4152
Phase contrast magnetic resonance imaging for diagnosis of inferior vena cava obstruction in Budd-Chiari syndrome1Radiology, Affiliated Hospital of Xuzhou Medical University, Xuzhou, China, 2CT and MRI, Xuzhou Central Hospital, Xuzhou, China
Synopsis
Keywords: Liver, Vessels, Budd-Chiari syndrome; inferior vena cava; phase contrast
Motivation: It is critical to determine whether the inferior vena cava (IVC) is occluded in Budd-Chiari syndrome (BCS) patients before interventional treatment. Magnetic resonance venography (MRV) has high sensitivity, but the specificity needs to be further improved.
Goal(s): This prospective study aims to compare the accuracy of IVC occlusion assessment using phase contrast MRI (PC-MRI) and MRV.
Approach: The Kappa coefficient test was used to evaluate the agreement, using digital subtraction angiography (DSA) as the gold standard.
Results: Intergroup agreement was excellent between PC-MR and DSA (κ=0.904), which was higher than that between MRV and DSA (κ=0.716).
Impact: Our results suggest that PC-MR is a more accurate method for assessing IVC obstruction. However, reproducibility tests still need to be performed. In addition, the hepatic vein was not evaluated, which could be investigated in future studies.
Introduction
Primary Budd-Chiari syndrome (BCS) is a rare disorder caused by occlusion or stenosis of the hepatic vein and/or the inferior vena cava (IVC)1. It is important to determine whether the IVC is only stenosis or total occlusion for the choice of interventional therapy2. A previous study showed that MRV has a high sensitivity in assessing IVC occlusion, but its specificity requires further improvement3. In recent years, phase contrast MRI (PC-MRI) has been used in IVC evaluation4. The purpose of this study was to assess the feasibility of PC-MRI in evaluating IVC occlusion compared to MRV using digital subtraction angiography (DSA) as the gold standard.Methods
