4168
Non-contrast Time-resolved 4D MR Angiography Reconstruction using Compressed Sensing with Sparsity Regularization and Subspace Modeling1School of Biomedical Engineering, ShanghaiTech University, Shanghai, China, Shanghai, China, 2United Imaging Healthcare, Shanghai, China, Shanghai, China
Synopsis
Keywords: Sparse & Low-Rank Models, Image Reconstruction
Motivation: ASL-based non-contrast enhanced (non-CE) time-resolved 4D MRA is a promising approach in the diagnosis of cerebrovascular disease, however, it suffers from low SNR and insufficient spatial and temporal resolution.
Goal(s): Our goal was to enhance the quality of 4D non-CE MRA and diminish artifacts.
Approach: This study proposed a novel reconstruct method combining the angiography sparsity and subspace modeling on data acquired by golden-angle stack-of-stars radial pulse sequence.
Results: The performance of the proposed method was compared with NUFFT, conventional GRASP and the state-of-the-art GRASP-pro reconstructions. The results suggest that the proposed method improves the image quality of the 4D ASL-based non-CE MRA.
Impact: The proposed reconstruction method can produce 4D non-CE MRA with high spatial-temporal resolution.
Introduction
Time-resolved magnetic resonance angiography (MRA) based on arterial spin labeling (ASL) technique using arterial blood as an endogenous tracer can obtain dynamic angiographic images without injection of exogenous contrast agents, and provides fine details about anatomy and hemodynamics in cerebrovascular disorders such as AVM and Moyamoya disease1. The main challenges facing the ASL-based non-contrast 4D MRA imaging technique include the low signal-to-noise ratio (SNR) of ASL and the slow acquisition speed leading to the tradeoff between spatial and temporal resolution. In recent years, several methods combined low-rank subspace-based reconstruction algorithm and the sparsity of individual image with stack-of-stars golden-angle radial sampling to achieve higher temporal resolution2,3. Nevertheless, these methods only exploit the sparsity of the original control or label image without considering the sparsity of the angiographic images. In this study, we propose a reconstruction method combines the inherent sparsity of angiography images4,5 and subspace modeling on data acquired by stack-of-stars golden-angle radial pulse sequence to improve the quality of dynamic MRA images. The performance of the proposed method was compared with NUFFT, conventional GRASP2 and the state-of-the-art GRASP-pro3 methods.Methods
MRI data acquisition:After IRB approval and obtaining written informed consent, the MRI experiment was performed in a healthy subject, on an uMR890 3.0T scanner (United Imaging Healthcare, Shanghai, China) with 64 channel head coil. Dynamic MRA data were acquired by flow-sensitive alternating inversion recovery (FAIR) ASL labeling scheme and GRE-based 3D stack-of-stars golden-angle radial acquisition6. The key imaging parameters included: FOV = 208mm×208mm, 80 slices, TE/TR = 1.8/4.5ms, bandwidth = 600Hz/pixel, flip angle = 10 degrees, spatial resolution = 1×1×1.5mm3. Coil compression from 64 channels to 16 was performed on k-space data in order to reduce the data size.
