4151
Abbreviated MRI as Frontline Screening for Metabolic Dysfunction-Associated Steatohepatitis (MASH) in Obese Patients with BMI > 321Radiology, Stanford University, Palo Alto, CA, United States, 2Radiology, VA Palo Alto, Palo Alto, CA, United States, 3Siemens Healthineers, Malvern, PA, United States, 4Hepatology, VA Palo Alto, Palo Alto, CA, United States, 5Gastroenterology / Hepatology, Stanford University, Palo Alto, CA, United States
Synopsis
Keywords: Liver, Liver, Obesity, Metabolic dysfunction-associated steatohepatitis (MASH), Metabolic dysfunction-associated steatotic liver disease (MASLD), vibration-controlled transient elastography (VCTE)
Motivation: Metabolic dysfunction-associated steatohepatitis (MASH) represents a growing pandemic with obese patients at higher risk. However, obesity limits vibration-controlled transient elastography (VCTE) in frontline screening.
Goal(s): We aimed to compare the effect of body mass index (BMI) on diagnostic performance of VCTE and abbreviated MRI.
Approach: Patients (N=229) were enrolled into a prospective study with VCTE and a subset (N=59) underwent same-day abbreviated MRI.
Results: Patients with BMI > 32 had a higher failure rate of VCTE at 33%, but MRI was diagnostic in all patients. Obese patients with BMI > 32 benefit from proceeding directly to MRI for hepatic evaluation.
