4164
Dynamic Contrast Images in the Pancreatobililary Regions on 1.5T with DL: Comparison of Images on 3T without DL1Radiology, Seirei Hamamatsu General Hospital, Hamamatsu, Japan, 2Global MR Clincal Solutions and Research Collaborations, GE HealthCare, Hino, Japan
Synopsis
Keywords: Pancreas, Pancreas
Motivation: A clinical 3T MR system is preferably utilized due to higher image quality and better recognition of lesions and anatomy compared to 1.5T MR.
Goal(s): Our goal was to show improved abilities of 1.5T with deep learning reconstruction (DL) in evaluation of the pancreatobiliary regions comparing 3T without DL.
Approach: In 9 patients, image qualities and information of vasculatures and soft tissues of dynamic Gd-contrast images of pancreatobiliary regions on 1.5T with DL were compared to those previously obtained on 3T without DL.
Results: 1.5T systems with DL can provide competitive information to those with 3T systems without DL for the pancreatobiliary regions.
Impact: DL reconstruction can fully utilize a 1.5T MR, providing competitive information to a 3T MR without DL for dynamic contrast studies in the pancreatobiliary regions. This can enhance patient-throughput without major socio-economic investment.
Introduction
Breath-hold dynamic contrast MR study has provided information of characterization of the pancreatobiliary lesions. Because of high SN, 3T systems might be preferably performed. Various features in clinical application of deep learning reconstruction (DL) have been introduced. Recent available DL can improve image quality with noise reduction and sharp edges of soft tissue and vasculatures(AIRTM Recon DL, GEHeathCare:GEHC)(1). Information with 1.5T using DL might be competitive to those with previous obtained on 3T without DL. Accordingly, the purpose was to assess efficiency of DL in dynamic contrast study of pancreatobiliary regions for the evaluation of soft tissues and vasculatures on 1.5T in comparison with on 3T without DL.Materials and Methods
The study was approved by IRB and informed consent was obtained. Population: Among patients undergoing previous 3T MR imaging [ 6 in normal bore of 3T (GEHC) and 3 in wide bore (GEHC)] of pancreatobiliary regions, 9 patients (5men, 4 women, mean 69years old) were selected, who underwent dynamic contrast MR imaging with DL on 1.5T. Pathologies were pancreatic cystic 7 including 5 IPMN, Autoimmune pancreatitis 1, status post resection of pancreatic tumor 1, Among them, Polyp in the gall bladder 1, and adenomyomatosis 1. MR imaging: A 1.5T system (Explorer, GE HealthCare, Milwaukee, 16 channel phased-array multicoil) was used in Breath-hold (BH) dynamic contrast imaging covering the liver and pancreas in transverse plane using Turbo LAVA with ARC and CS using spec IR for fat-sat. The parameters were as follows; ARC factor 2x1, CS factor 1.1, TR 3.3ms, Matrix 256x164, thickness -3.4mm/-50%, imaging time10seconds for one phase. Consecutive 2 phases of images were obtained during one BH after injection of nonspecific Gd-chelate (Gadovist, 0.1mmol/kg body weight, injection rate 1mL/sec) followed by saline flash. With Smart prep (GE HealthCare); five seconds after contrast arrival at the level of the diaphragm and 60sec after triggering of the first phase, dual phase imaging was obtained for arterial and portal phases. The data were postprocessed with DL (1). Original images without DL were generated. Parameters for 3T were as follows, ARC factor 2x1.25, CS factor 1.1, TR 3.3ms, Matrix 288x200, slice thickness 3-3.4mm/-50%. Evaluations: Three sets of MR images in precontrast, first phase in the arterial phase, and 3nd phase as in the portal phase were selected and evaluated. Subjective evaluations: Overall mage quality (IQ) and artifacts (blurring & nose) were evaluated using five-point scale (1 non-diagnostic or sever artifacts to 5 excellent quality or no blurring. With coronal reformation, Edge of liver, pancreas, spleens and small and large bowels were evaluated regarding sharpness. Conspicuity of the lesions in the pancreas was also evaluated. Vasculatures: Partial MIP was applied with reviewer-dependent slab thickness and orientation. Selective recognition of aorta and its branches in 1st phase, Portal vein (PV), SMV, Branches of PV in portal phase were evaluated. In subjective and objective evaluations, Wilcoxon ranked test was used with Bonferroni correction.Results
IQ in 2nd and later phases was good and blurring artifacts were less recognized on 1.5 T with DL and those on 3T (Fig 1-3) (IQ 4.3 vs 4.4, NS). Noise and artifacts were less on images with DL on 1.5T(4.5, 4.5). SI were not significantly different between images with and without DL, but SD of SI was less on images with DL than those without DL. Objective SI were highest on 3T among all images in pre, arterial and portal phases (Figs). In MIP, recognition of arteries and portal veins and other veins best on 1.5T with DL(Fig1-3). Recognitions of the cystic lesions were not significantly different between those on 1.5T with DL and on 3T. Contrast of lesions against the parenchyma was highest on 3T. Visual recognitions of lesions on 1.5T with DL and on 3T were not significantly different.Discussion
Currently improvement of IQ and recognitions of vasculatures including portal veins and arteries and soft tissues on dynamic contrast MR imaging with DL on 1.5T could be made. DL can reduce noise and improve sharp delineations of organs in coronal reformations. Information on 1.5T with DL may be competitive to those previously obtained on 3T systems. Using both1.5T and 3T systems in imaging suites, expected equal performance of both MR systems can give great advantages for patient-throughputs. Efficient investment might be made with keeping 1.5T systems with DL instead of renewing 3T systems. Limitations: Study population was limited. further studies in larger population should be performed.Conclusion
Application of DL on 1.5T can improve IQ and recognitions of soft tissues and vasculatures, which may be competitive to those on 3T without DL.Acknowledgements
No acknowledgement found.References
1)Saleh M. et al. J Comput Assist Tomogr 2023 47 721Figures
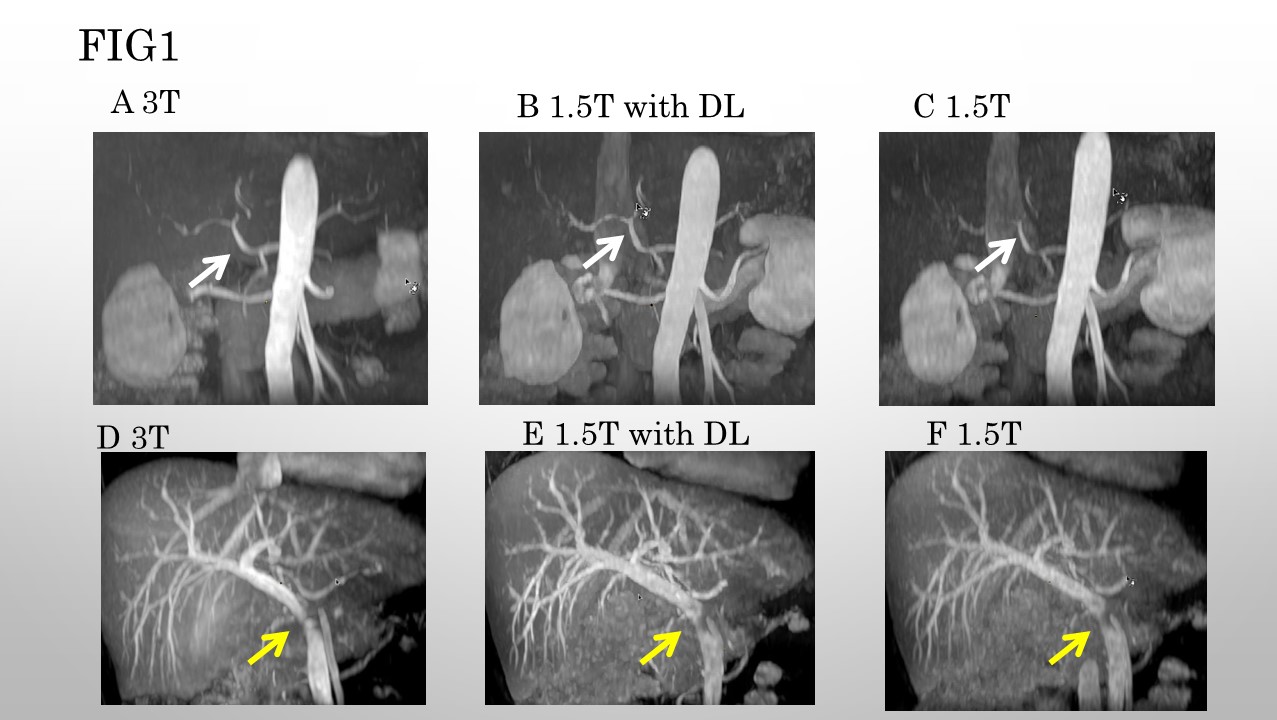
FIG 1 S/P Resection of the pancreatic tumor in the tail. 70ys Male.
