.
DISCUSSION
Directly applying motion fields to eigenimages rather than time-domain images makes non-rigid MoCo practical for high-dimensional MR Multitasking, with 3,045× fewer Fourier transforms and motion deformations. Non-rigid MoCo reduced the rank in the respiratory dimension, indicating more efficient modeling for respiratory motion, crucial for low-dose DCE imaging. MoCo reduced intra-bin motion in the end-expiratory bin and showed potential for improved DCE quantification. The potential for reliable low-dose free-breathing DCE application warrants further study in a larger cohort, including patients, assessing repeatability/reproducibility, and comparing with standard-dose DCE MRI.CONCLUSION
Non-rigid MoCo can be applied directly to eigenimages in MR Multitasking, reducing intra-bin motion in low-dose free-breathing abdominal DCE imaging.Acknowledgements
This work was partially supported by NIH R01 EB032801.References
1. Wang N, Gaddam S, Wang L, et al. Six-dimensional quantitative DCE MR Multitasking of the entire abdomen: Method and application to pancreatic ductal adenocarcinoma. Magn Reson Med. 2020; 84: 928–948.
2. Wang N, Gaddam S, Xie Y, et al. Multitasking dynamic contrast enhanced magnetic resonance imaging can accurately differentiate chronic pancreatitis from pancreatic ductal adenocarcinoma. Front Oncol. 2023; 12:1007134.
3. Scannell M, Villa ADM, Lee J, et al. Robust Non-Rigid Motion Compensation of Free-Breathing Myocardial Perfusion MRI Data. IEEE Trans Med Imaging. 2019; 38: 1812-1820.
4. Cruz G, Qi H, Jaubert O, Kuestner T, et al. Generalized low-rank nonrigid motion-corrected reconstruction for MR fingerprinting. Magn Reson Med. 2022;87: 746-763.
5. Tan F, Zhu X, Chan M, et al. Motion-compensated low-rank reconstruction for simultaneous structural and functional UTE lung MRI. Magn Reson Med. 2023; 90: 1101-1113.
6. Wang N, Cao T, Han F, et al. Free‐breathing multitasking multi‐echo MRI for whole‐liver water‐specific T1, proton density fat fraction, and quantification. Magn Reson Med. 2021; 87: 120–137.
7. Avants BB, Tustison N, Song G. Advanced normalization tools (ANTS). Insight j. 2009; 2:1-35.
Figures