4142
Simplified LI-RADS Table for Hepatocellular Carcinoma Diagnosis on Extracellular-Contrast Enhanced MRI: AFP as an Additional Major Feature1Department of Radiology, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, China, 2Department of Radiology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, China, 3Department of Medical Imaging Center, Nanfang Hospital, Southern Medical University, Guangzhou, China, 4Department of Radiology, Affiliated Cancer Hospital & Institute of Guangzhou Medical University, Guangzhou, China, 5Department of Radiology, Meizhou People's Hospital, Meizhou, China, 6Department of Radiology, The Third Affiliated Hospital of Sun Yat-sen University Yuedong Hospital, Meizhou, China, 7Department of Hepatic Surgery and Liver transplantation Center, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, China
Synopsis
Keywords: Liver, Tumor, LI-RADS, AFP
Motivation: The MRI LI-RADS v2018 table is complex and has insufficient sensitivity.
Goal(s): To evaluate the diagnostic performance of the simplified LI-RADS table for HCC on ECA-MRI, and to determine the value of AFP level as an additional major feature.
Approach: We developed and compared the per-lesion sensitivity for HCC defined by LI-RADS v2018, simplified LI-RADS table, and both of them combined with AFP ≥ 200 ng/mL.
Results: Compared with LR-5 v2018, the simplified LI-RADS table provided higher sensitivity and comparable specificity for HCC. AFP ≥ 200 ng/mL may be a suitable additional major feature for further improving LR-5 v2018 and sLR-5 classification.
Impact: Our simplified LI-RADS table may be more convenient and clinically helpful, and the AFP ≥ 200 ng/mL may be a suitable additional major feature for accurate LR-5 and sLR-5 classification.
Introduction
The Liver Imaging Reporting and Data System (LI-RADS) table at MRI has been widely accepted as a standard for HCC diagnosis, but with complex and insufficient sensitivity[1,2]. Alpha-fetoprotein (AFP) as a sole diagnostic biomarker has insufficient and variable diagnostic performance according to patient characteristics and the AFP cutoff values used[3,4].To our knowledge, studies of US/CT/MRI LI-RADS including AFP as an additional major feature (MF) for the noninvasive diagnosis of HCC are limited [5–9].Thus, we aim to evaluate the diagnostic performance of the simplified LI-RADS table and to determine the value of AFP level as an additional MF for diagnosing HCC on extracellular contrast-enhanced MRI (ECA-MRI).Methods
This retrospective, multicenter study was approved by the local institutional review boards of all participating centers, with the informed consent requirement waived. A total of 1127 patients at high risk for HCC with 1322 observations who underwent ECA-MRI were enrolled from five independent centers (Center 1, training and internal test dataset, N = 690 and 204; Centers 2-5, external testing dataset, N = 233). The simplified LI-RADS table was formed by the no APHE and nonrim APHE columns: 1) for observations with No APHE, we developed sLR-5 criteria for observations with two major features; 2) for observations with nonrim APHE, we combined two size criteria cells of 10 -19 mm and ≥ 20 mm. When the observation showed one of the MFs but its size was at least 10 mm or showed two MFs of any size, it was re-categorized as sLR-5. Two blinded radiologists independently evaluated the LI-RADS features and categorized each observation according to the LI-RADS v2018 and the simplified LI-RADS table. Then, we chose AFP ≥ 200 ng/mL as an additional MF or as an alternative to “threshold growth” as an additional MF in the LI-RADS v2018 and simplified LI-RADS table. The diagnostic performances of each version of the LR-5 were compared using generalized estimating equations. Subgroup analyses were performed for small observations (≤ 30 mm).Results