This prospective clinical study was approved by the local Institution Review Board and written informed consent was obtained from all patients. Between October 2017 and December 2019, 72 consecutive IVC-related BCS patients confirmed by computed tomography or ultrasonography were included in this study. All patients underwent scanning with a 3.0T MR scanner (Philips Ingenia, Netherlands). For PC-MRI, a cine PC-based fast Q-flow sequence was performed. Sagittal and coronal planes of IVC were obtained. Peripheral gating was used to acquire the signal. A group of sequences contains 30 frames of images, including 2 sets (anatomical and phase map). PC-MRI parameters: matrix size = 300 × 248, slice thickness = 8 mm, TR/TE = 3.1ms/4.7ms, NSA = 1, flow rate coded 50 cm/s. The scanning time was 15-25 s. MRV parameters: 3D mode. FOV = 40 cm, matrix size = 268 × 248, TR/TE = 3.6ms/1.32ms, NSA = 1. Gd-DTPA (0.1 mmol/kg) was injected intravenously at a flow rate of 3.0 ml/s with a high-pressure syringe (Ulrich, Germany), followed by administration of 20 ml of isotonic saline. Axial, coronal, and sagittal images of IVC were separately acquired after contrast injection (55, 90, and 180 seconds after injection). MRV scans were performed with breath-holding. All image analyses were performed as follows: PC-MRI images were imported into Philips’ postprocessing software package (Q-flow). The system automatically generates the phase map related to one cardiac cycle with overlaid pseudo-color. The image quality of PC-MRI was assessed via a five-point scale by two radiologists (with 12 and 10 years of experience) separately for each patient4. The