4144
Multi-shot DWI has a high sensitivity in hepatic NET metastasis detection, outperforming multiplanar T2w imaging1Stanford University, Palo Alto, CA, United States, 2Radiology, Stanford University, Palo Alto, CA, United States
Synopsis
Keywords: Liver, Diffusion/other diffusion imaging techniques, oncologic imaging, rapid protocol, T2 weighted, neuroendocrine tumor, hepatic metastasis, multi-shot DWI, surveillance imaging, tumor assessment, Gadoxetate
Motivation: Liver metastasis detection without intravenous contrast has potential applications in MRI surveillance and whole-body imaging.
Goal(s): To compare multishot DWI (msDWI) and T2w imaging with fat suppression (T2w+FS) in detecting neuroendocrine tumor (NET) liver metastases.
Approach: We retrospectively determined the visibility of 114 lesions (35 patients) on msDWI and multiplanar T2w+FS. Sensitivities were calculated.
Results: msDWI outperforms T2w+FS, with sensitivity approaching 90% for lesions <=5mm.
Impact: HBP (Gadoxetate) imaging is the gold standard for detecting liver metastases, however rapid MRI without intravenous contrast is attractive from a cost and patient perspective. msDWI alone may prove sufficient for NET metastasis detection.
Motivation
MRI is valuable in cancer detection and staging but is widely considered time consuming and expensive, reducing clinical adoption compared to workhorse methods like CT scan. With increasing emphasis on patient access and cost containment, rapid MRI protocols (sometimes referred to as abbreviated or targeted MRI) are gaining interest. Diffusion-weighted imaging (DWI) is effective in cancer detection (1, 2) without the need for gadolinium-based contrast agents, which is attractive from a cost, workflow, and patient