Impact: Obesity correlates with higher liver fibrosis in metabolic dysfunction-associated steatohepatitis (MASH), but also increases failure of vibration-controlled transient elastography (VCTE) in frontline screening. Abbreviated MRI should be considered a frontline screening modality in obese patients with BMI >32.
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) afflicts over 25% of the global population, many are undiagnosed until advanced stages of disease.1 Approximately 21% of MASLD patients progress to metabolic dysfunction-associated steatohepatitis (MASH),2 a leading cause of cirrhosis and hepatocellular carcinoma. Effective screening for at risk individuals is a pressing clinical need.Obese patients are up to 14-fold higher risk for MASLD/MASH.3,4 Paradoxically, however, the current frontline screening tool, vibration-controlled transient elastography (VCTE),5 is frequently non-diagnostic in obese patients. Advances in MRI sequences enable rapid abbreviated MRI exams to answer focused clinical questions without being limited by obesity, opening the door for using same-day abbreviated MRI as a frontline screening tool. We aim to determine an optimal BMI threshold for triaging patients directly to abbreviated MRI as a frontline screening tool for MASH.
Methods
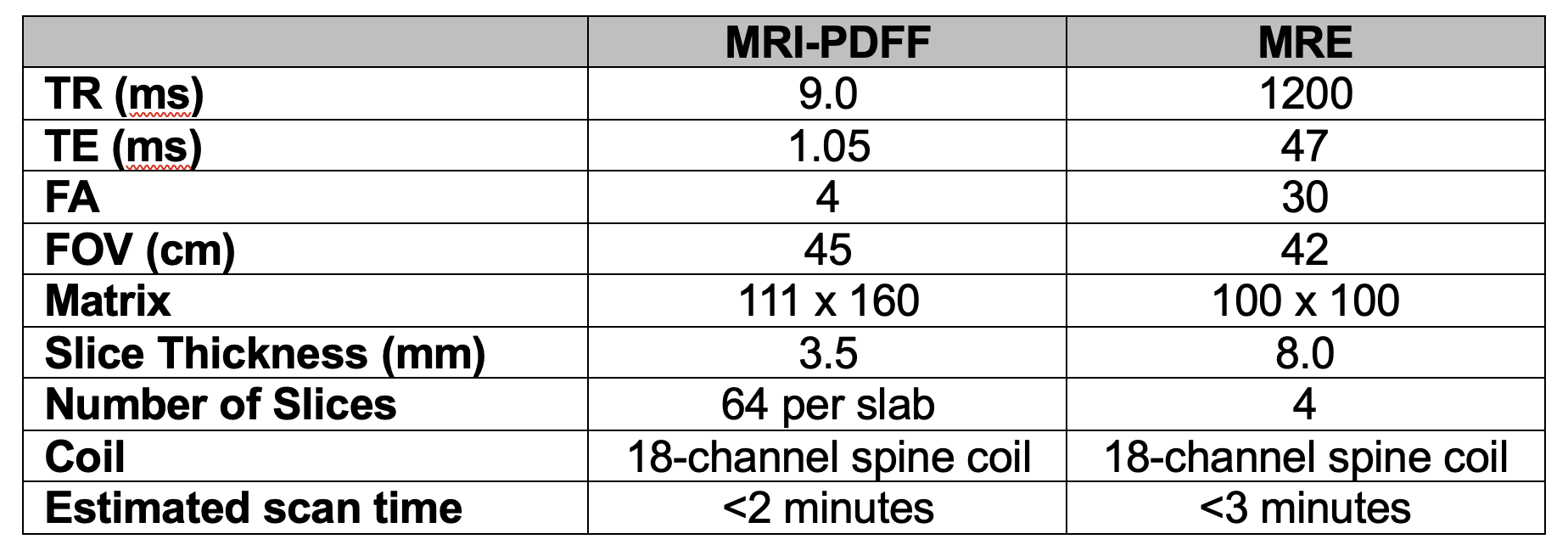
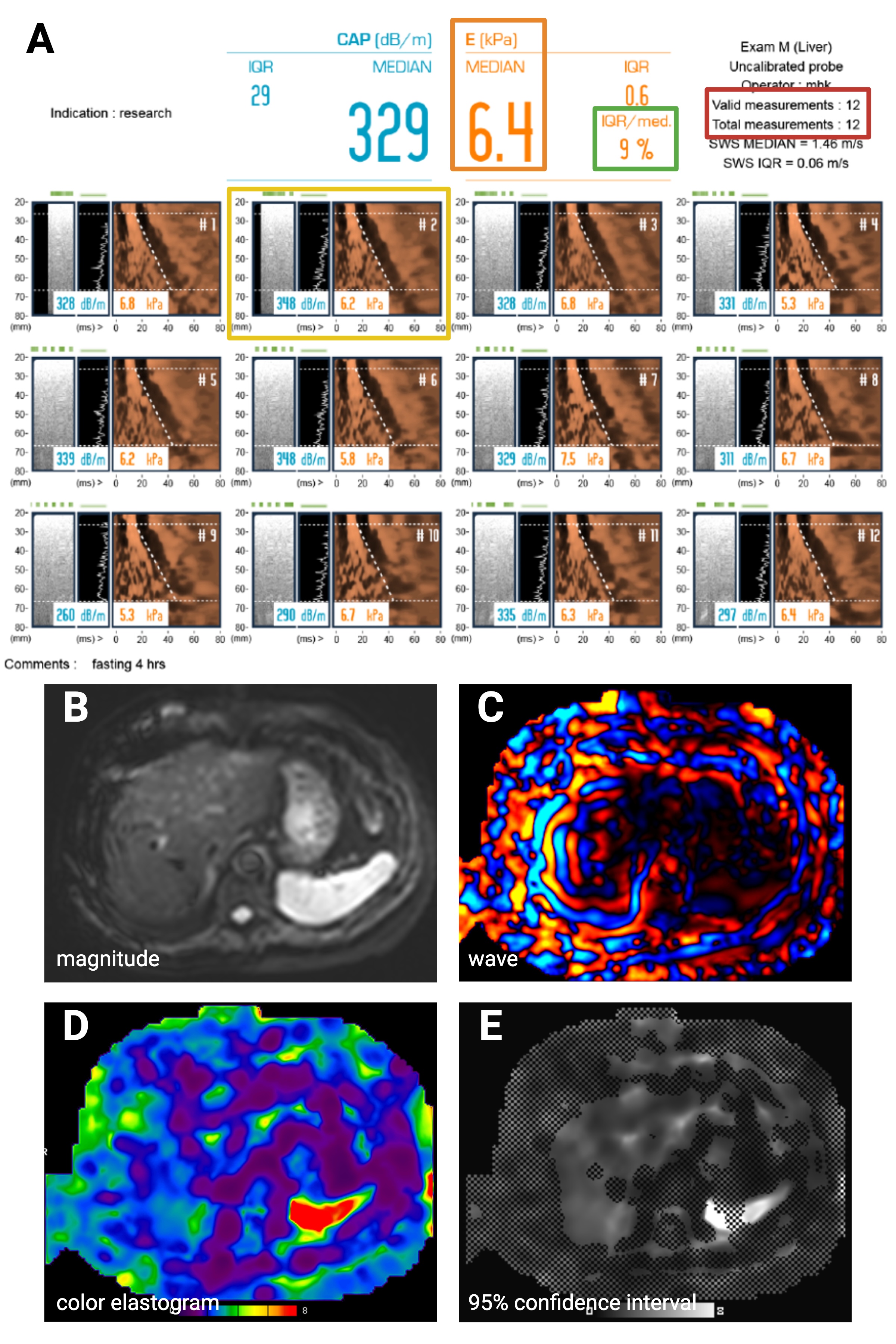
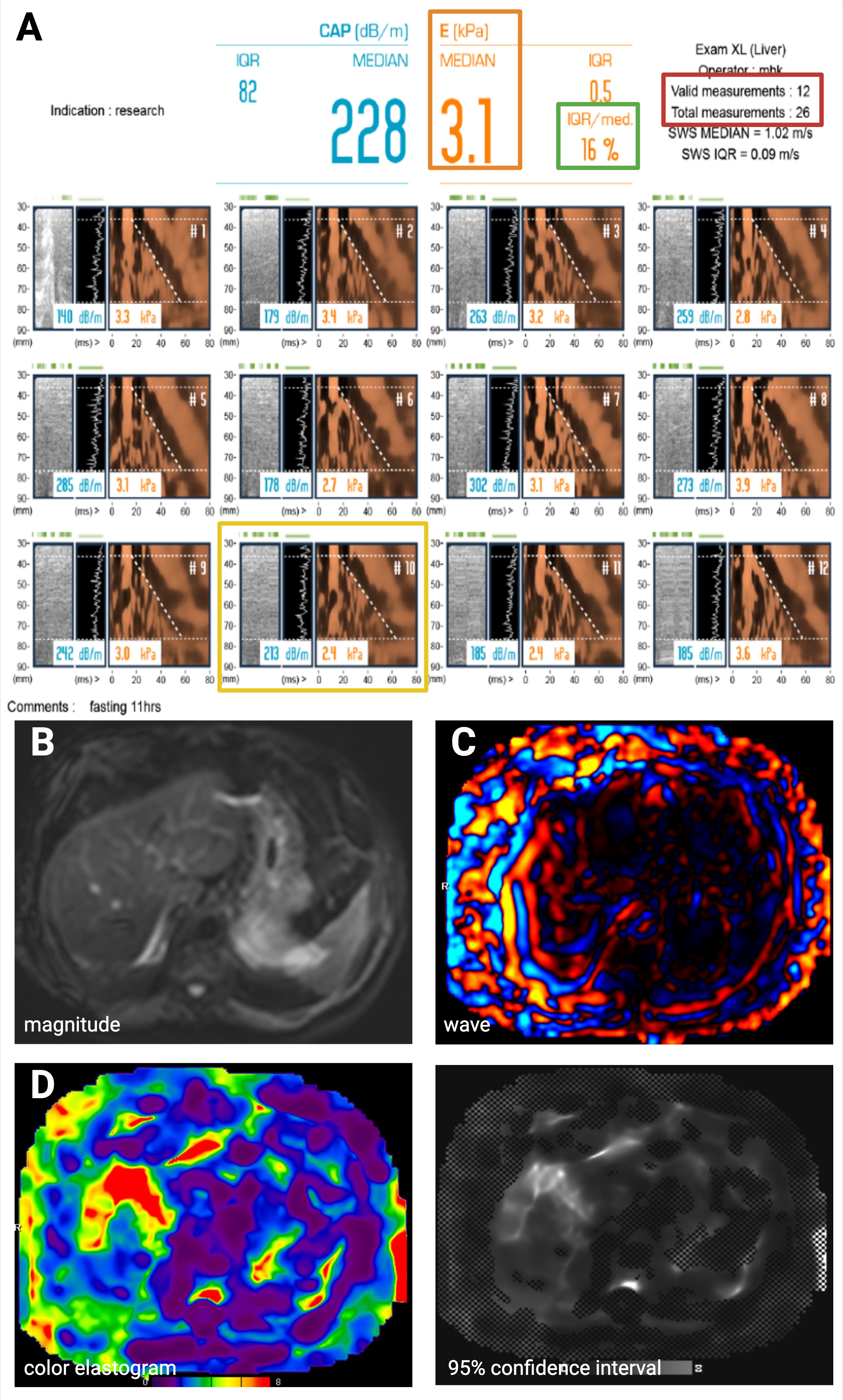
