4165
Identification of Relative Factors for Degraded Image Quality in Free-Breathing Dynamic Abdominal MRI1Department of Radiology, Gifu University, Gifu, Japan, 2Department of Radiology Services, Gifu University Hospital, Gifu, Japan, 3Philips Japan, Tokyo, Japan, 4Center for One Medicine Innovative Translational Research, Institute for Advanced Study, Gifu University, Gifu, Japan
Synopsis
Keywords: Liver, Body
Motivation: The image quality of free-breathing sequence (4D FreeBreathing) is not stable.
Goal(s): To identify the relative factors for degraded image quality in 4D FreeBreathing.
Approach: Images using 4D FreeBreathing sequence were retrospectively obtained from 73 patients and logistic regression analysis was conducted.
Results: The presence of cirrhosis and unacceptable image quality on pre-contrast images were the relative factors for degraded image quality in 4D FreeBreathing.
Impact: It is not preferable to perform 4D FreeBreathing in patients with cirrhosis and unacceptable image quality in pre-contrast scanning. Using the information of cirrhosis and image quality at pre-contrast, we may be able to select the appropriate candidates.
INTRODUCTION
Dynamic contrast-enhanced imaging needs multiple breath-holds; however, degraded image quality is often observed due to its susceptibility to body motion. To address this issue, free-breathing sequence (4D FreeBreathing) has been recently introduced and the clinical usefulness has been reported1. Still, unacceptable image quality can be seen in some cases even in 4D FreeBreathing. In the present study, we attempted to identify the relative factors for unacceptable image quality in 4D FreeBreathing.METHODS
This retrospective study was approved by our IRB, and written informed consent was waived. Seventy-three patients who underwent free-breathing dynamic abdominal MRI between April 2022 and September 2023 were included. From the hospital information system matching with the time of MRI, we obtained each patients’ demographics and underlying diseases including chronic hepatitis B and C, cirrhosis, alcoholic liver disease, NASH, liver metastasis, coronary disease, lung disease, ascites, and plural effusion.Using a 3T MRI scanner (Ingenia 3.0T CX; Philips Healthcare) equipped with a 32-channel digital coil, we performed dynamic contrast-enhanced abdominal MRI. Scanning parameters were as follows: repetition time/echo time, 4.0/1.86 msec; flip angle, 12 degrees; acquisition voxel size, 1.56 × 1.56 × 4.00 mm3; field of view, 40 × 40 cm2; the number of slices, 100; CS factor, 2.0 (in-plane)/2.0 (through-plane). Multiphasic imaging was immediately started after the start of contrast agent administration. The scan duration of 3 minutes was required to capture from the arterial to delayed phases. A footprint of 30 seconds and temporal resolution of 10 seconds were used in this study. Gd-EOB-DTPA or Gd-BT-DO3A was used as contrast agent.
Before the image analyses, the study coordinator selected the optimal images for the arterial and portal venous phases. A radiologist randomly reviewed the images at pre-contrast, arterial, portal venous, and delayed phases and assigned confidence scores for motion, streak, and overall image quality using a 5-point scale. Acceptable image quality was defined as ≥ 3 points in the overall image quality. The patients were classified into two groups based on the overall image quality at the arterial phase: acceptable image quality (acceptable group) and non-acceptable image quality (unacceptable group).
The Mann-Whitney U and Fisher’s exact tests were conducted to compare the clinical information and confidence scores between the acceptable and unacceptable groups. The statistically significant parameters which can be acquired pre-contrast were included in the logistic regression analysis to determine the relative factors associated with unacceptable image quality in 4D FreeBreathing. A P value of less than 0.05 was considered to be significant.
