4146
Risk prediction and postoperative recurrence of Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma based on LI-RADS v20181Nantong Third People's Hospital, Nantong, China, 2Philips Healthcare, Shanghai, China
Synopsis
Keywords: Liver, Liver, HCC, MTM-HCC
Motivation: Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma (MTM-HCC) has been confirmed to possess higher invasiveness and malignancy.
Goal(s): This study aims to compare the clinical parameters and imaging characteristics between MTM-HCC and non-MTM-HCC patients, construct a predictive model for the MTM-HCC subtype, and evaluate the model's value in risk stratification.
Approach: This study is a retrospective research.
Results: The ≥ 50% AP hypovascular component and peritumoral hypointensity on HBP images are independent predictive factors for diagnosing MTM-HCC, and the predictive model exhibits a significant difference in overall recurrence-free survival (RFS) and early recurrence (P < 0.05).
Impact: This study, based on the significant imaging features of LI-RADS v2018 and other imaging signs, offers clinical value for the diagnosis and prognosis prediction of the MTM-HCC pathological subtype, providing new insights for the personalized treatment of HCC patients.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignant tumor of the liver. In the 2019 WHO classification of digestive system tumors, eight distinct histological subtypes of HCC were identified, among which the MTM-HCC stands out for its higher invasiveness and malignancy compared to more common HCC subtypes. Identifying this aggressive subtype holds promise for personalized treatment and prognosis prediction. Imaging features has been proven to be a particularly useful non-invasive method for diagnosing and characterizing HCC. The Liver Imaging Reporting and Data System (LI-RADS) provides standardized imaging criteria for the diagnosis of HCC and the assessment of treatment responses. However, only a few studies have used LI-RADS for the diagnosis of MTM-HCC, and none have investigated its prognosis. Therefore, this study aims to establish an MTM-HCC predictive model based on important imaging features from LI-RADS v2018 and other criteria, and to assess its predictive value for prognosis.Methods
This study included 236 patients with HCC, including 50 MTM-HCC and 186 non-MTM-HCC, all of whom underwent preoperative MRI and received pathologic confirmation between April 2015 and January 2022. Preoperative clinical parameters and MRI imaging features of all patients were analyzed. Univariate and multivariate logistic regression were used to select independent predictive factors for MTM-HCC, and then construct a predictive model. The model's efficacy was assessed using Receiver Operating Characteristic (ROC) curve analysis, and the differences in the Area