safety perspective (3) and is ideally suited for rapid MRI. However, conventional single-shot spin-echo echo-planar imaging (ssEPI) DWI has limited spatial-resolution and is prone to artifact in the abdomen making it suboptimal for cancer surveillance yet remains popular because of wide availability and ease of use. Multishot DWI (msDWI) can help reduce these limitations (4, 5). We recently implemented a high-resolution, motion-mitigated, multi-shot SE-EPI DWI (msDWI) (9) method on clinical liver MRI protocols. The liver is one of the most common sites of metastatic disease for many cancers, including neuroendocrine tumors (NETs), with 25% of patients with NET suffering from liver metastases (6), impacting prognosis (7), and reducing survival up to 40% (8). Thus, rapid MRI for hepatic metastases detection in patients with NET may be clinically valuable.Goals
To determine the performance of msDWI and T2w imaging in detecting NET liver metastases. We suspected msDWI will allow detection of small lesions due to its high contrast-to-noise ratio (CNR) and may be well suited for liver metastasis surveillance.Approach
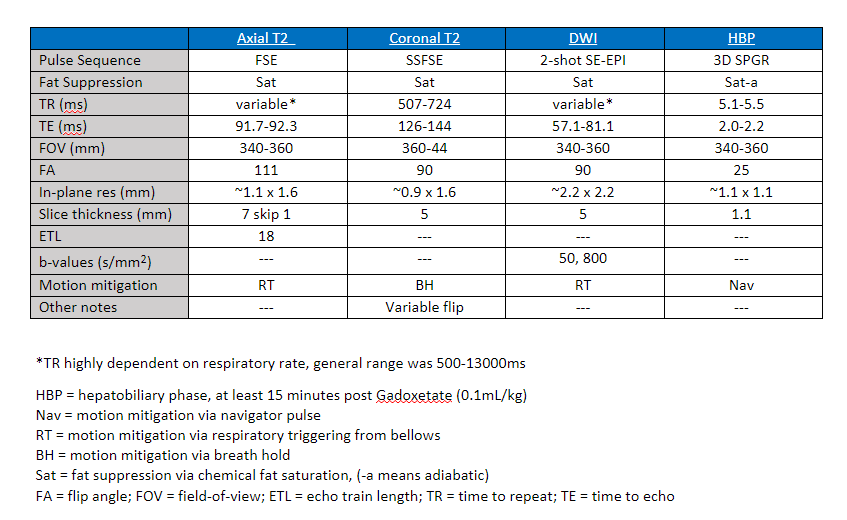
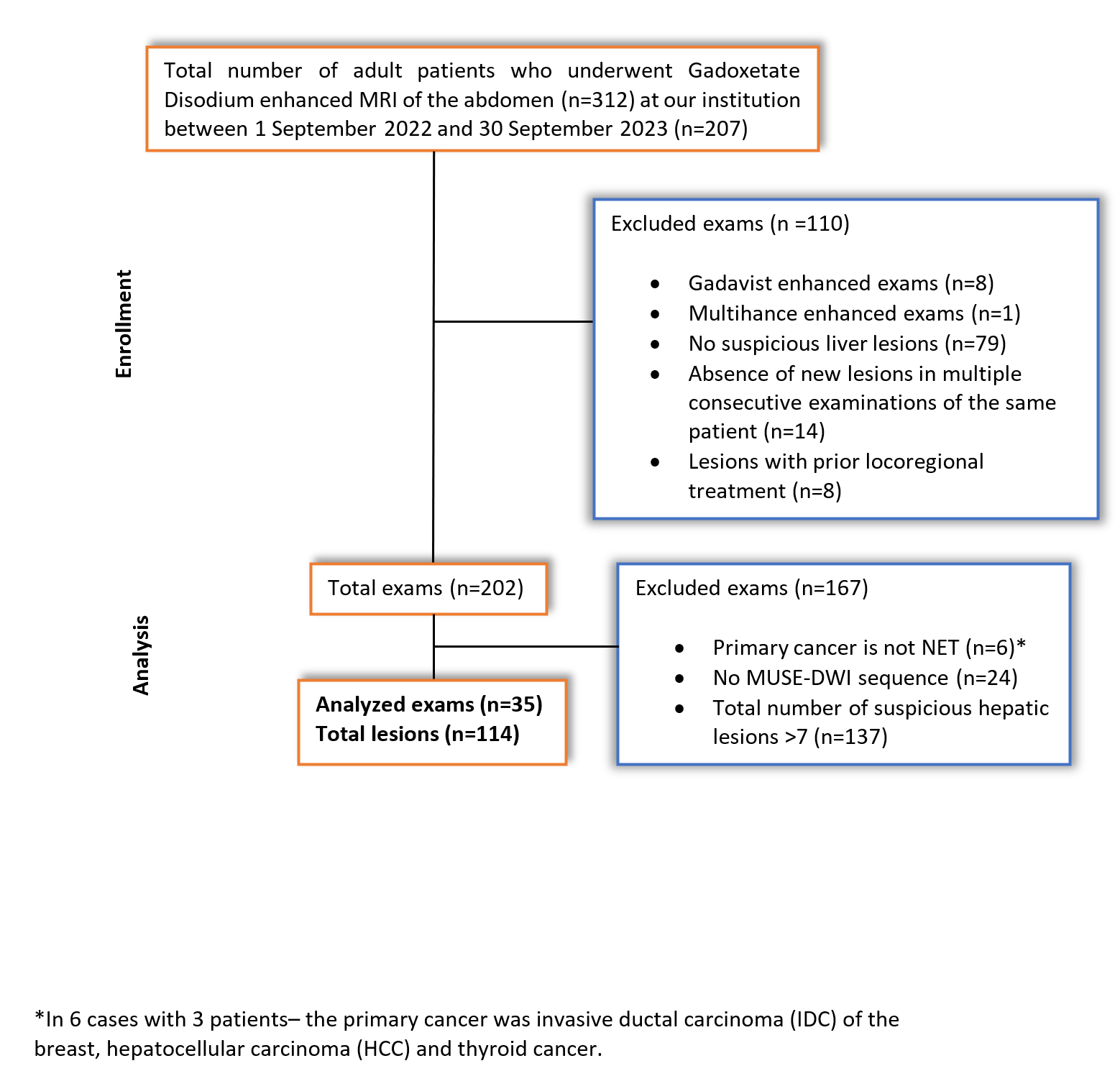
This retrospective study single-center study was conducted with Institutional Review Board approval and informed consent waiver, and adhered to institutional guidelines for data collection, storage, and analysis. Our imaging archive was searched for adult patients (18 and older) with a clinically documented NET diagnosis and at least one abdominal MRI performed with Gadoxetate (0.1mg/kg) contrast between 1 September 2022 and 30 September 2023. Exclusion criteria were patients without liver metastases, patients with more than 7 liver