Image Reconstruction:
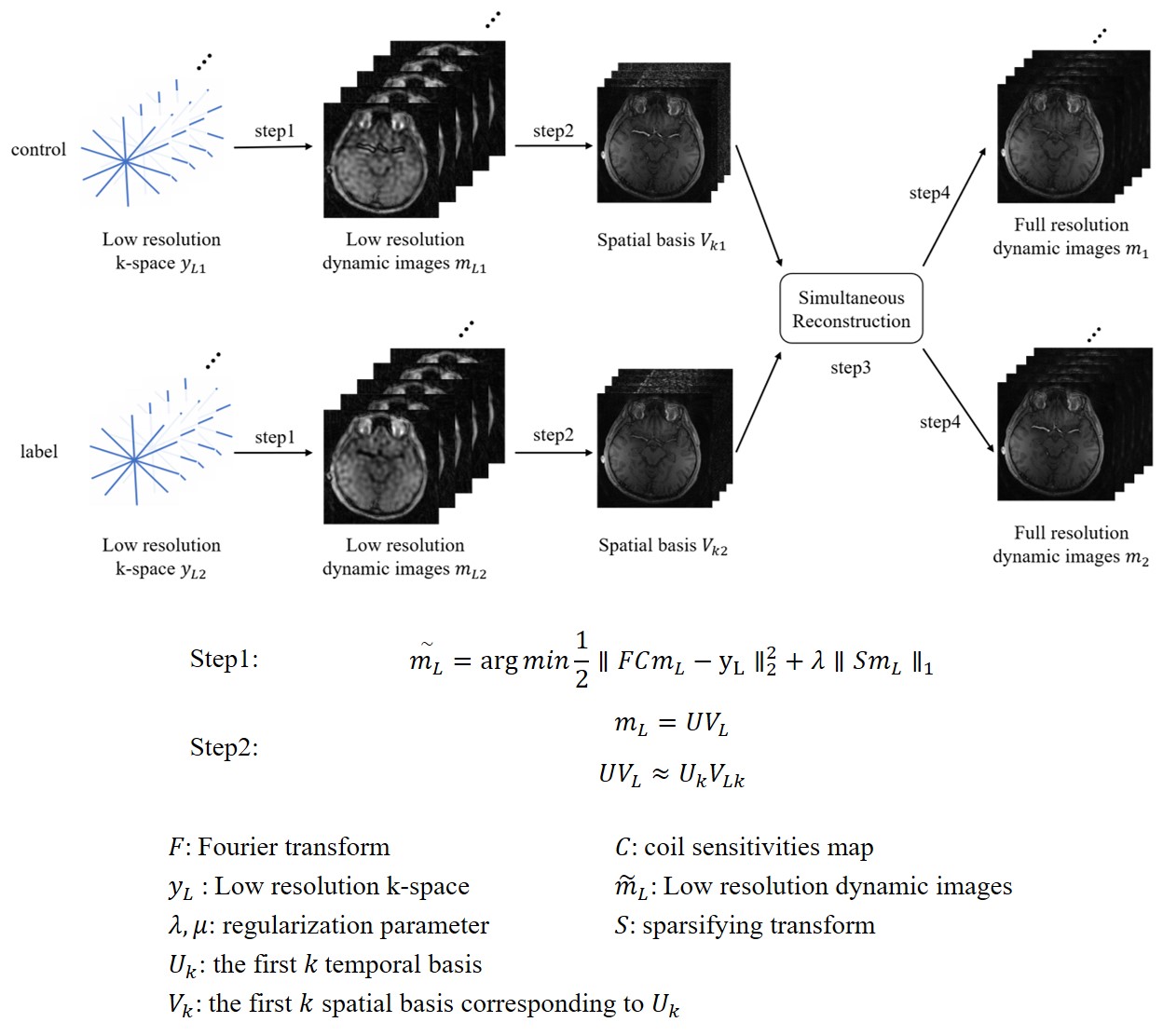
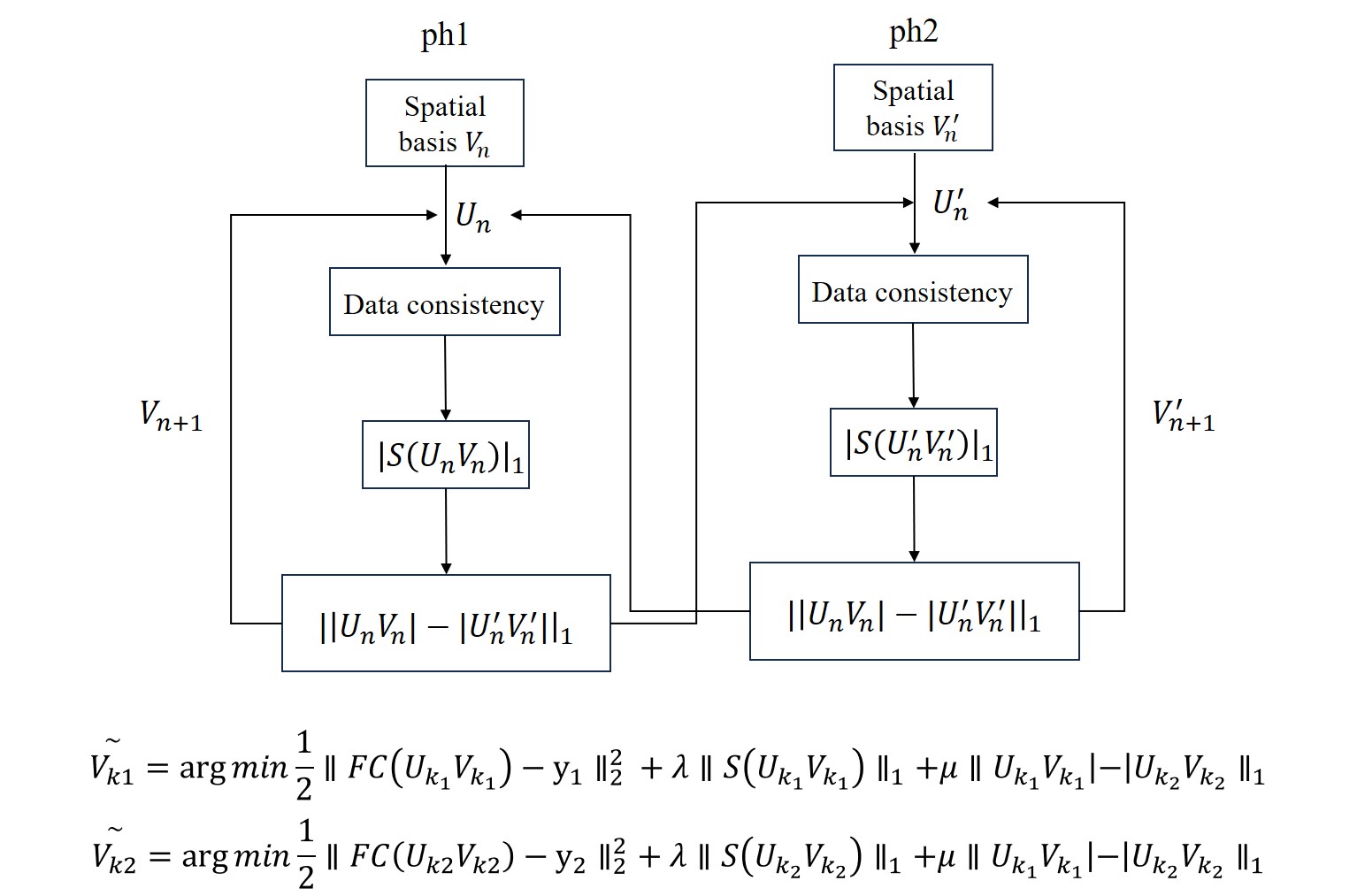
As shown in Figure 1, the proposed method can be described in four steps: (1) the low resolution dynamic image series $$$m_L$$$ for ASL control and label images were reconstructed separately using the central portion of the corresponding k-space data $$$y_L$$$; (2) the temporal basis $$$U_k$$$ and spatial basis $$$V_k$$$ for the control or label images were generated from the low resolution dynamic image series by single value decomposition (SVD); (3) the temporal basis $$$U_k$$$ is used as a prior to optimize the subspace images with the constraint of the subtraction term. The control and label phases are reconstructed simultaneously (Details shown in Figure 2), the results from the last iteration will be fed into the next iteration with sparsity constraints on the subtraction of the control and label images; (4) the full resolution dynamic image series of control and label are composed by the optimized spatial basis $$$\tilde{V_k}$$$ and temporal basis $$$U_k$$$. After reconstruction of ASL control and label images, maximum intensity projection (MIP) was performed on their subtraction to display blood flow dynamics.
The same MR raw data was also reconstructed using NUFFT, GRASP and GRASP-Pro methods for comparison.