A, B, C: MIP images in the arterial phase. The celiac axis and its branches (white arrow) are well delineated on 1.5T with DL which, are compatible to those on 3T.
D, E, F: MIP images in the portal phase. Narrowing of the portal vein is noted (yellow arrow). The intrahepatic branches of the portal vein are better demarcated with sharp margins on 1.5T with DL. DL improves overall image quality with sharp delineation of the edges of the structures. DL indicates deep learning reconstruction.
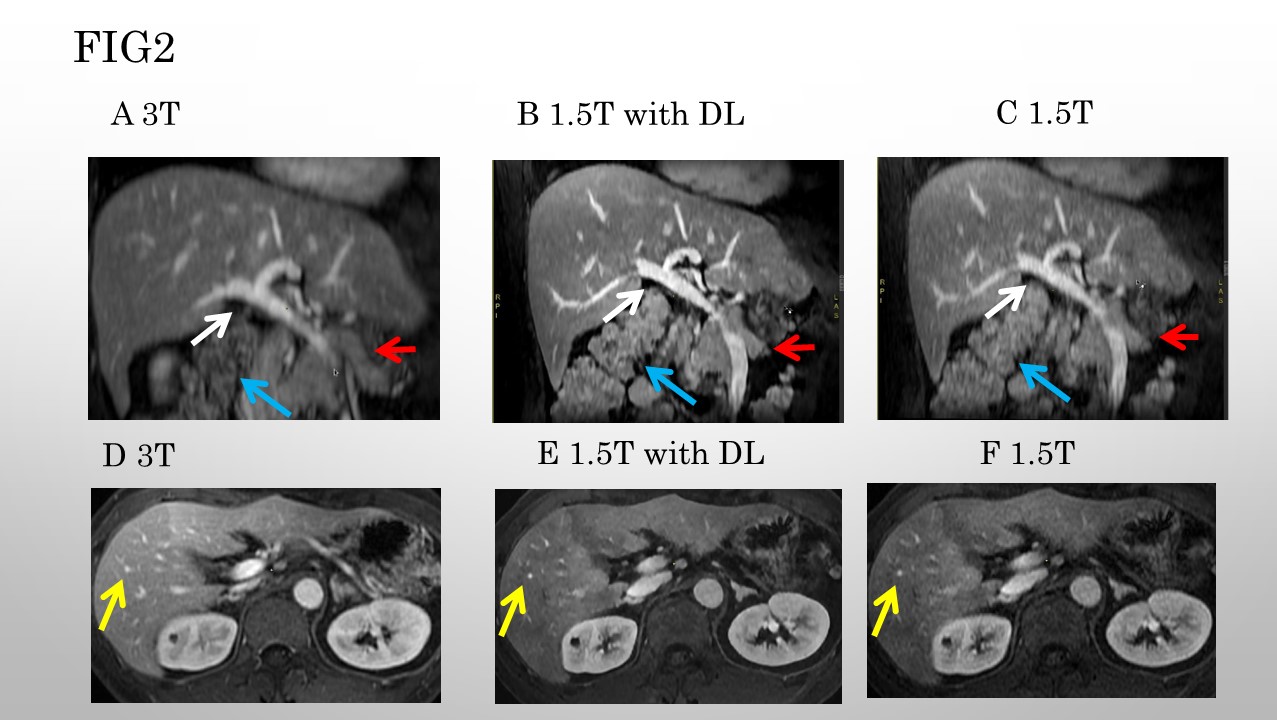
FIG 2 S/P Resection of the pancreatic tumor in the tail. 70ys Male.