We enrolled patients (N=229) from the Veterans Affairs (VA) Hospital in Palo Alto, California, USA, with risk factors for MASLD/MASH (type 2 diabetes and/or obesity with BMI >30) between 2022-2023 in a prospective screening study with VCTE. A subset of patients (N=59) underwent same-day abbreviated MRI. Abbreviated MRI included localizer, magnetic resonance elastography (MRE), and fat/iron quantification with MRI proton density fat fraction (MRI-PDFF) performed on a 3T scanner (Siemens Skyra/Vida Fit) (Table 1) with a median MRI setup and scan time of 12 minutes (range 8-30 min). MRI time of 30 minutes was due to technical failure of MRI scanner requiring reboot. Non-diagnostic VCTE was defined as failure to obtain any measurements or failure of at least 1 of 3 standard criteria (>=10 valid measurements, >60% valid total measurements, or interquartile range (IQR/median) <30%).5 Non-parametric Wilcoxon Rank-Sum tests were performed to compare clinical characteristics between patients with diagnostic versus non-diagnostic VCTE. Youden index analysis was performed to determine an optimal BMI cutoff for non-diagnostic VCTE.Results
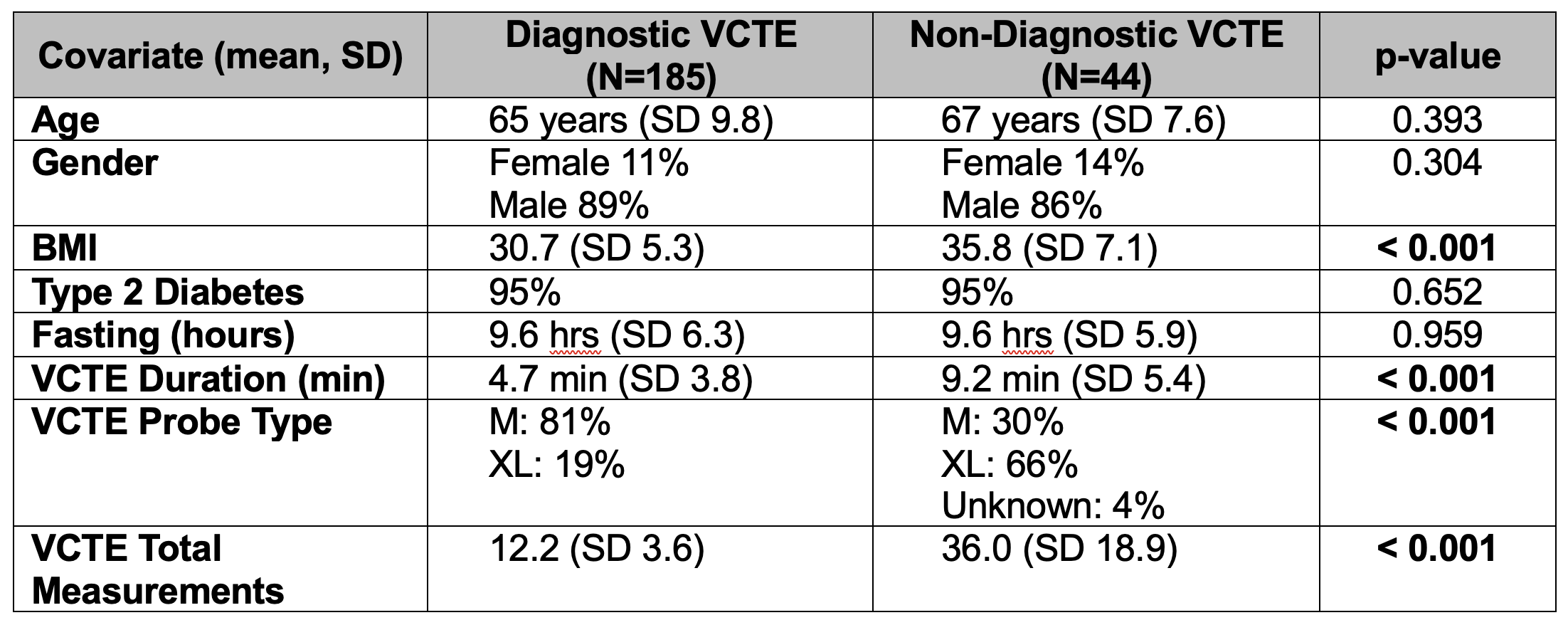
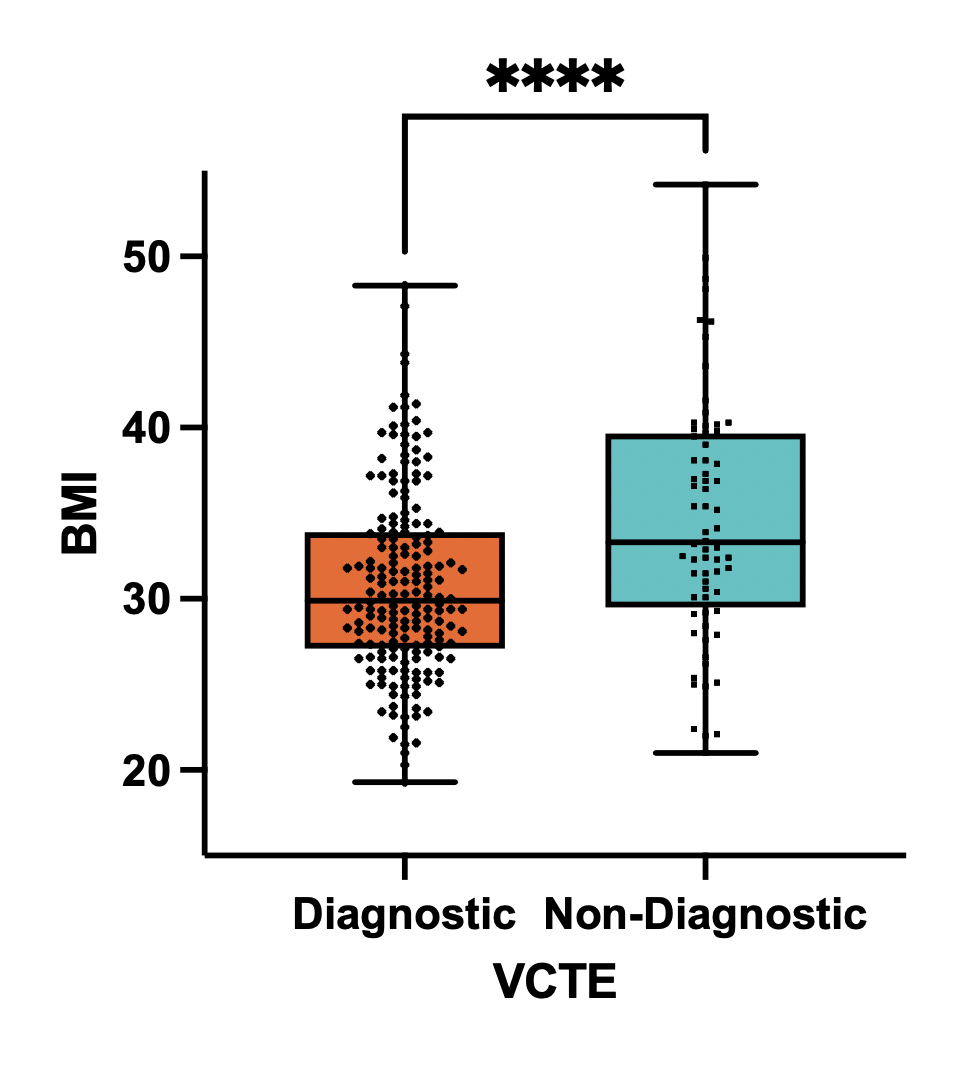
Out of 229 veterans enrolled (median age 68 years, range 34-76 years), 87% were male and 96% had type 2 diabetes. Median BMI was 31 (range 19-54). VCTE was non-diagnostic for 44/229 patients (19%). Patients with non-diagnostic VCTE had significantly higher mean BMI of 36 compared to