4141
Gadoxetic acid‑enhanced MRI for evaluation of vessels encapsulating tumor clusters and microvascular invasion in hepatocellular carcinoma1Affiliated Nantong Hospital 3 of Nantong University, Nantong Third People’s Hospital, Nantong, China, 2Philips Healthcare, Shanghai, China, Nantong, China
Synopsis
Keywords: Liver, Liver
Motivation: VETC and MVI have a synergistic effect on prognosis assessment and treatment selection of HCC. Preoperative noninvasive evaluation of VETC and MVI is important.
Goal(s): To explore the diagnosis value of nomograms based on preoperative gadoxetic acid (GA)-enhanced MRI features for MVI, VETC, and RFS in patients with HCC.
Approach: Retrospective study explored the relationship between the clinical and imaging features of MVI, VETC, and MVI+/VETC+ using the same dataset.
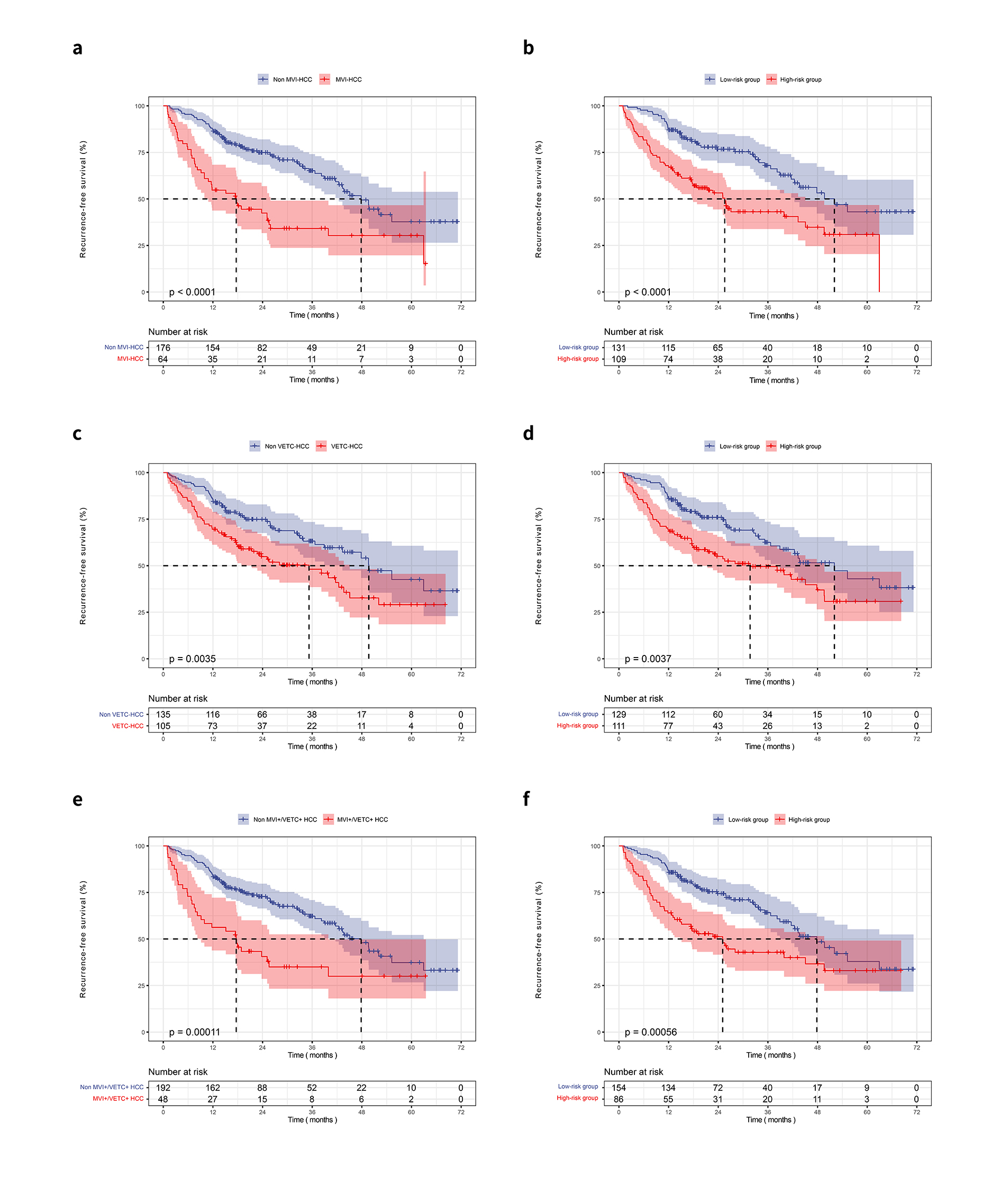
Results: Nomograms incorporating independent indicators showed good performance in the training and internal validation cohorts. Significant differences in recurrence rates between the nomogram-evaluated high- and low-risk stratification were found.