metastases (to avoid too many lesions of a single phenotype), and those that were missing any of the 4 key sequences (Table 1). The presence of a metastasis was determined based on all available imaging data (including prior imaging), including the current gold-standard for liver metastasis detection, post Gadoxetate hepatobiliary phase (HBP) 3D SPGR (10, 11). Metastases were categorized by size, segment, and viability (presumed based on detectable arterial hyperenhancement). Sensitivities were tabulated. A lesion was considered positive on T2w imaging if it was seen on either sequence.Results
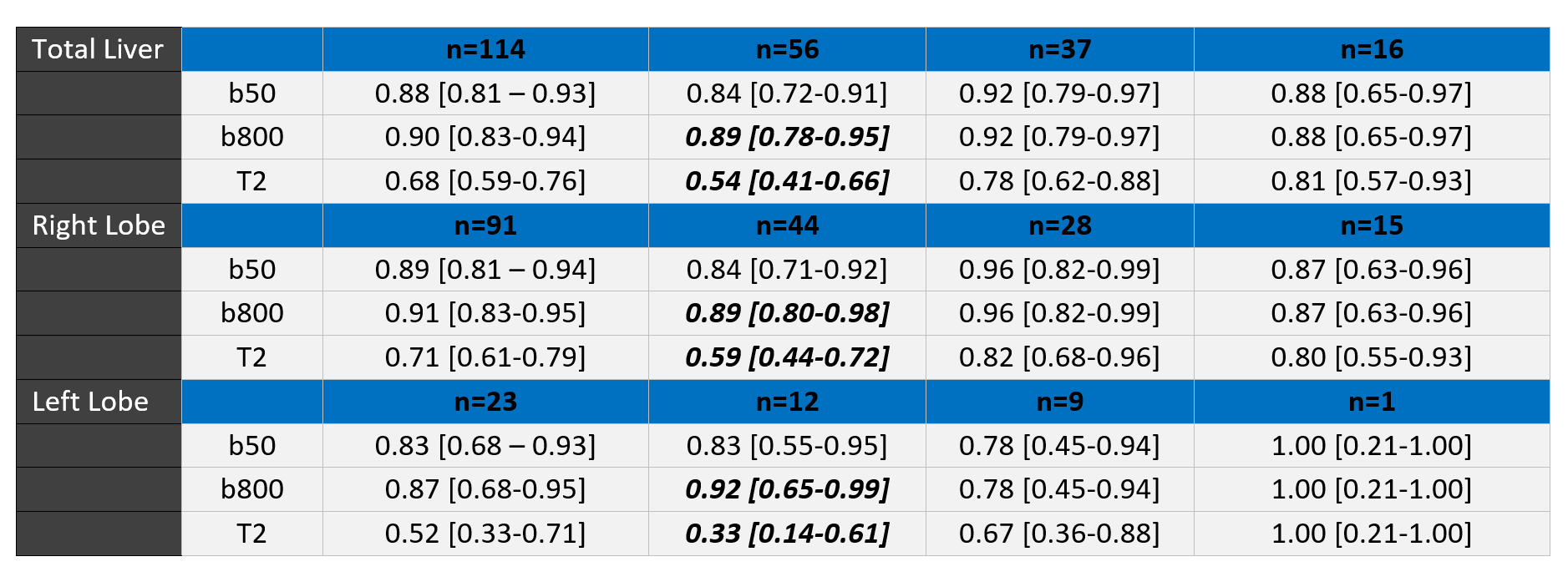
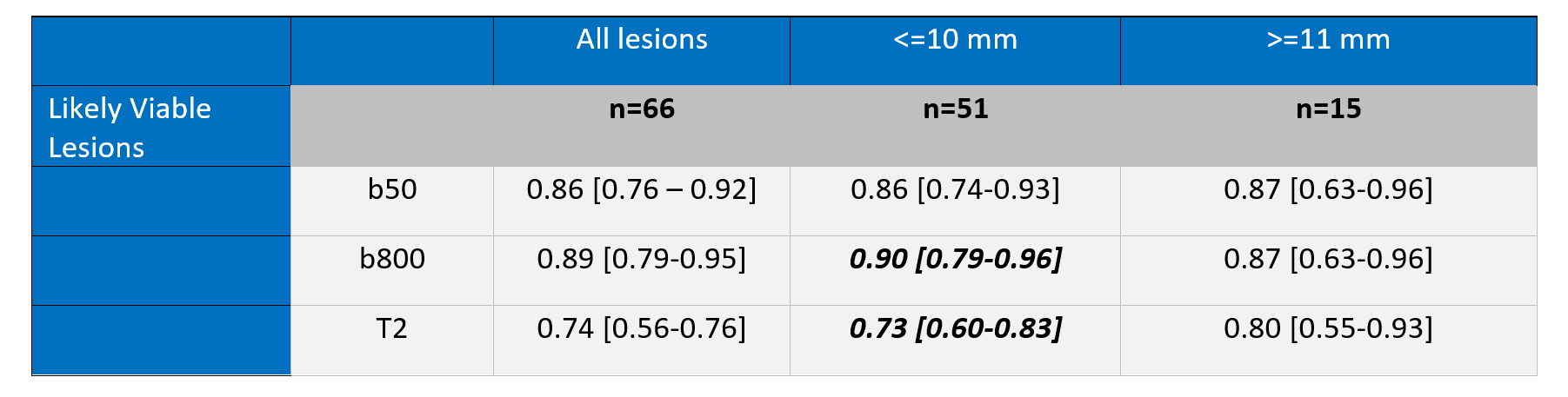
Among 207 patients with NET, 35 patients (15 females [43%] and 20 males [57%], median age 64 [range 22-88 years]) with 114 unique lesions were included (Figure 1). On a per-lesion basis, msDWI has an aggregate sensitivity of 90% [95% CI: 0.83-0.94] for all lesions, which was superior to the combination of T2w methods which had a sensitivity of 68% [95% CI: 0.59-0.76]. msDWI had a similar performance even for small (6-10mm: 92% [95% CI: 0.79-0.97]) and very small (<5mm: 89% [95% CI: 0.78-0.95]) lesions, while T2w imaging had a declining performance for decreasing lesions size (78% [95% CI: 0.62-0.88] and 54% [95% CI: 0.41-0.66], respectively). For lesions that were presumed viable, msDWI still outperformed T2w imaging (88% [95% CI: 0.76-0.94] versus 75% [95% CI: 0.61-0.85], respectively). The mean size was larger for lesions deemed viable as compared to all lesions (16.4 mm vs 9.5 mm, respectively), possibly reflecting the challenge in proving viability of very small lesions. Mean ADC values of presumably viable lesions was 0.96x10-3 mm2/s, while those of presumed non-viable lesions was 1.10x10-3 mm2/s, which was not significant (p = 0.2064).Discussion