patients with diagnostic VCTE and mean BMI of 31 (p<0.0001) (Table 2, Figure 1). Using the Youden criteria to maximize the combination of sensitivity and specificity of VCTE (rates of diagnostic vs. non-diagnostic VCTE at varying BMI thresholds), a threshold BMI > 32 resulted in a higher failure rate for VCTE at 33% (p < 0.001). MRE was diagnostic in all subjects. Among 44 patients with non-diagnostic VCTE, 10 patients selected on the basis of laboratory-based Fibrosis-4 (FIB-4) Index results underwent successful same-day MRE with values ranging from 1.84 to 4.35 kPa (median 2.42 kPa), including one patient with Stage 3 advanced fibrosis (4.35 kPa) diagnosed by MRE. Same-day abbreviated MRE obviates the need for a second visit and reduces time to diagnosis. Eliminating need for a second visit is significant because VA patients can travel long distances to clinic. We also observed a significant relationship between higher BMI and higher stages of liver fibrosis based on VCTE and MRE. Specifically, for each unit value increase in BMI, there is an associated 1.47% increase in MRE (kPa) (CI 0.42-2.52%, p = 0.0070).Discussion
Among a selected higher risk population for MASLD/MASH, we have previously shown that MRE is more cost effective than VCTE for diagnosis.6 Obesity represents a significant risk factor for MASLD/MASH, yet also lowers the likelihood of obtaining diagnostic screening VCTE results5 with a 