Results
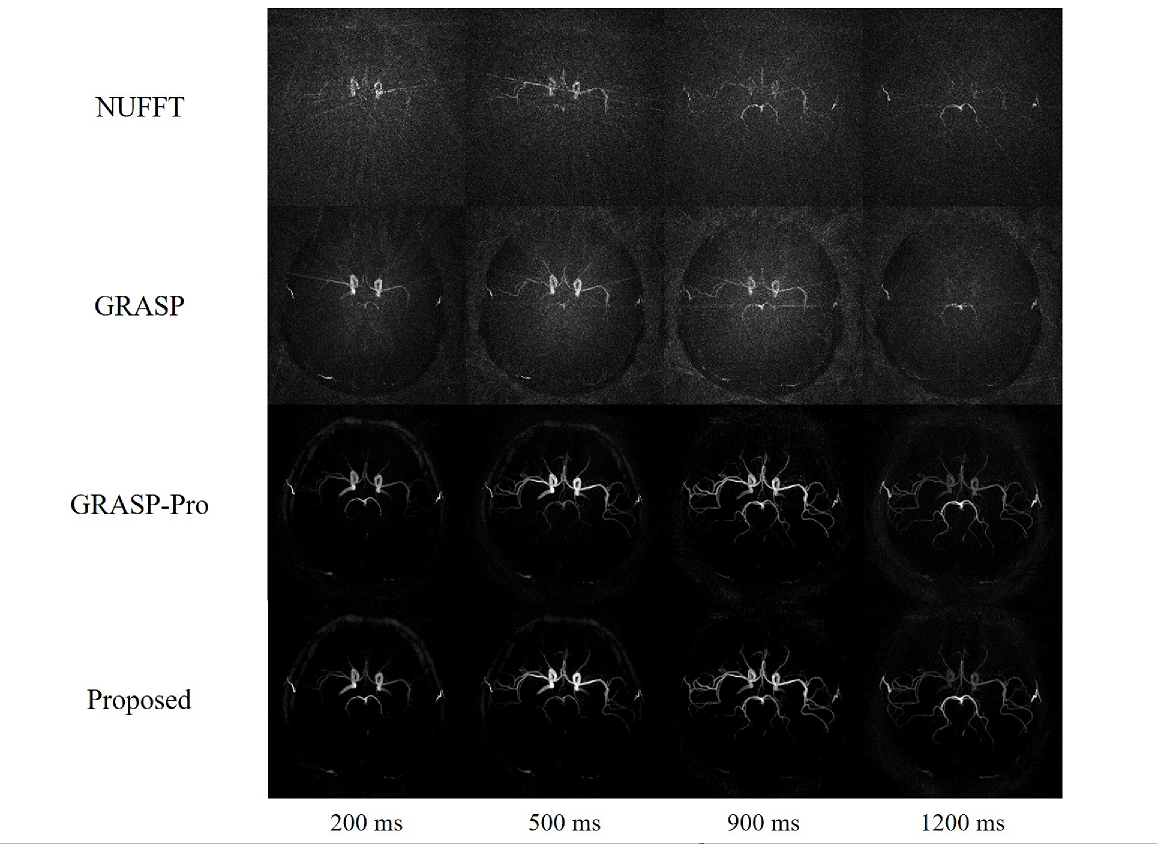
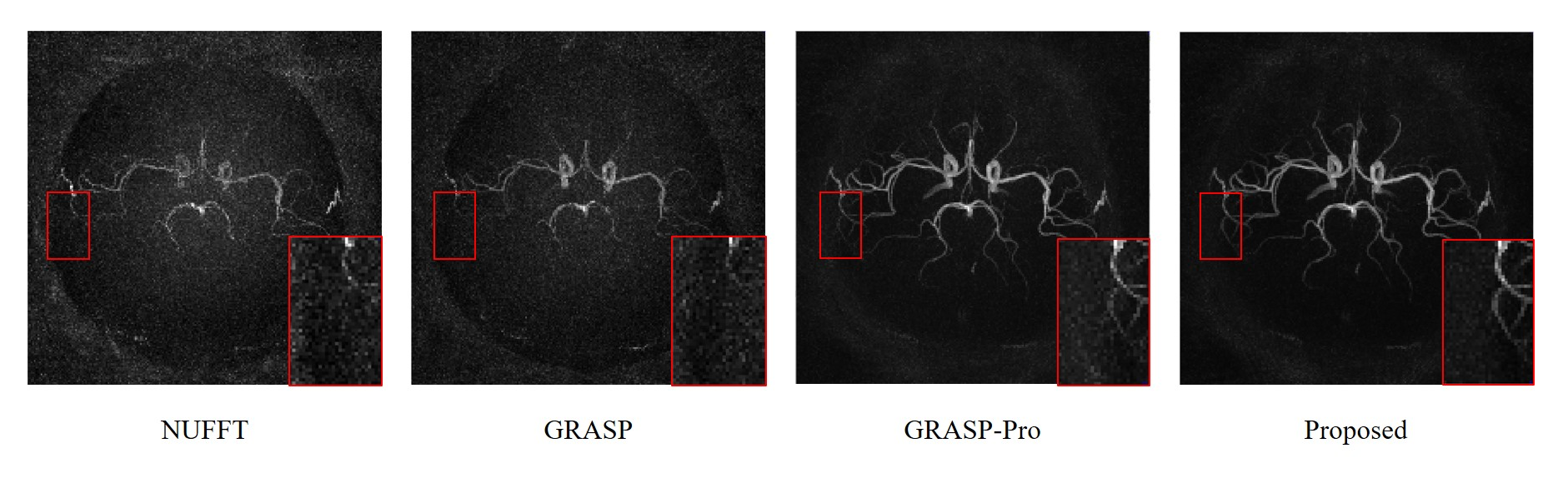
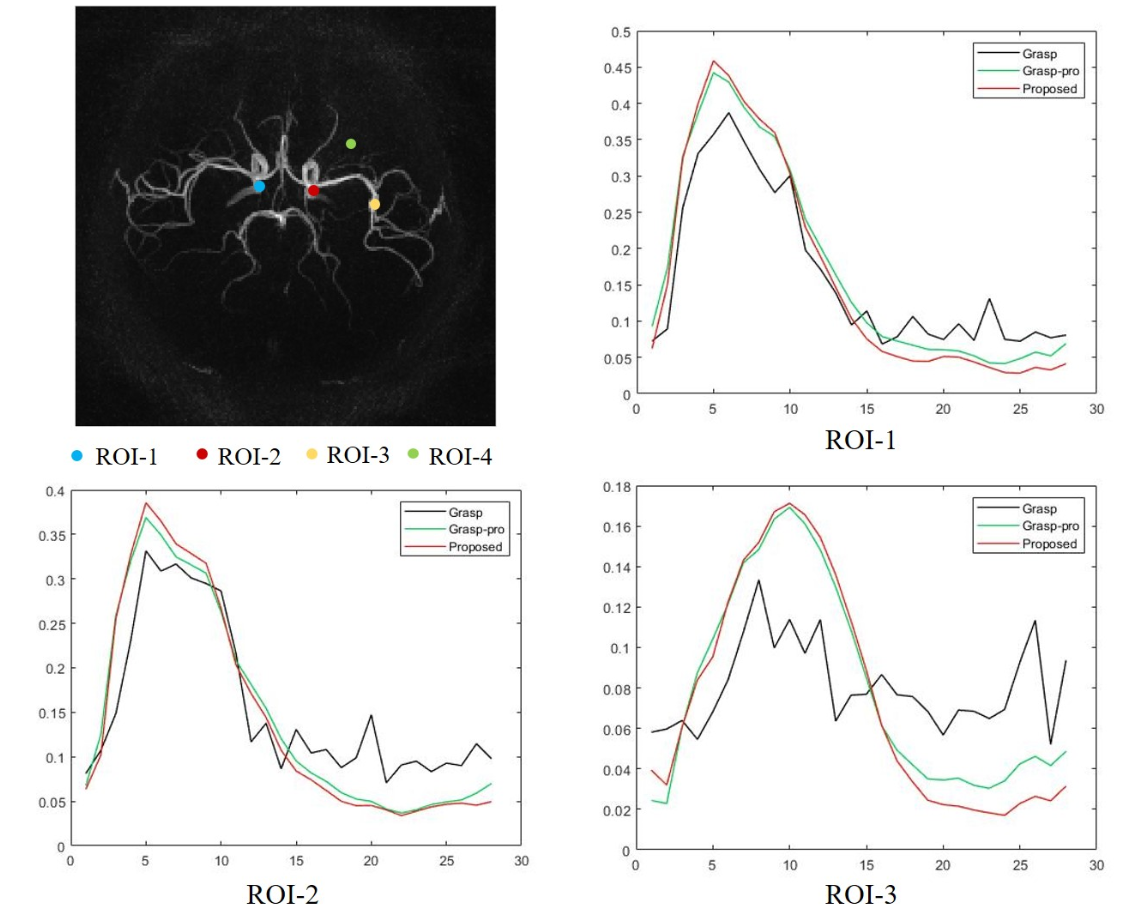
Figure 3 shows several representative frames of MIP images reconstructed with 15 spokes per frame using NUFFT, GRASP, GRASP-Pro and the proposed method. It can be seen that the proposed method has overall similar image quality to GRASP-Pro, both of which outperformed NUFFT and GRASP methods with significantly lower background noise level and fewer artifacts. A closer inspection of distal vessels in Figure 4 demonstrates that the proposed method can improve the sharpness of the blood vessels and reduce the background noise even further compared to the GRASP-Pro method. Figure 5 illustrates the time course signals of three vascular ROIs in the reconstructions with GRASP, GRASP-Pro and the proposed method. It can be seen that the proposed method reduced image noise without compromising the temporal fidelity. Signal-to-noise ratio (SNR) was calculated for GRASP-Pro and the proposed method, using the approach described in [7]. Briefly, a 5×5 square ROI was drawn on the vessel signal (Fig.5 ROI-2) and adjacent