msDWI outperformed multiplanar T2w imaging in detecting NET liver metastases, even when both a breath-hold coronal single-shot method (time efficient) and axial fast-spin echo with respiratory triggering method (high contrast) are used. The sensitivity of msDWI remained high even for small (<=5mm) lesions, while the performance of T2w imaging declined at smaller lesion sizes. msDWI also outperformed T2w imaging for lesions presumed to be viable, however the difference in performance may be underestimated due to the difficulty in proving viability of <=5mm lesions. While there was a difference in ADC values between presumed viable and non-viable lesions, the difference was small limiting establishment of a meaningful cutoff value.Conclusion
msDWI detects NET liver metastases with high sensitivity. Further investigation as a stand-alone option for MRI-based surveillance of liver metstases are warranted.Acknowledgements
No acknowledgement found.References
- Donati, Olivio F., Michael A. Fischer, Natalie Chuck, Roger Hunziker, Dominik Weishaupt, and Caecilia S. Reiner. “Accuracy and Confidence of Gd-EOB-DTPA Enhanced MRI and Diffusion-Weighted Imaging Alone and in Combination for the Diagnosis of Liver Metastases.” European Journal of Radiology 82, no. 5 (May 2013): 822–28. https://doi.org/10.1016/j.ejrad.2012.12.005.
- Hardie, Andrew D., Mohit Naik, Elizabeth M. Hecht, Hersh Chandarana, Lorenzo Mannelli, James S. Babb, and Bachir Taouli. “Diagnosis of Liver Metastases: Value of Diffusion-Weighted MRI Compared with Gadolinium-Enhanced MRI.” European Radiology 20, no. 6 (June 2010): 1431–41. https://doi.org/10.1007/s00330-009-1695-9.