33% failure rate among patients with BMI > 32. Critically, we observed a significant relationship between higher BMI and higher stages of fibrosis,7 which underscores how individuals with a greater likelihood of liver fibrosis remain undetected by VCTE. Implementation of an abbreviated MRI protocol enabled same-day MRI screening using <15 minutes of total time. Faster exam times and the known higher diagnostic accuracy of MRE8 compared to VCTE makes same-day abbreviated MRI a realistic screening tool. We found that BMI > 32 may represent an optimal threshold for consideration of abbreviated MRI as a frontline screening tool for MASH. We plan to develop future cost effectiveness modeling to evaluate whether patients with BMI > 32 would benefit from frontline abbreviated MRI rather than VCTE screening for MASH.Conclusion
Abbreviated MRI exams enable rapid (< 15 minutes) and cost effective diagnosis of MAFLD/MASH. Obese patients with BMI > 32 at risk for MASH/MAFLD may benefit from directly proceeding to abbreviated MRI given the high likelihood of non-diagnostic VCTE in these individuals.Acknowledgements
This project was supported in part by Siemens Healthineers.References
1. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatol Baltim Md. 2016;64(1):73-84. doi:10.1002/hep.284312.
2. Loomba R, Adams LA. The 20% Rule of NASH Progression: The Natural History of Advanced Fibrosis and Cirrhosis Caused by NASH. Hepatol Baltim Md. 2019;70(6):1885-1888. doi:10.1002/hep.309463.