RESULTS
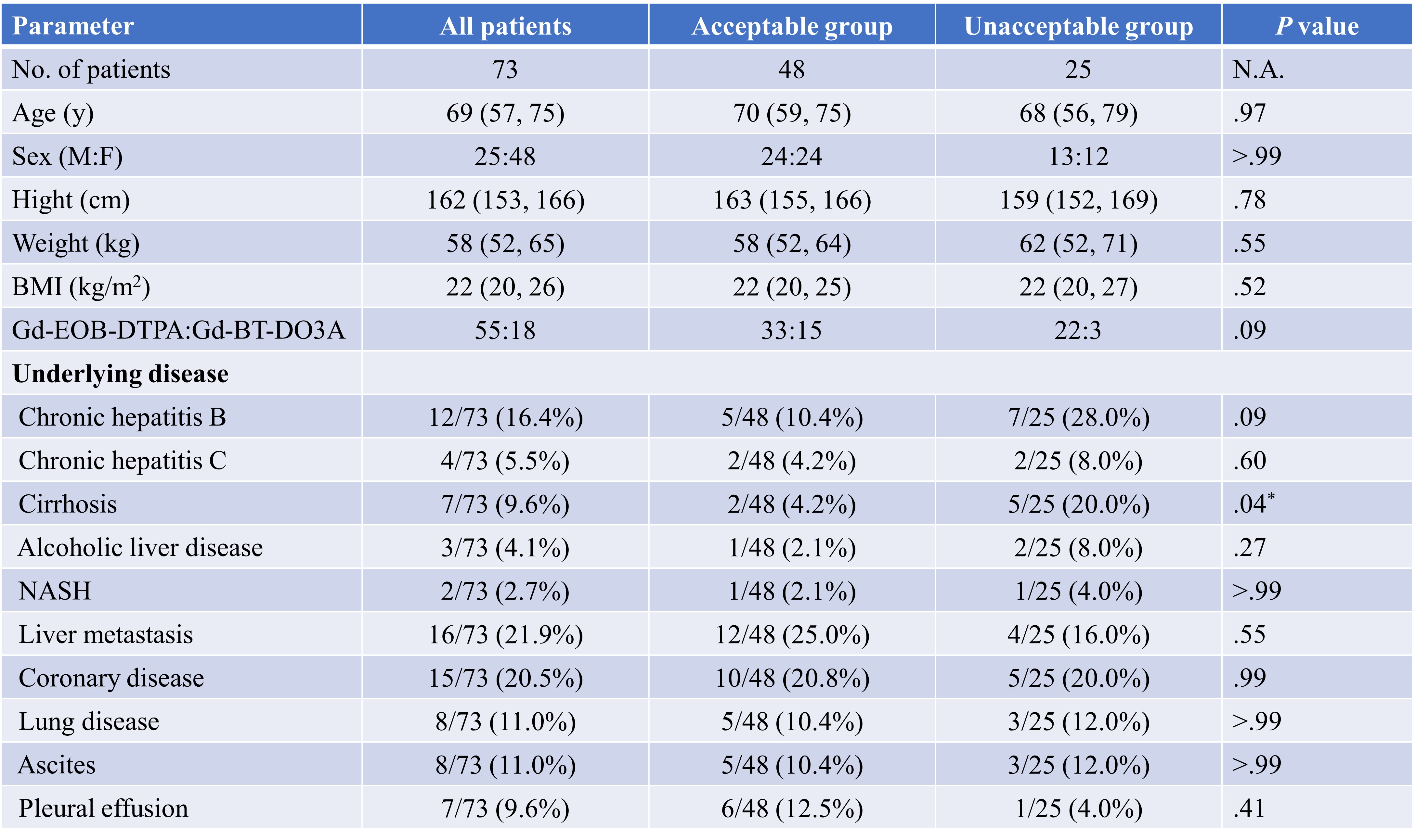
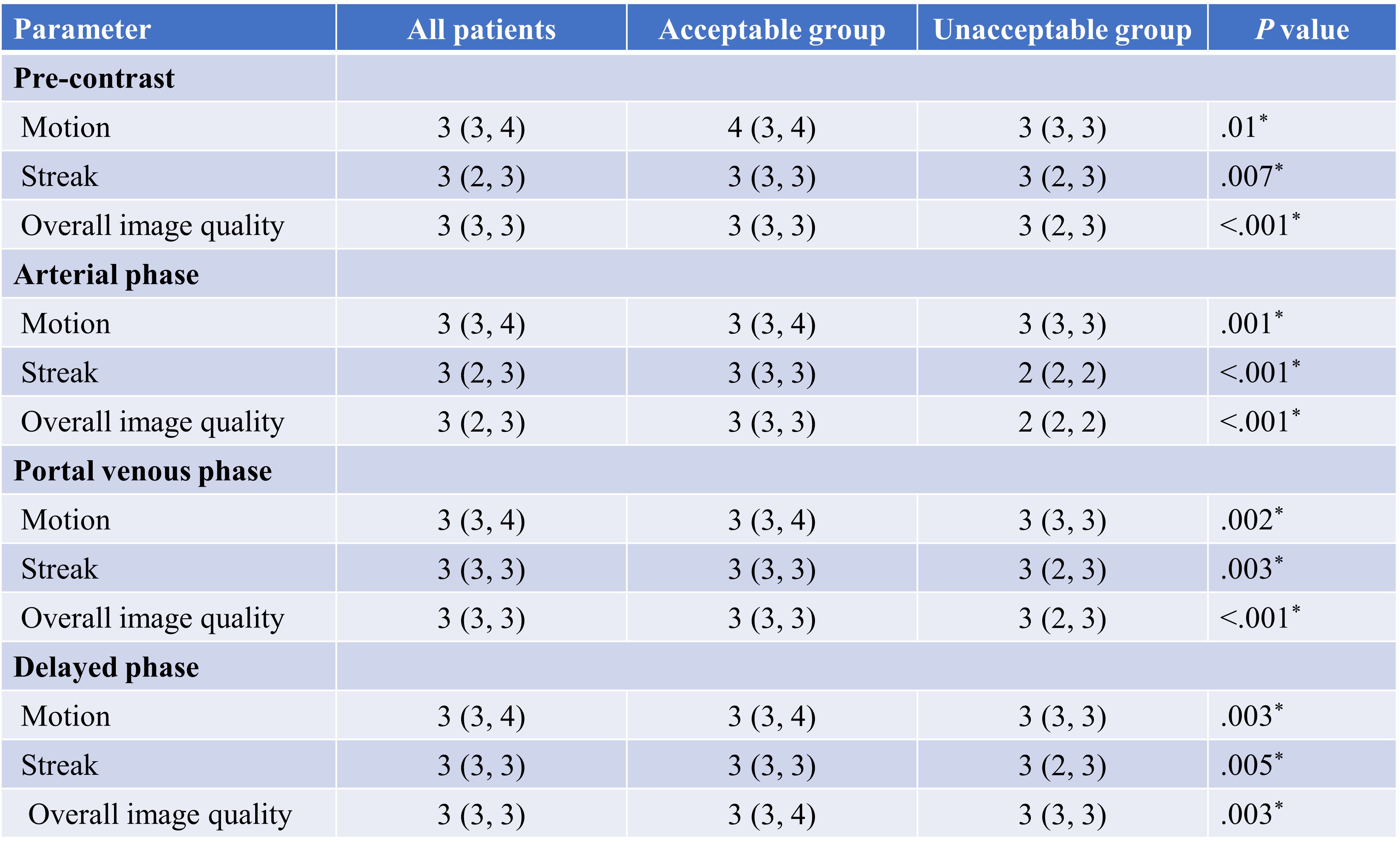
Patients’ demographics and underlying diseases are summarized in Table 1. Among the 73 patients, 48 (65.8%) were classified in the acceptable group and 25 (34.2%) were the unacceptable group. Only the proportion of cirrhosis was different between the two groups (4.2% in acceptable group vs. 20.0% in unacceptable group; P = .04). No difference was found in all other parameters between the two groups (P = .09–>.99).All confidence scores regardless of scan phases were higher in the acceptable group than in the unacceptable group (P <.001–.007; Table 2).