background (Fig.5 ROI-4) on the MIP image to measure the SNR at the time point with peak signal among the time series. SNR was calculated by the ratio of the mean signal to the standard deviation of background noise. The proposed method (SNR = 79.4) achieved 14% increase of SNR compared with GRASP-Pro (SNR = 69.7).Conclusion
The proposed method utilized the inherent sparsity of blood vessel images and subspace modeling to reconstruct the ASL-based 4D MRA images. The results suggest that it improves the image quality with higher SNR and better blood vessel delineation. Future studies will test the proposed method in more subjects.Acknowledgements
NoneReferences
1. Yu S, Yan L, Yao Y, Wang S, Yang M, Wang B, Zhuo Y, Ai L, Miao X, Zhao J, Wang DJ. Noncontrast dynamic MRA in intracranial arteriovenous malformation (AVM), comparison with time of flight (TOF) and digital subtraction angiography (DSA). Magn Reson Imaging. 2012 Jul; 30(6):869-77.
2. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2014 Sep;72(3):707-17.
3. Feng L, Wen Q, Huang C, Tong A, Liu F, Chandarana H. GRASP-Pro: imProving GRASP DCE-MRI through self-calibrating subspace-modeling and contrast phase automation. Magn Reson Med. 2020 Jan;83(1):94-108.
4. Zhou Z, Han F, Yu S, Yu D, Rapacchi S, Song HK, Wang DJJ, Hu P, Yan L. Accelerated noncontrast-enhanced 4-dimensional intracranial MR angiography using golden-angle stack-of-stars trajectory and compressed sensing with magnitude subtraction. Magn Reson Med.2018; 79:867-878.
5. Rapacchi S, Han F, Natsuaki Y, Kroeker R, Plotnik A, Lehrman E, Sayre J, Laub G, Finn JP, Hu P. High spatial and temporal resolution dynamic contrast-enhanced magnetic resonance angiography using compressed sensing with magnitude image subtraction. Magn Reson Med. 2014 May;71(5):1771-83.
6. Kim SG. Quantification of relative cerebral blood flow change by flow-sensitive alternating inversion recovery (FAIR) technique: application to functional mapping. Magn Reson Med 1995; 34:293–301.
7. Song HK, Yan L, Smith RX, Xue Y, Rapacchi S, Srinivasan S, Ennis DB, Hu P, Pouratian N, Wang DJJ. Noncontrast enhanced four dimensional dynamic MRA with golden angle radial acquisition and K-space weighted image contrast (KWIC) reconstruction. Magn Reson Med. 2014; 72:15411551.
Figures