- Kenis, Christoph, Filip Deckers, Bert De Foer, François Van Mieghem, Steven Van Laere, and Marc Pouillon. “Diagnosis of Liver Metastases: Can Diffusion-Weighted Imaging (DWI) Be Used as a Stand Alone Sequence?” European Journal of Radiology 81, no. 5 (May 2012): 1016–23. https://doi.org/10.1016/j.ejrad.2011.02.019.
- Geng, Ruiqi, Yuxin Zhang, James Rice, Matthias R. Muehler, Jitka Starekova, David R. Rutkowski, Nataliya V. Uboha, et al. “Motion-Robust, Blood-Suppressed, Reduced-Distortion Diffusion MRI of the Liver.” Magnetic Resonance in Medicine 89, no. 3 (2023): 908–21. https://doi.org/10.1002/mrm.29531.
- Kim, Yeun-Yoon, Myeong-Jin Kim, Sung-Min Gho, and Nieun Seo. “Comparison of Multiplexed Sensitivity Encoding and Single-Shot Echo-Planar Imaging for Diffusion-Weighted Imaging of the Liver.” European Journal of Radiology 132 (November 2020): 109292. https://doi.org/10.1016/j.ejrad.2020.109292.
- Veenendaal, Liesbeth M, Inne Hm Borel Rinkes, Cornelis Jm Lips, and Richard Van Hillegersberg. “Liver Metastases of Neuroendocrine Tumours; Early Reduction of Tumour Load to Improve Life Expectancy.” World Journal of Surgical Oncology 4, no. 1 (December 2006): 35. https://doi.org/10.1186/1477-7819-4-35.
- Bhosale, Priya, Jin Wei Kwek, Revathy Iyer, Wei Wei, Roland Bassett, and Vikas Kundra. “Follow-Up of Known Carcinoid Liver Metastases: Is Respiratory-Gated T2 Fast Spin-Echo Enough?” Neuroendocrinology 93, no. 4 (2011): 241–48. https://doi.org/10.1159/000326237.
- Kulkarni, Rugved, Irfan Kabir, James Hodson, Syed Raza, Tahir Shah, Sanjay Pandanaboyana, and Bobby V. M. Dasari. “Impact of the Extent of Resection of Neuroendocrine Tumor Liver Metastases on Survival: A Systematic Review and Meta-Analysis.” Annals of Hepato-Biliary-Pancreatic Surgery 26, no. 1 (February 28, 2022): 31–39. https://doi.org/10.14701/ahbps.21-101.
- Chen, Nan-kuei, Arnaud Guidon, Hing-Chiu Chang, and Allen W. Song. “A Robust Multi-Shot Scan Strategy for High-Resolution Diffusion Weighted MRI Enabled by Multiplexed Sensitivity-Encoding (MUSE).” NeuroImage 72 (May 2013): 41–47. https://doi.org/10.1016/j.neuroimage.2013.01.038.
- Luersen, Gustavo Felipe, W Wei, Eric P. Tamm, Priya R. Bhosale, and Janio Szklaruk. “Evaluation of Magnetic Resonance (MR) Biomarkers for Assessment of Response With Response Evaluation Criteria in Solid Tumors: Comparison of the Measurements of Neuroendocrine Tumor Liver Metastases (NETLM) With Various MR Sequences and at Multiple Phases of Contrast Administration.” Journal of Computer Assisted Tomography 40, no. 5 (2016): 717–22. https://doi.org/10.1097/RCT.0000000000000425.
- Morse, Brian, Daniel Jeong, Kerry Thomas, Dalanda Diallo, and Jonathan R. Strosberg. “Magnetic Resonance Imaging of Neuroendocrine Tumor Hepatic Metastases: Does Hepatobiliary Phase Imaging Improve Lesion Conspicuity and Interobserver Agreement of Lesion Measurements?” Pancreas 46, no. 9 (October 2017): 1219–24. https://doi.org/10.1097/MPA.0000000000000920.