diagnosis of IVC occlusion with PC-MRI and MRV was separately analyzed by the same two radiologists who were blinded to DSA results. To avoid interference, there was a one-month interval between PC-MRI and MRV analysis. DSA was performed as a gold standard within one week of the MRI exam. All statistical analyses were performed using MedCalc Software (version 18.2). Interobserver agreement for PC-MR image quality and IVC obstruction assessment between the two readers were all determined by calculating the κ values using a kappa test. Intergroup agreement for the detection of IVC obstruction between two methods (MRV vs. DSA, PC-MRI (Reader 1) vs. DSA) was determined by calculating the κ values using a kappa test. A κ value between 0.61 to 0.8 indicates good agreement and above 0.81 indicates excellent agreement. Diagnostic accuracy was assessed by measuring sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).Results
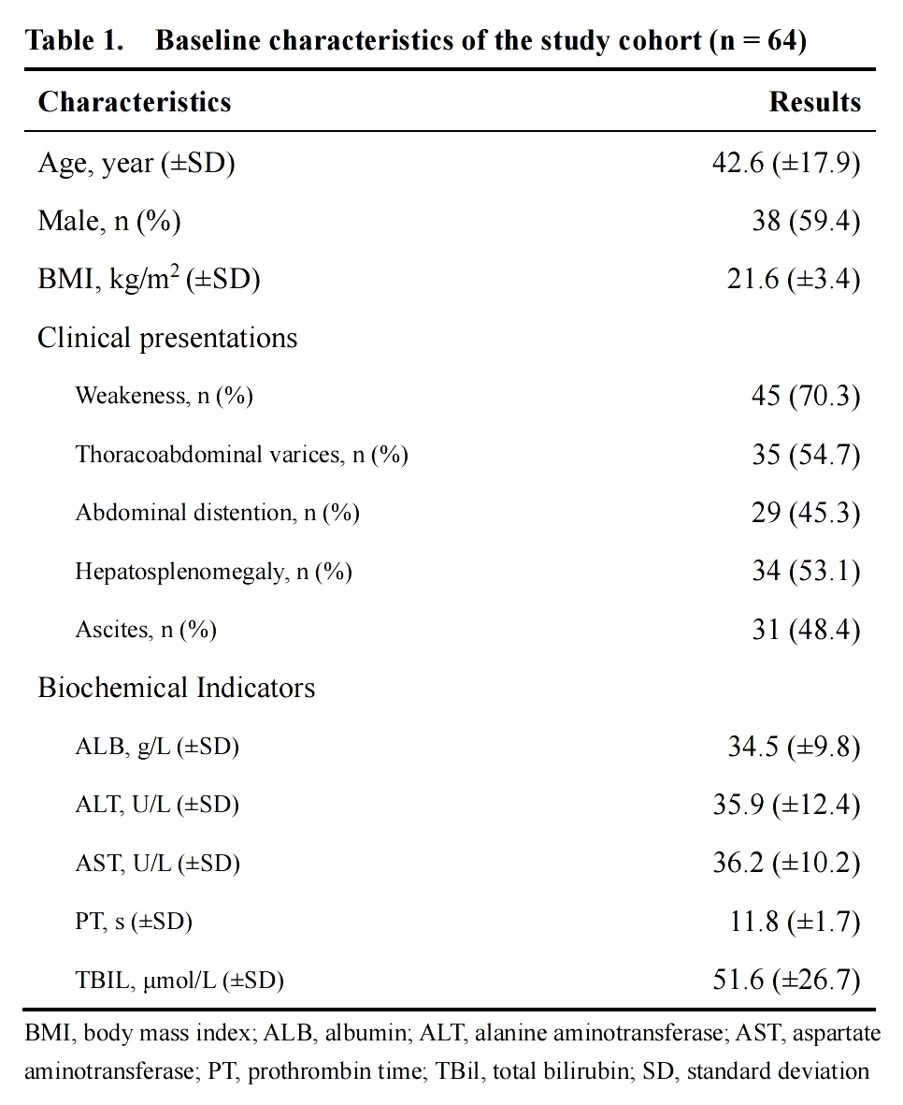
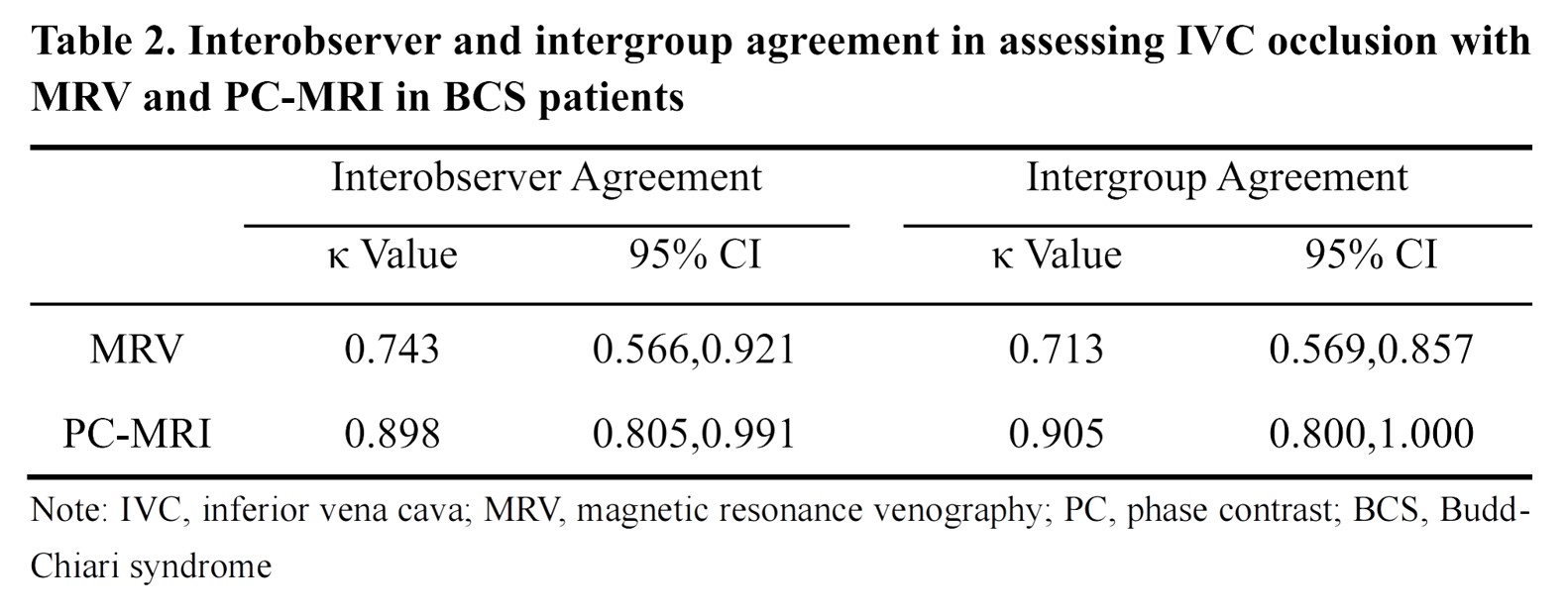
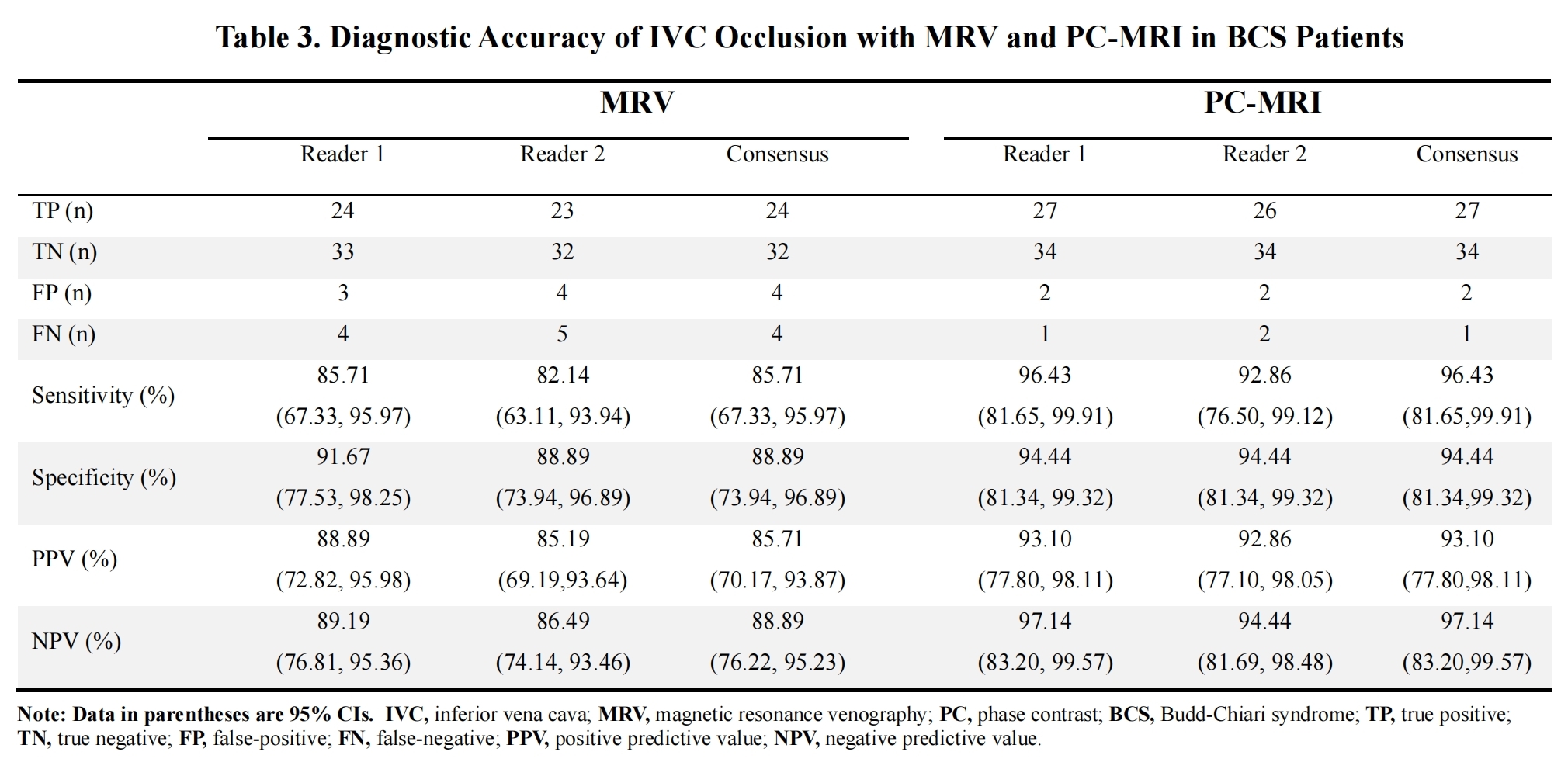
PC-MR image acquisition was successful in 64 patients (score ≥2). Interobserver agreement for image quality was excellent (κ=0.904). Demographic information relevant to patients is presented in Table 1. Among them, 28 cases were confirmed to have IVC occlusion. Interobserver agreement between the 2 readers was excellent in MRV (κ=0.935) and PC-MRI (κ=0.968) for the detection of IVC obstruction. Intergroup agreement was good between MRV and DSA (κ=0.716), and excellent between PC-MR and DSA (κ=0.904) (Table 2) (Figure 1 and Figure 2). The sensitivity, specificity, PPV, and NPV of MRV for the detection of IVC obstruction were 85.71%, 88.89%, 85.71%, and 88.89%, respectively. For the PC-MRI group, they were 96.43%, 94.44%, 93.10%, and 97.14%, respectively (Table 3).Discussion