A, B, C: Oblique coronal images in the portal phase. The portal vein (white arrows), its branches, arteries, other organs such as the pancreas (red arrows) and intestines (blue arrows) are sharply demarcated on 1.5T with DL. Blurring of the edges are noted on images on 3T and 1.5T without DL. D, E, F: Transverse images in the portal phase. Edges of the soft tissues and intrahepatic vasculatures (yellow arrows) are sharply delineated on 1.5T with DL although on images with 3T and 1.5T, blurring is noted.
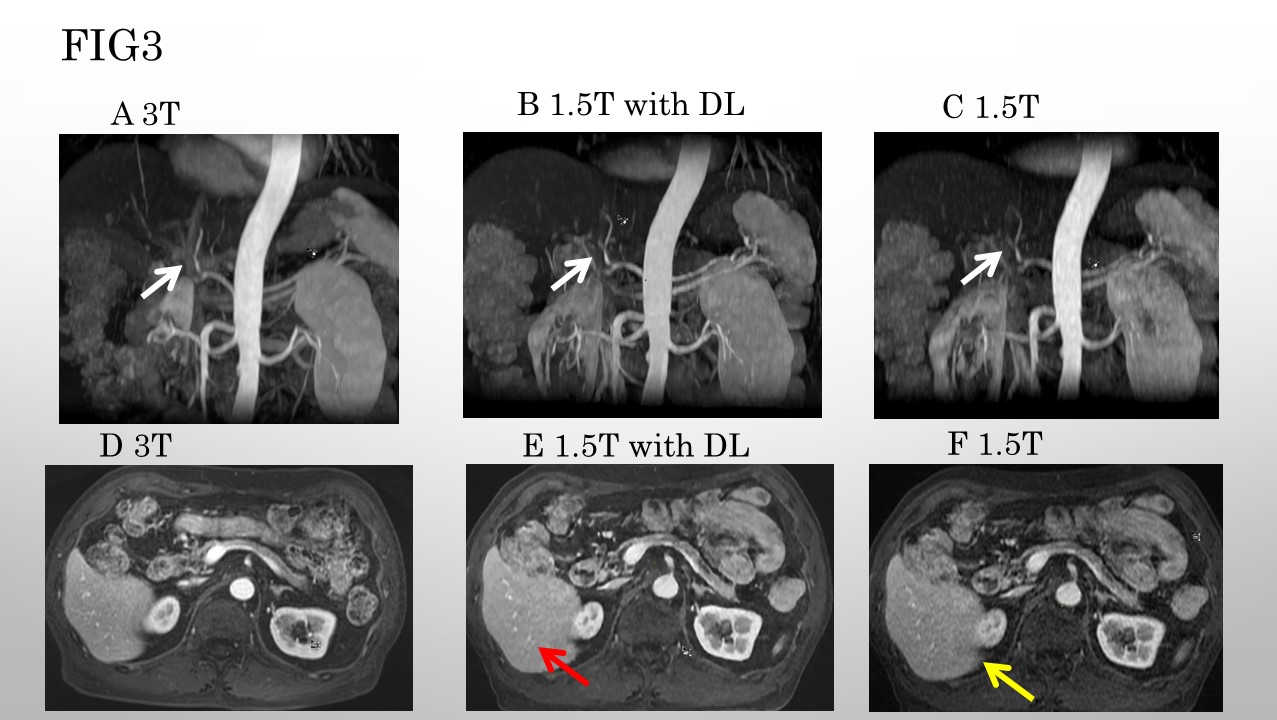
FIG3. Autoimmune pancreatitis. 50ys Male.
A, B, C: MIP images in the arterial phase. The celiac axis and its branches (white arrow) are well delineated on 1.5T with DL, which are compatible to those on 3T.
D, E, F: Transverse images in the poral phase. On the image on 1.5T with DL, sharp delineation of the edges of the organs and intra hepatic vasculatures (red arrow on E) are recognized. Noise (yellow arrow on F) is noted on 1.5T without DL.