Under the Curve (AUC) were compared using the DeLong test. The cut-off value, determined as the point with the maximum Youden Index, divided patients into high and low-risk subgroups. Kaplan-Meier analysis was used to compare overall RFS, early and late recurrence in the predictive model high-risk and low-risk groups and the pathologic MTM-HCC (+/-) group.Results
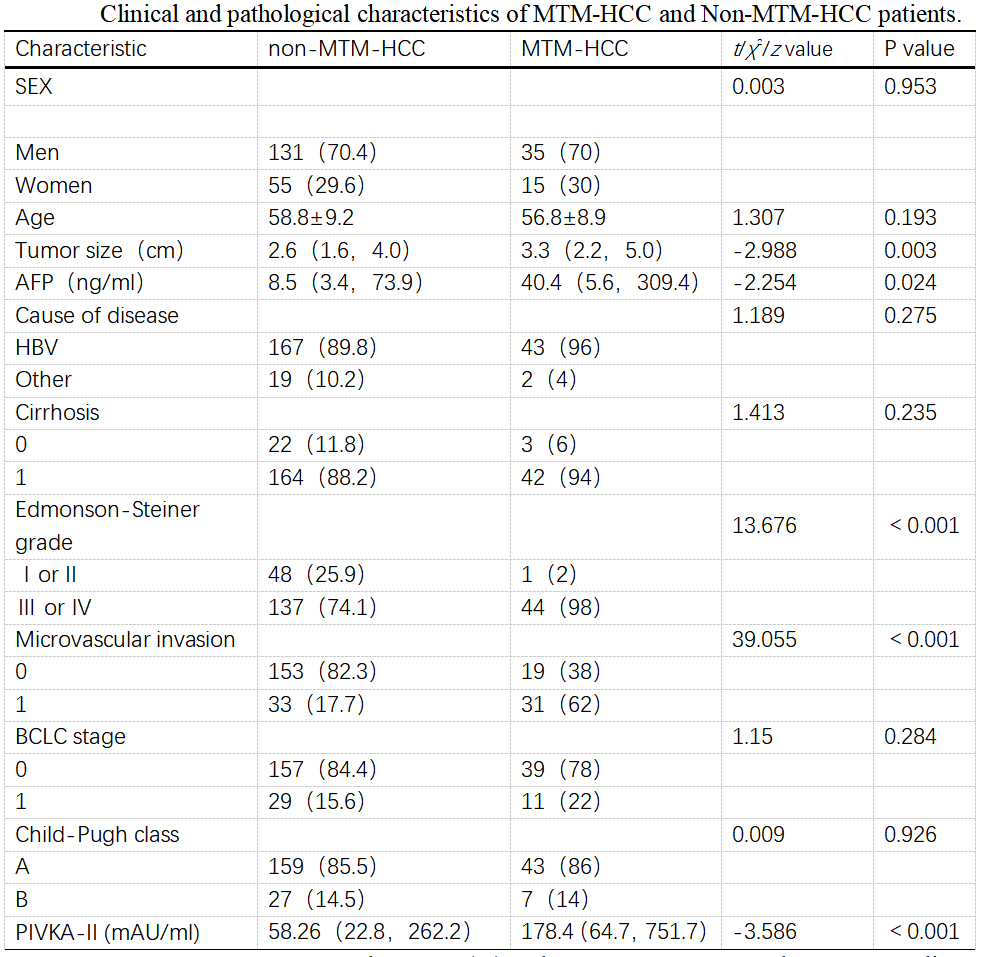
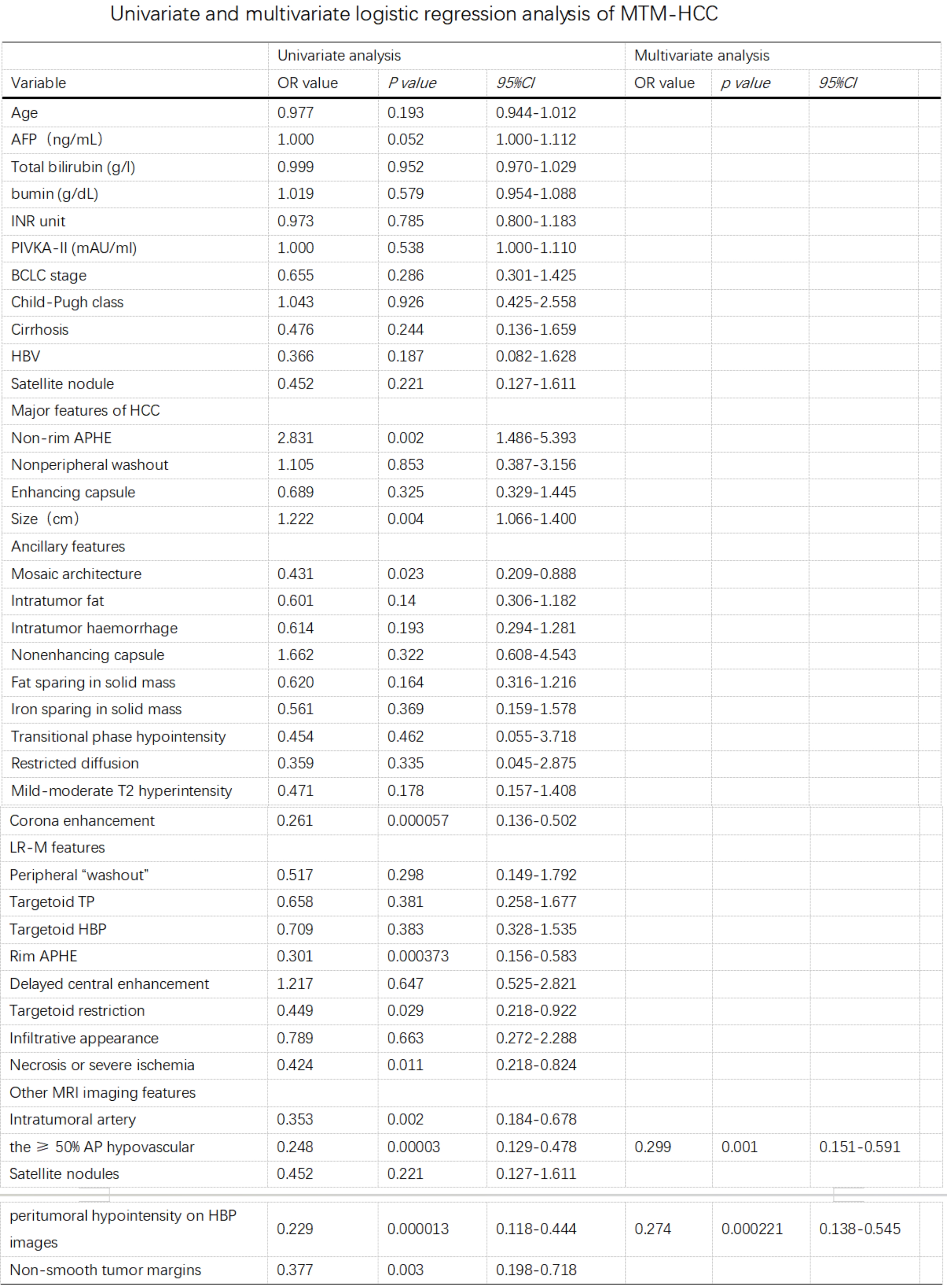
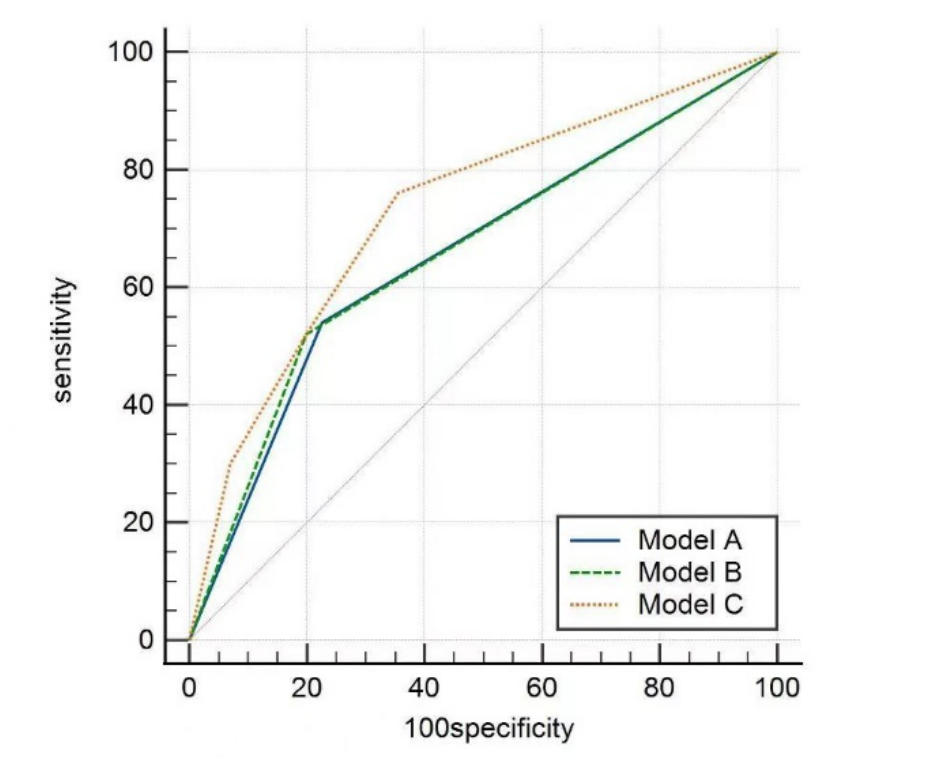
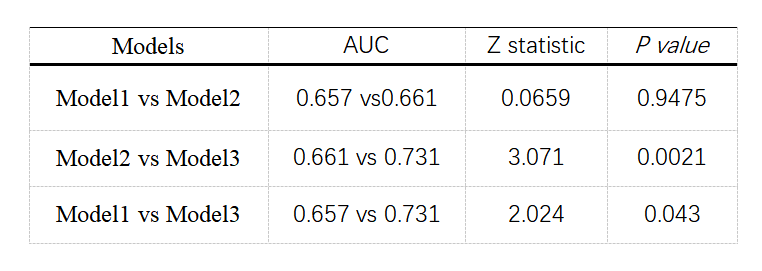
1.MTM-HCC was associated with elevated serum alpha-fetoprotein (AFP) levels (P=0.024), higher Edmonson-Steiner grading (P<0.001), larger tumor size (P=0.003), microvascular invasion (P<0.001), and increased abnormal prothrombin (P<0.001). There were no significant differences in other characteristics between MTM-HCC and non-MTM-HCC.2.Multivariable logistic regression analysis revealed that the ≥ 50% AP hypovascular component (P=0.001, OR=0.299) and peritumoral hypointensity on hepatobiliary phase (HBP) images (P<0.001, OR=0.274) were independent predictive factors for diagnosing MTM-HCC. The AUC, sensitivity, and specificity were 0.731 (95% CI 0.670 - 0.786, P<0.0001), 76%, and 65%, respectively. The DeLong test found that the combined diagnosis of the ≥ 50% AP hypovascular component and peritumoral hypointensity on HBP images had the highest diagnostic efficacy for MTM-HCC.