In our study, for the first time, we evaluated IVC obstruction in BCS patients by qualitative PC-MR. Our findings suggest a more accurate method for assessing IVC obstruction. However, although PC-MR has more advantages than MRV in assessing IVC obstruction, we strongly recommend that MRV should be performed conventionally before interventional treatment. Because, MRV could provide some additional useful information, such as collateral circulation, accessory hepatic veins, regenerative nodules, venous thrombosis, etc5.Conclusion
PC-MRI has higher diagnostic efficiency than MRV in evaluating IVC obstruction in BCS patients, which can be used as an important supplementary assessment method for pre-interventional therapy.Acknowledgements
No acknowledgement found.References
1. Bansal V, Gupta P, Sinha S, et al. Budd-Chiari syndrome: imaging review. Br J Radiol. 2018; 91:20180441.
2. Huang Q, Shen B, Zhang Q, et al. Comparison of long-term outcomes of endovascular management for membranous and segmental inferior vena cava obstruction in patients with primary Budd-Chiari syndrome. Circ Cardiovasc Interv. 2016 Mar;9(3): e003104.
3. Lu X, Xu K, Zhang Q, et al. Study on between magnetic resonance venography and digital subtraction angiography on the inferior vena cava obstructive interface morphology of Budd-Chiari syndrome. Chin J Hepatol. 2011;19: 923-926.
4. Lu X, Ma X, Xu K, et al. Inferior vena cava obstruction in Budd-Chiari syndrome: a comparative study of rapid quantitative phase-contrast MRI and MRV. Abdom Radiol (NY). 2020; 45:1069-1074.
5. Shukla A, Shreshtha A, Mukund A, et al. Budd-Chiari syndrome: consensus guidance of the Asian Pacific Association for the study of the liver (APASL). Hepatol Int. 2021; 15:531-567.