This retrospective, multicenter study was approved by the local institutional review boards of all participating centers, with the informed consent requirement waived. A total of 1127 patients at high risk for HCC with 1322 observations who underwent ECA-MRI were enrolled from five independent centers (Center 1, training and internal test dataset, N = 690 and 204; Centers 2-5, external testing dataset, N = 233). The simplified LI-RADS table was formed by the no APHE and nonrim APHE columns: 1) for observations with No APHE, we developed sLR-5 criteria for observations with two major features; 2) for observations with nonrim APHE, we combined two size criteria cells of 10 -19 mm and ≥ 20 mm. When the observation showed one of the MFs but its size was at least 10 mm or showed two MFs of any size, it was categorized as sLR-5. Two blinded radiologists independently evaluated the LI-RADS features and categorized each observation according to the LI-RADS v2018 and the simplified LI-RADS table. Then, we chose AFP ≥ 200 ng/mL as an additional MF or as an alternative to “threshold growth” as an additional MF in the LI-RADS v2018 and simplified LI-RADS table. The diagnostic performances of each version of the LR-5 were compared using generalized estimating equations. Subgroup analyses were performed for small observations (≤ 30 mm).Discussion
For observations with no APHE, it has been reported that the vascular supply of early HCC significantly overlaps with that of HGDNs, which commonly show iso- or hypovascularity[10,11]. However, enhancing capsule appearance is a sign of high specificity for HCC diagnosis[12]. For observations with nonrim APHE, our result is consistent with one study for the diagnosis of 10-19 mm HCCs using ECA-MRI and another study in diagnosing small HCCs using HBA-MRI[13,14]. This is probably because the LI-RADS category assignment for LR-5 and non-LR-5 is rarely determined by size between 10-19 mm and 20 mm[15]. The cutoff value of AFP ≥ 200 ng/mL used in our study is consistent with recent studies in the CEUS LI-RADS combined with serum AFP level for HCC diagnosis[5,6]. It suggested that increased AFP levels are also commonly observed in patients with acute and chronic liver conditions and cirrhosis, which overlaps with elevated AFP levels in patients with HCC. Selecting a high cutoff value for the AFP level may reduce the false positive rate of HCC diagnosis[3].Conclusions
The simplified LI-RADS table provides the higher sensitivity for HCC, and AFP level (≥ 200 ng/mL) further significantly increases sensitivity for both of LR-5 v2018 and simplified LR-5.Acknowledgements
National Natural Science Foundation of China grant (82271973 and 91959118, Jin Wang), The ‘Five Five’ Project of the Third Affiliated Hospital of Sun Yat-sen University (2023WW103, Jin Wang), Guangdong Basic and Applied Research Foundation (2021A1515010582, Jin Wang), Key Research and Development Program of Guangdong Province (2019B020235002, Jin Wang), China International Medical Foundation SKY Research Fund for Medical Imaging (Z-2014-07-2101 and Z-2014-07-1912-15, Jin Wang), Clinical Research Foundation of the 3rd Affiliated Hospital of Sun Yat-Sen University (YHJH201901, Jin Wang), National Natural Science Foundation of China (81770648 and 81972286, Yang Yang), National Key R&D Plan (2017YFA0104304, Yang Yang), and Science and Technology Program of Guangdong Province (2020B1212060019, Yang Yang).References
[1] Marrero J A, Kulik L M, Sirlin C B, Zhu A X, Finn R S, Abecassis M M, Roberts L R, Heimbach J K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases: Marrero et al.[J]. Hepatology, 2018, 68(2): 723–750.
[2] Chernyak V, Fowler K J, Kamaya A, Kielar A Z, Elsayes K M, Bashir M R, Kono Y, Do R K, Mitchell D G, Singal A G, Tang A, Sirlin C B. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients[J]. Radiology, 2018, 289(3): 816–830.
[3] Hanif H, Ali M J, Susheela A T, Khan I W, Luna-Cuadros M A, Khan M M, Lau D T-Y. Update on the applications and limitations of alpha-fetoprotein for hepatocellular carcinoma[J]. World Journal of Gastroenterology, 2022, 28(2): 216–229.
[4] Arif D, Mettler T, Adeyi O A. Mimics of hepatocellular carcinoma: a review and an approach to avoiding histopathological diagnostic missteps[J]. Human Pathology, 2021, 112: 116–127.
[5] Gong W, Wu J, Wei H, Jiang Z, Wan M, Wu C, Xue W, Ma R, Zhou X, Zhou H. Combining serum AFP and CEUS LI-RADS for better diagnostic performance in Chinese high-risk patients[J]. Abdominal Radiology, 2023, 128(4): 393–401.