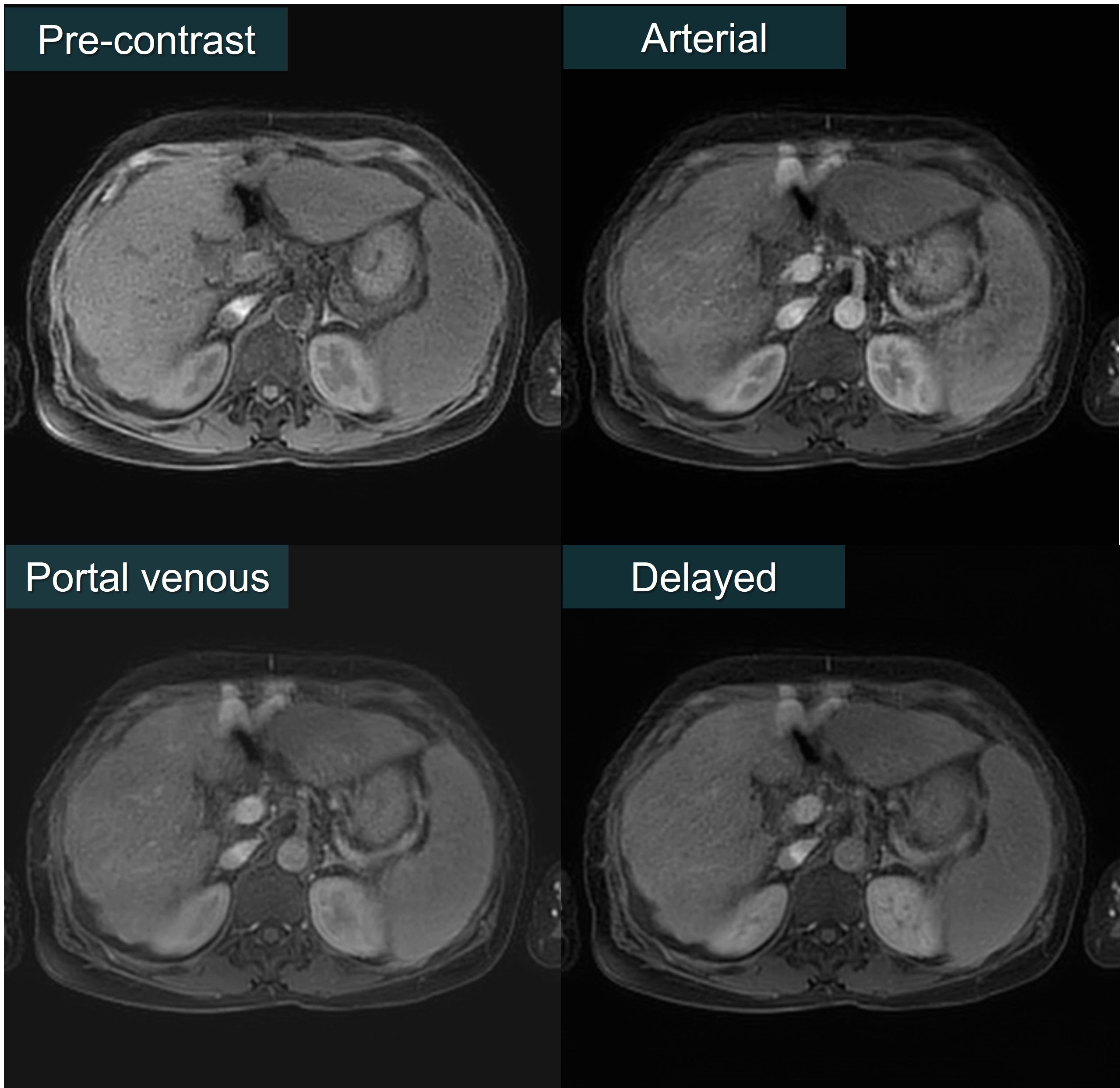
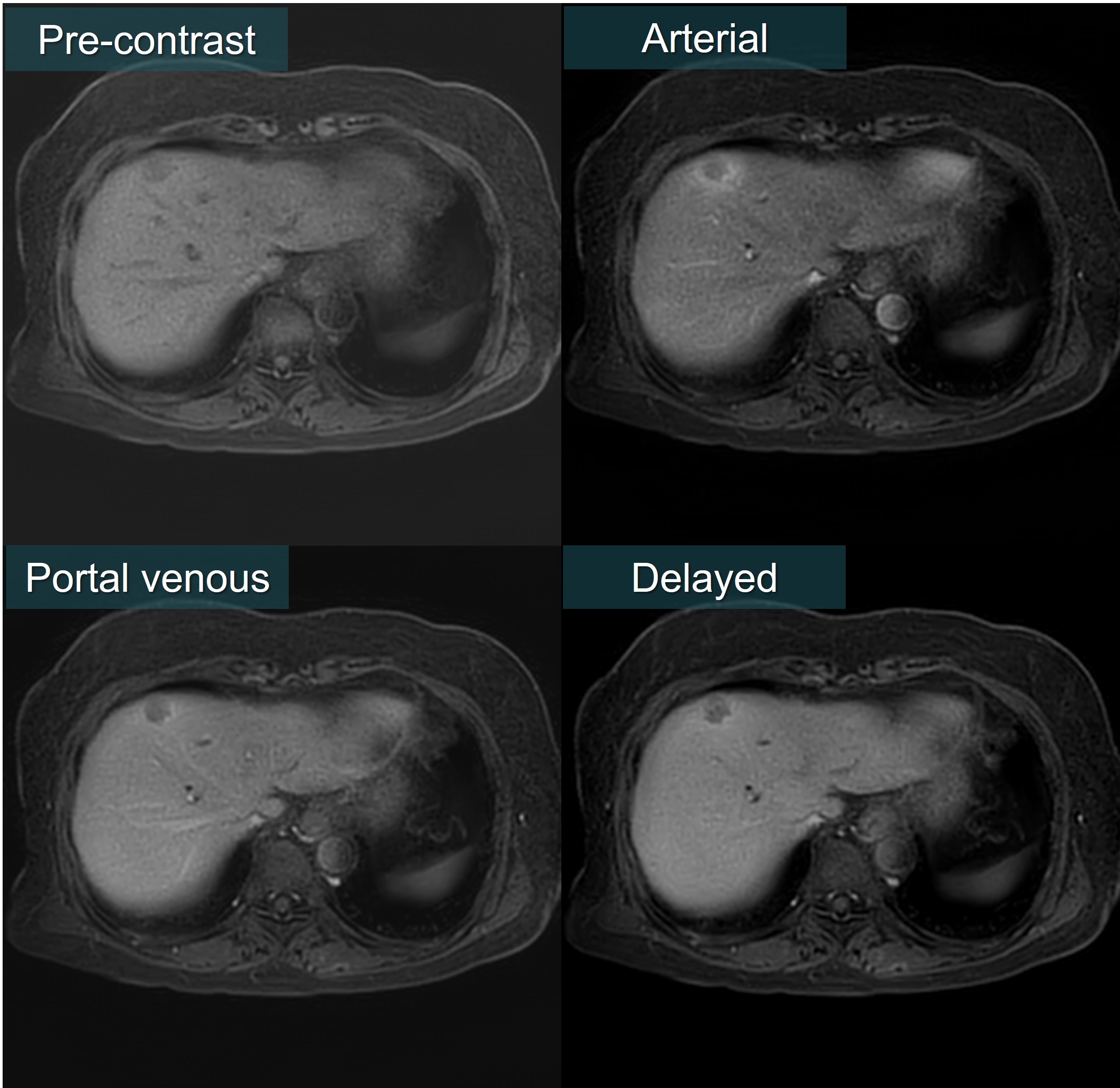
Based on the results, the presence or absence of cirrhosis, the confidence scores for motion, streak, and overall image quality at pre-contrast were included in the logistic regression analysis and only cirrhosis (P = .03) and overall image quality at pre-contrast (P = .02) were identified as the relative factors (Table 3; Figures 1 and 2). Using the fitted logistic regression equation, the sensitivity, specificity, and area under the curve for predicting unacceptable image quality in 4D FreeBreathing were calculated as 56.0%, 91.7%, and 0.79, respectively, by receiver operating characteristics curve analysis.
DISCUSSION
Free-breathing sequence is being applied to abdominal dynamic contrast-enhanced study; however, degraded image quality is also seen in some cases. The rate of acceptable image quality at the arterial phase was 80.5% in patients with mixed breath-holding capacity and 65.6% in patients with limited breath-holding capacity2. Although the vendors were different between ours and theirs, our result (65.8%) was consistent with their patients with limited breath-holding capacity.Our results demonstrated that the presence of cirrhosis and unacceptable image quality at pre-contrast were the relative factors associated with degraded image quality in 4D FreeBreathing. And these factors can be informed before the scan of dynamic study. Using the information of cirrhosis and image quality at pre-contrast, we may be able to select the appropriate candidates for 4D FreeBreathing because the specificity for predicting unacceptable image quality in 4D FreeBreathing was 91.7%.
CONCLUSION
The presence of cirrhosis and unacceptable image quality at pre-contrast were associated with degraded image quality in 4D FreeBreathing.Acknowledgements
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
1. Endler CH, Kukuk GM, Peeters JM, Beck GM, Isaak A, Faron A et al.: Dynamic liver magnetic resonance imaging during free breathing: A feasibility study with a motion compensated variable density radial acquisition and a viewsharing high-pass filtering reconstruction. Invest Radiol 2022; 57: 470-477.
2. Young Park J, Min Lee S, Sub Lee J, Chang W, Hee Yoon J: Free-breathing dynamic t1wi using compressed sensing-golden angle radial sparse parallel imaging for liver mri in patients with limited breath-holding capability. Eur J Radiol 2022; 152: 110342.
Figures