Figures
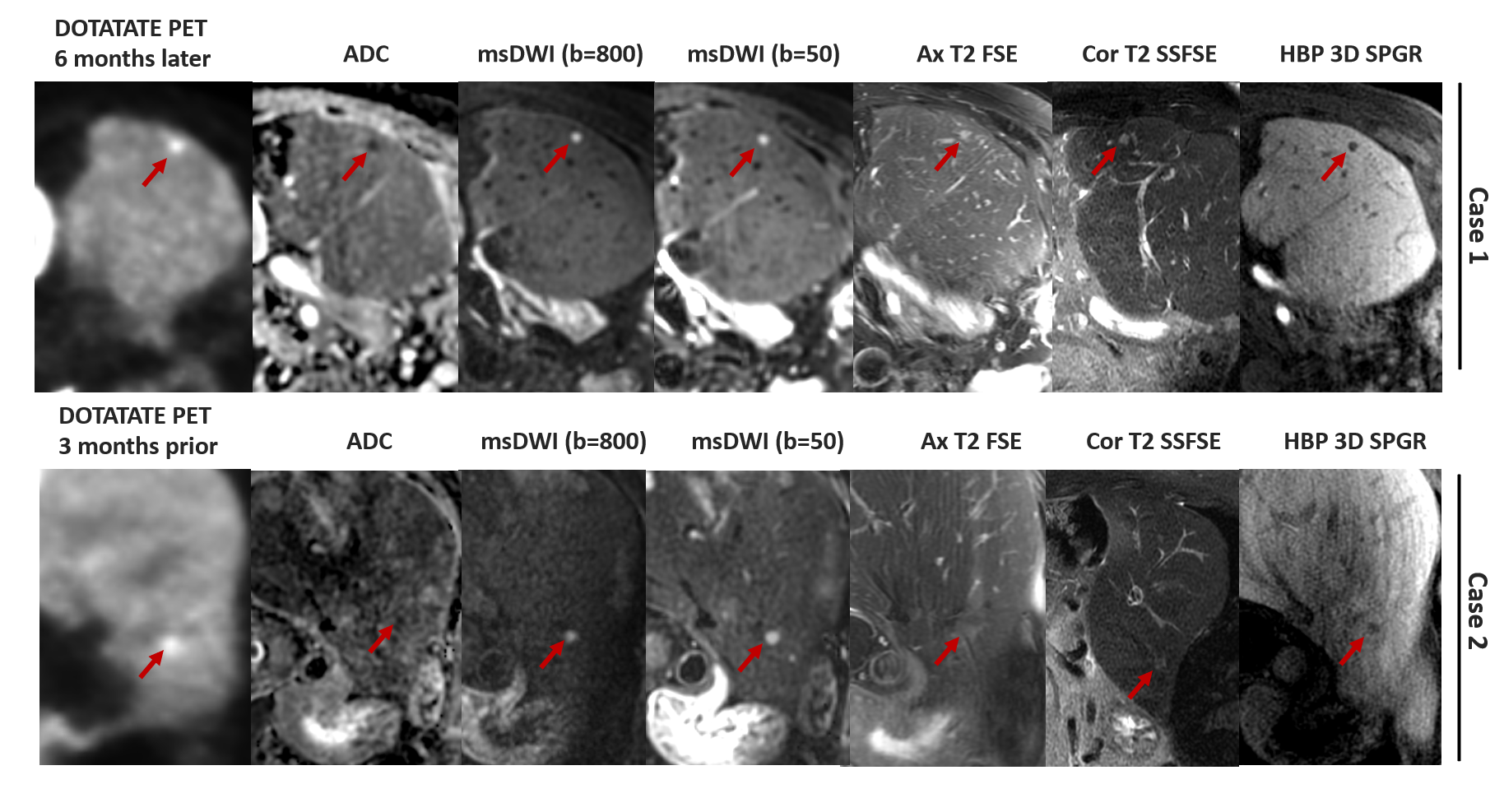
Case 1: 5mm lesion in segment 6 of a 54 year old male with grade jejunal 2 NET s/p multiple wedge resections and left lateral segmentectomy for hepatic metastasis. Lesion is barely distinguishable on T2 but is clear on DWI, with PET images showing it is viable.
Case 2: 8mm lesion in segment 2 near the dome of a 58 year old female with grade 2 pancreatic NET. Lesion cannot be differentiated from background structures on T2 but is clear on DWI, with PET images showing it is viable. ADC maps are somewhat compromised by cardiac motion in this case.