Figures
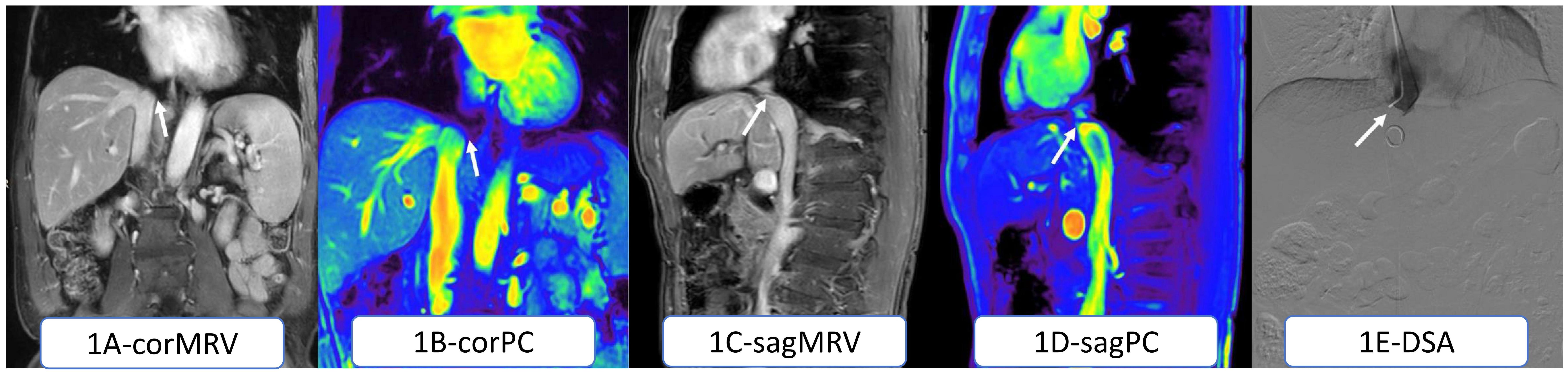
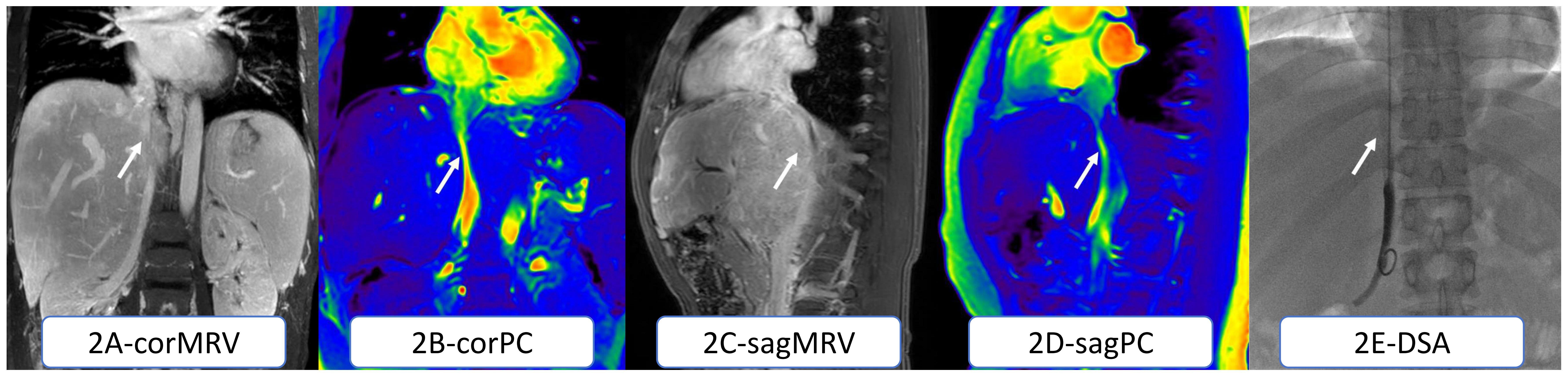
Figure 2. BCS with IVC segmental stenosis in a 27-year-old man. Coronal (a) and sagittal (c) MRV images were in a dilemma to judge IVC obstruction. Coronal (b) and sagittal (d) PC-MRI showing IVC stenosis, which was confirmed by DSA (e).