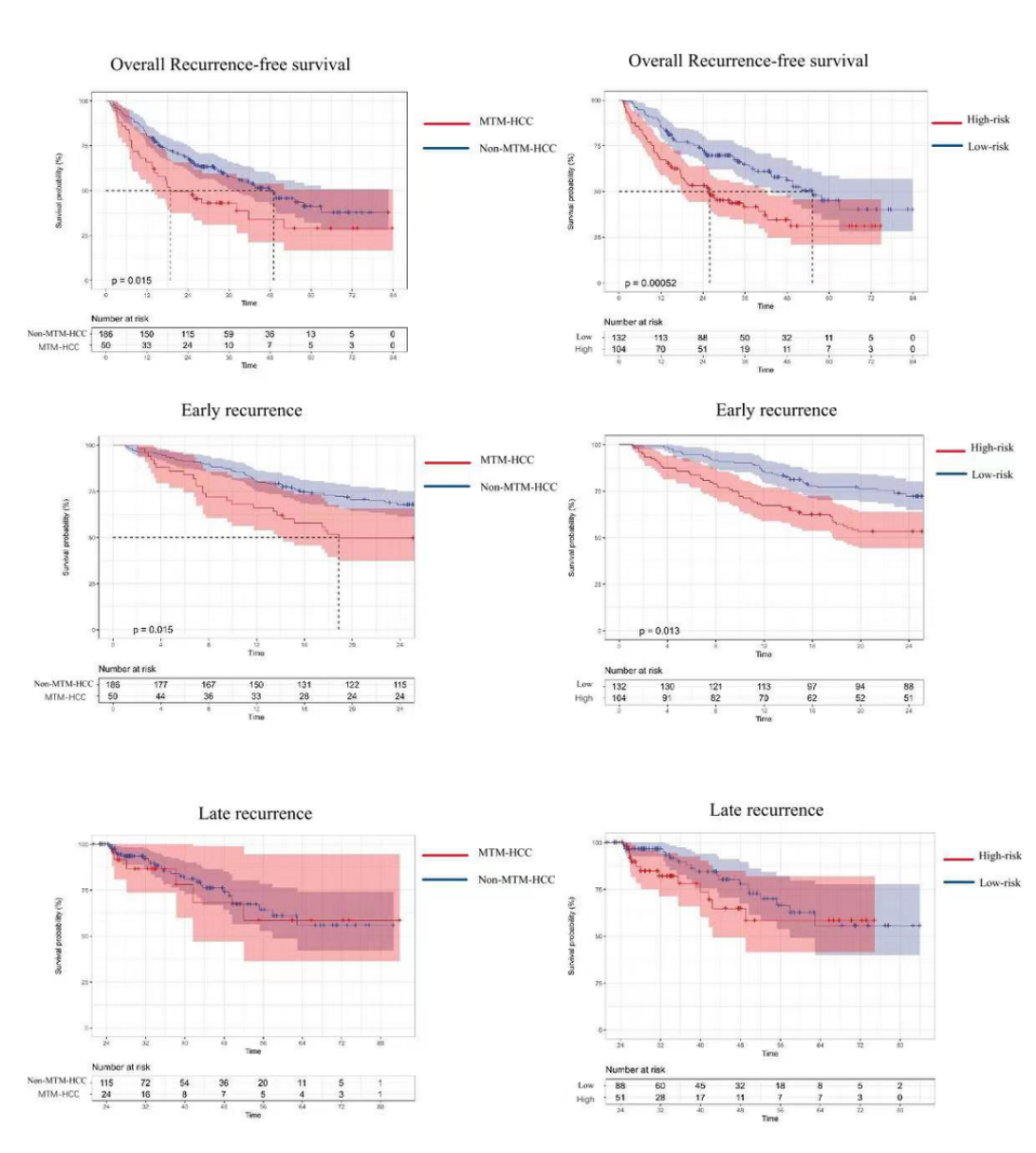
3.Kaplan-Meier survival analysis revealed that there were significant differences in the RFS and early recurrence between the high-risk and low-risk groups predicted by the MTM-HCC prognostic model and the pathologically confirmed MTM-HCC (+/-) groups (P<0.05), while there were no significant differences in late recurrence. This is consistent with the results obtained through pathological confirmation.