[6] Li C, Huang H, Ruan S, Hu H, Xian M, Xie X, Lu M, Kuang M, Wang Y, Chen L. An assessment of liver lesions using a combination of CEUS LI-RADS and AFP[J]. Abdominal Radiology, 2022, 47(4): 1311–1320.
[7] Huang P, Wu F, Hou K, Zhou C, Xiao Y, Wang C, Miao G, Yang C, Zeng M. Diagnostic algorithm for subcentimeter hepatocellular carcinoma using alpha-fetoprotein and imaging features on gadoxetic acid–enhanced MRI[J]. European Radiology, 2023[2023-10-05].
[8] Jiang Z-P, Zeng K-Y, Huang J-Y, Yang J, Yang R, Li J-W, Qiu T-T, Luo Y, Lu Q. Differentiating malignant and benign focal liver lesions in children using CEUS LI-RADS combined with serum alpha-fetoprotein[J]. World Journal of Gastroenterology, 2022, 28(21): 2350–2360.
[9] Jiang H, Song B, Qin Y, Chen J, Xiao D, Ha H I, Liu X, Oloruntoba-Sanders O, Erkanli A, Muir A J, Bashir M R. Diagnosis of LI-RADS M lesions on gadoxetate-enhanced MRI: identifying cholangiocarcinoma-containing tumor with serum markers and imaging features[J]. European Radiology, 2021, 31(6): 3638–3648.
[10] Hytiroglou P, Bioulac-Sage P, Theise N D, Sempoux C. Etiology, Pathogenesis, Diagnosis, and Practical Implications of Hepatocellular Neoplasms[J]. Cancers, 2022, 14(15): 3670.
[11] Park H J, Choi B I, Lee E S, Park S B, Lee J B. How to Differentiate Borderline Hepatic Nodules in Hepatocarcinogenesis: Emphasis on Imaging Diagnosis[J]. Liver Cancer, 2017, 6(3): 189–203.
[12] Cerny M, Bergeron C, Billiard J-S, Murphy-Lavallée J, Olivié D, Bérubé J, Fan B, Castel H, Turcotte S, Perreault P, Chagnon M, Tang A. LI-RADS for MR Imaging Diagnosis of Hepatocellular Carcinoma: Performance of Major and Ancillary Features[J]. Radiology, 2018, 288(1): 118–128.
[13] Chen J, Kuang S, Zhang Y, Tang W, Xie S, Zhang L, Rong D, He B, Deng Y, Xiao Y, Shi W, Fowler K, Wang J, Sirlin C B. Increasing the sensitivity of LI-RADS v2018 for diagnosis of small (10–19 mm) HCC on extracellular contrast-enhanced MRI[J]. Abdominal Radiology, 2021, 46(4): 1530–1542.
[14] Kwag M, Choi S H, Choi S J, Byun J H, Won H J, Shin Y M. Simplified LI-RADS for Hepatocellular Carcinoma Diagnosis at Gadoxetic Acid–enhanced MRI[J]. Radiology, 2022: 220659.
[15] Van Der Pol C B, McInnes M D F, Salameh J-P, Levis B, Chernyak V, Sirlin C B, Bashir M R, Allen B C, Burke L M B, Choi J-Y, Choi S H, Forner A, Fraum T J, Giamperoli A, Jiang H, Joo I, Kang Z, Kierans A S, Kang H-J, Khatri G, Kim J H, Kim M-J, Kim S Y, Kim Y-Y, Kwon H, Lee J M, Lewis S C, McGinty K A, Mulazzani L, Park M-S, Piscaglia F, Podgórska J, Reiner C S, Ronot M, Rosiak G, Song B, Song J S, Tang A, Terzi E, Wang J, Wang W, Wilson S R, Yokoo T. CT/MRI and CEUS LI-RADS Major Features Association with Hepatocellular Carcinoma: Individual Patient Data Meta-Analysis[J]. Radiology, 2022, 302(2): 326–335.