3. Hamid O, Eltelbany A, Mohammed A, Alsabbagh Alchirazi K, Trakroo S, Asaad I. The epidemiology of non-alcoholic steatohepatitis (NASH) in the United States between 2010-2020: a population-based study. Ann Hepatol. 2022;27(5):100727. doi:10.1016/j.aohep.2022.1007274.
4. Loomis AK, Kabadi S, Preiss D, et al. Body Mass Index and Risk of Nonalcoholic Fatty Liver Disease: Two Electronic Health Record Prospective Studies. J Clin Endocrinol Metab. 2016;101(3):945-952. doi:10.1210/jc.2015-34445.
5. Castéra L, Foucher J, Bernard PH, et al. Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatol Baltim Md. 2010;51(3):828-835. doi:10.1002/hep.234256.
6. Sangha K, Chang ST, Cheung R, Deshpande VS. Cost-effectiveness of MRE versus VCTE in staging fibrosis for nonalcoholic fatty liver disease (NAFLD) patients with advanced fibrosis. Hepatol Baltim Md. 2023;77(5):1702-1711. doi:10.1097/HEP.00000000000002627.
7. Ajmera V, Cepin S, Tesfai K, et al. A prospective study on the prevalence of NAFLD, advanced fibrosis, cirrhosis and hepatocellular carcinoma in people with type 2 diabetes. J Hepatol. 2023;78(3):471-478. doi:10.1016/j.jhep.2022.11.0108.
8. Selvaraj EA, Mózes FE, Jayaswal ANA, et al. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: A systematic review and meta-analysis. J Hepatol. 2021;75(4):770-785. doi:10.1016/j.jhep.2021.04.044
Figures