Discussion
Our study found that the ≥ 50% AP hypovascular component and peritumoral hypointensity on HBP images are independent predictive factors for diagnosing MTM-HCC. When combined, they can sensitively identify 76% of MTM-HCC cases with a specificity of 65%. Some researchers have investigated the performance of Gd-EOB-DTPA-enhanced MRI in characterizing MTM-HCC and discovered a strong correlation between the ≥ 50% AP hypovascular component and MTM-HCC. The sensitivity, specificity, and negative predictive value (NPV) for ≥20% hypovascular component were 88%, 57%, and 95%, respectively, and for ≥50% hypovascular component, the sensitivity, specificity, and NPV were 67%, 86%, and 92%, respectively. The mechanism behind this may be due to the presence of abundant coarse fibrous structures within the lesion, which slows down the inflow of contrast agent during the arterial phase, resulting in the manifestation of arterial phase hypoenhancement. Another study showed that peritumoral hypointensity on HBP images is associated with poor prognosis. The mechanism for this involves tumor invasion of peri-tumoral portal vein branches, leading to compensatory arterial blood supply in the tumor's vicinity. This, in turn, causes impaired uptake of contrast agents by normal liver cells around the tumor during the hepatobiliary phase, resulting in lower signal intensity. This provides robust support for the findings of our study. Additional studies have found that MTM-HCC is an independent risk factor for early recurrence. In our study, the risk score for MTM-HCC showed good predictive efficacy for postoperative recurrence of HCC, and there were significant differences in RFS and early recurrence between the high-risk and low-risk groups.Conclusion
The LI-RADS v2018 and other MRI features not only contribute to the preoperative diagnosis of MTM-HCC but also hold significant clinical significance in predicting the RFS and early recurrence in patients with HCC.Acknowledgements
No acknowledgement found.References
[1]Chen J, Xia C, Duan T, et al. Macrotrabecular-massive hepatocellular carcinoma: imaging identification and prediction based on gadoxetic acid-enhanced magnetic resonance imaging. Eur Radiol[J]. 2021 Oct, 31(10):7696-7704.
[2]Liang Y, Xu F, Wang Z, et al. A gadoxetic acid-enhanced MRI-based multivariable model using LI-RADS v2018 and other imaging features for preoperative prediction of macrotrabecular-massive hepatocellular carcinoma[J]. Eur J Radiol. 2022 Aug,153:110356.
[3]Rhee H, Cho ES, Nahm JH, et al. Gadoxetic acid-enhanced MRI of macrotrabecular-massive hepatocellular carcinoma and its prognostic implications[J]. J Hepatol. 2021 Jan,74(1):109-121.
[4]Ziol M, Poté N, Amaddeo G, et al. Macrotrabecular-massive hepatocellular carcinoma: A distinctive histological subtype with clinical relevance. Hepatology[J]. 2018 Jul,68(1):103-112.
[5] Mulé S, Serhal A, Pregliasco AG, et al. MRI features associated with HCC histologic subtypes: a western American and European bicenter study[J]. Eur Radiol. 2023 Feb,33(2):1342-1352.
[6]Liang Y, Xu F, Wang Z, et al. A gadoxetic acid-enhanced MRI-based multivariable model using LI-RADS v2018 and other imaging features for preoperative prediction of macrotrabecular-massive hepatocellular carcinoma[J]. Eur J Radiol. 2022 Aug,153:110356.
[7]Cha H, Choi JY, Park YN, et al. Comparison of imaging findings of macrotrabecular-massive hepatocellular carcinoma using CT and gadoxetic acid-enhanced MRI[J]. Eur Radiol. 2023 Feb,33(2):1364-1377.
Figures