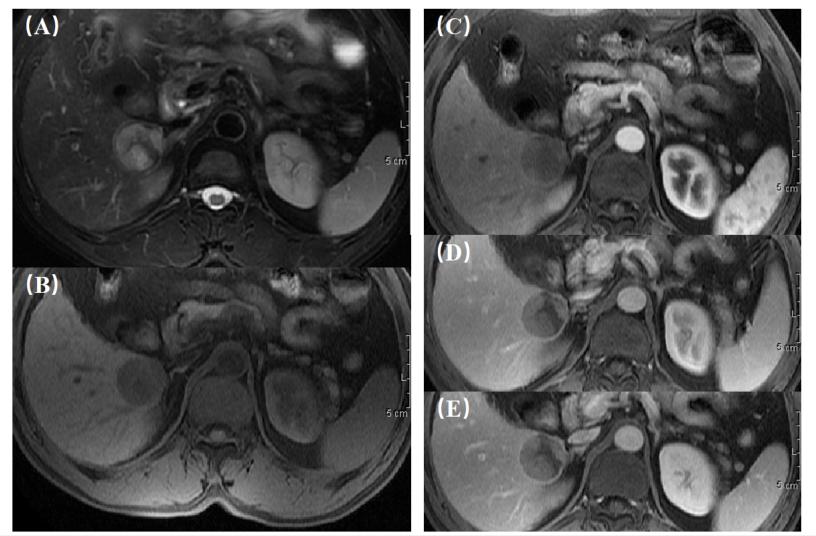
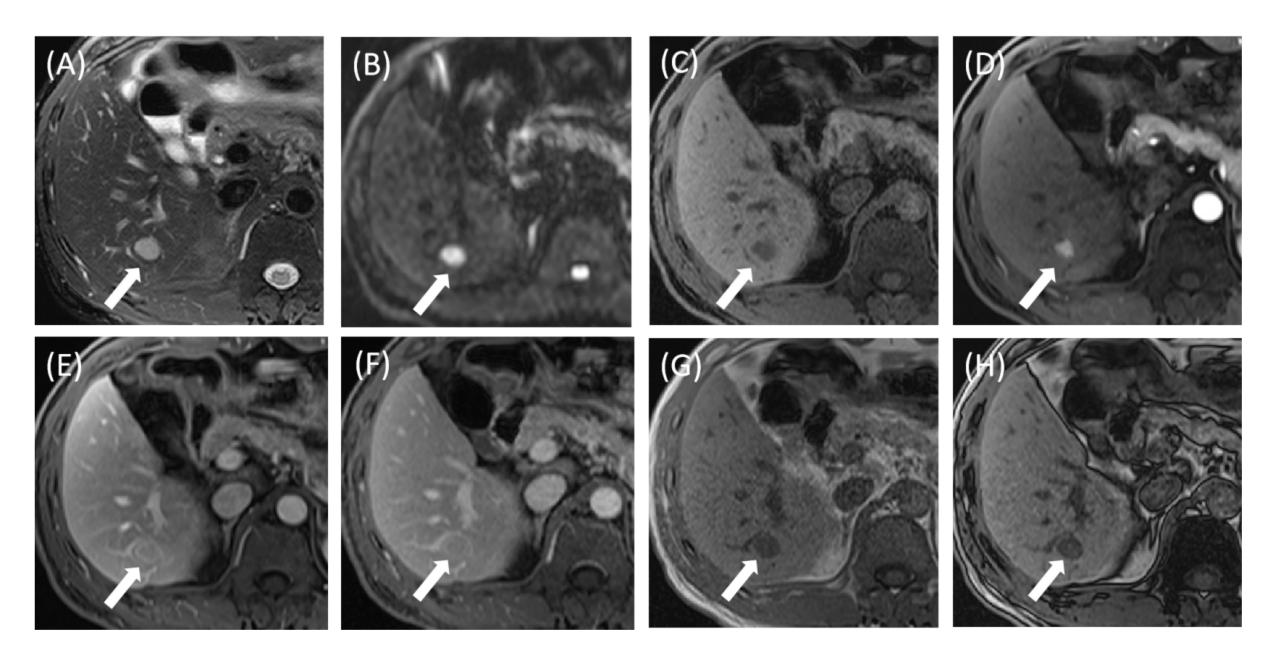
Figures