Impact: Through the in-depth exploration of the combination of MVI and VETC, we can deepen the understanding of tumor metastasis heterogeneity, and the diagnosis and treatment plan, prognosis prediction and risk stratification of tumor patients can be formulated.
Introduction
EMT-mediated metastasis promotes the progression of microvascular invasion (MVI).1 The histopathological grades of MVI, including M0, M1, and M2, are significantly negatively correlated with recurrence-free survival (RFS) in patients with HCC.1,2 However, many patients with MVI-negative HCC are also at risk of early recurrence after radical resection,3,4 suggesting that MVI is inadequate for explaining the mechanism of HCC recurrence and metastasis. Vessels encapsulating tumor clusters (VETC)-mediated metastasis cannot be explained by single-cell metastasis based on EMT.5,6 In VETC+ HCC, tumor cell clusters are completely surrounded by CD34(+) endothelial cells, and the overall efficient metastasis is carried out. The cancer nest metastasize to the target organ with the bloodstream, and proliferate to form new metastases, leading to a higher rate of VETC+ HCC metastasis, more likely recurrence after surgery, and a worse prognosis for patients.5,7 VETC and MVI are two different vascular patterns that underlie distinct molecular and cellular bases. Lin et al. reported that VETC is weighted slightly higher than MVI in a multivariable model in evaluating HCC recurrence.8 The presence of VETC suggests that HCC is more aggressive.9 Lu et al.10 found that VETC+/MVI+ patients had the worst overall survival (OS) and disease-free survival (DFS), while patients with VETC-/MVI- had the best long-term prognosis. No studies have focused at the independent risk factors only associated with VETC+/MVI+ HCCs and no studies have simultaneously predicted MVI+, VETC+, and VETC+/MVI+ in the same patient cohort.Methods
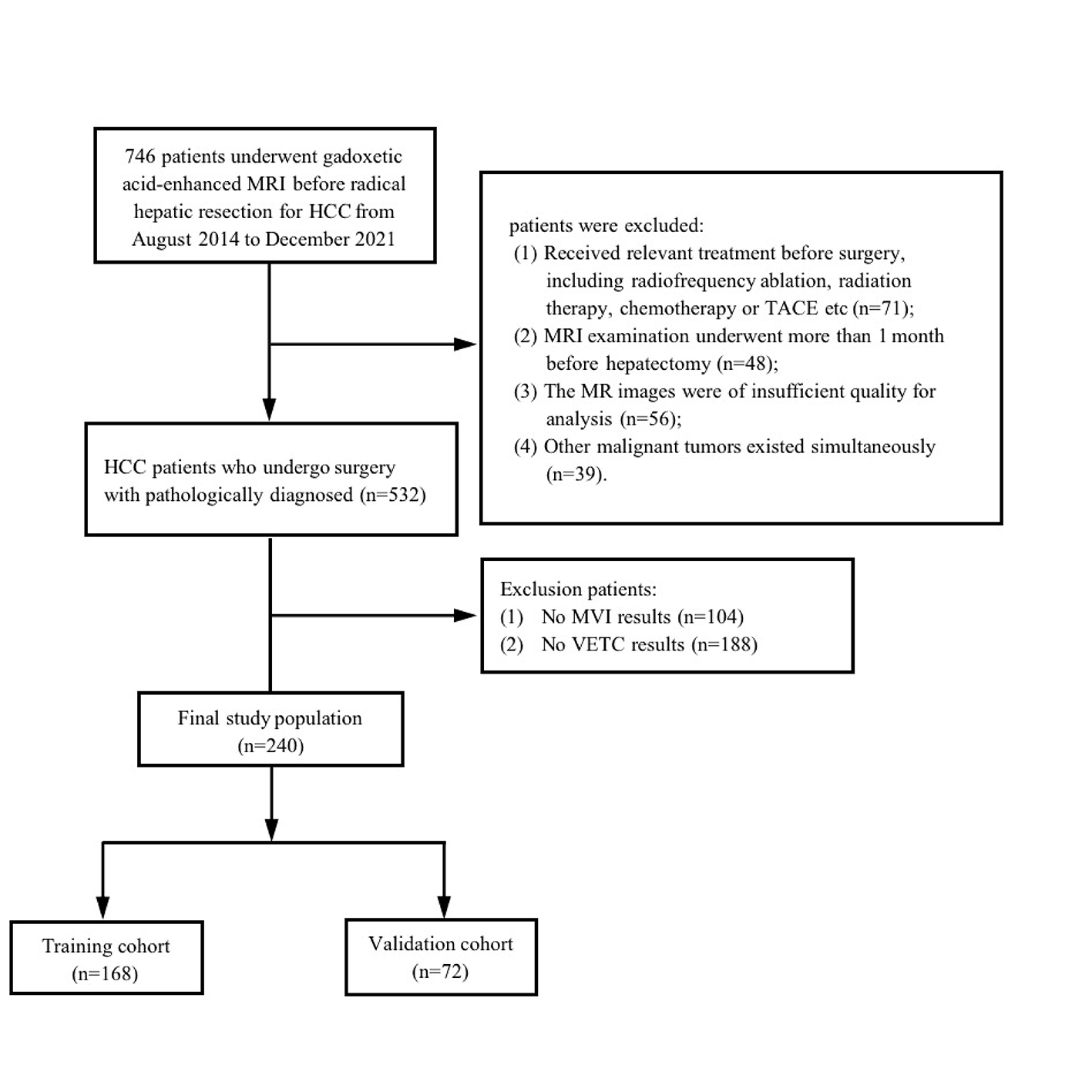
240 patients with pathologically confirmed HCC (allocated to training and validation sets with a 7:3 ratio) who underwent GA-enhanced MRI examination followed by radical hepatectomy. Preoperative clinical characteristics and imaging features of subjective assessment by the radiologist were collected and analyzed. Regression-based nomograms to diagnose MVI, VETC, and VETC+/MVI+ were developed for HCC in the training set. Based on the nomograms, the RFS prognostic stratification system was further.Results
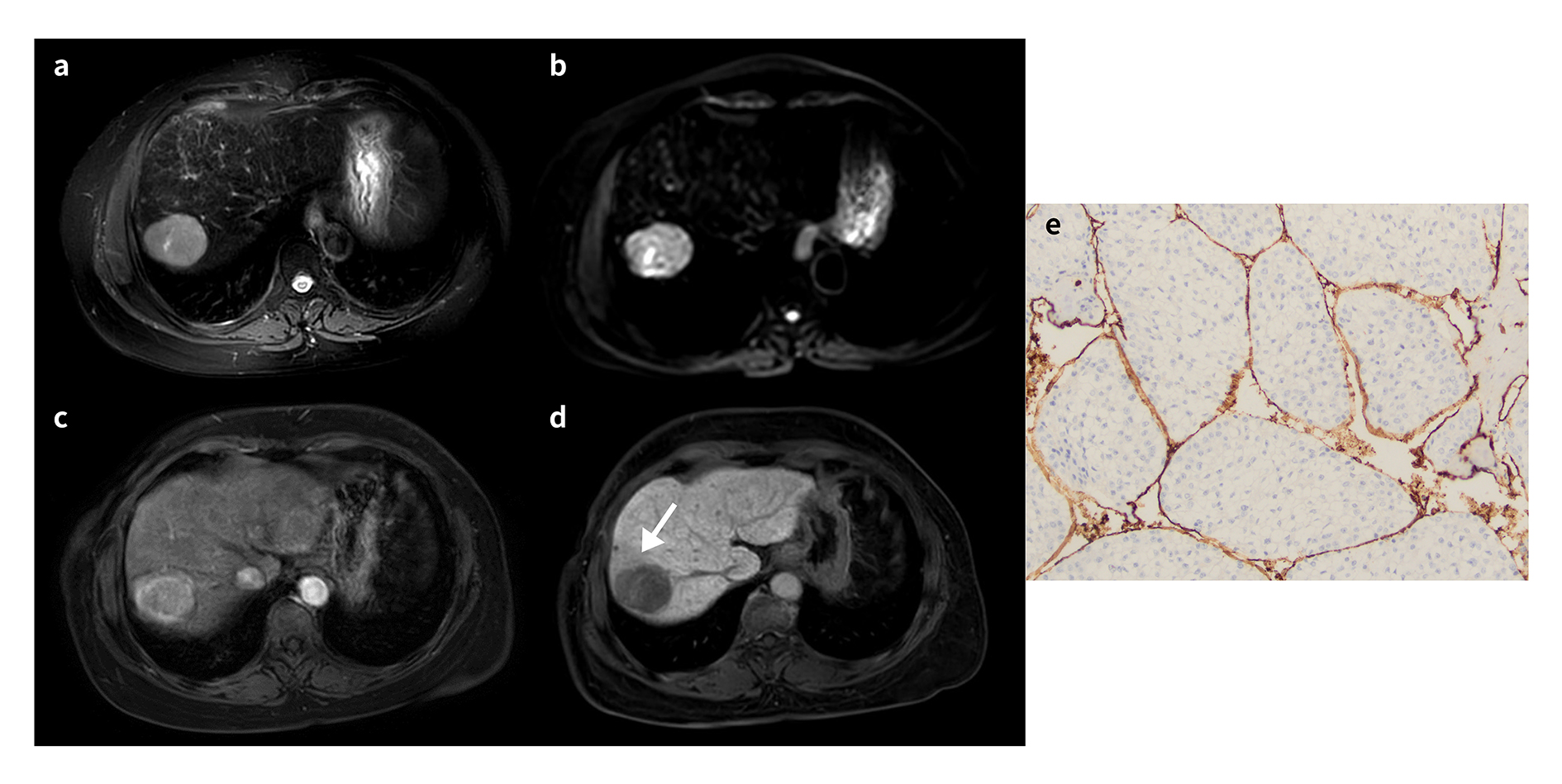
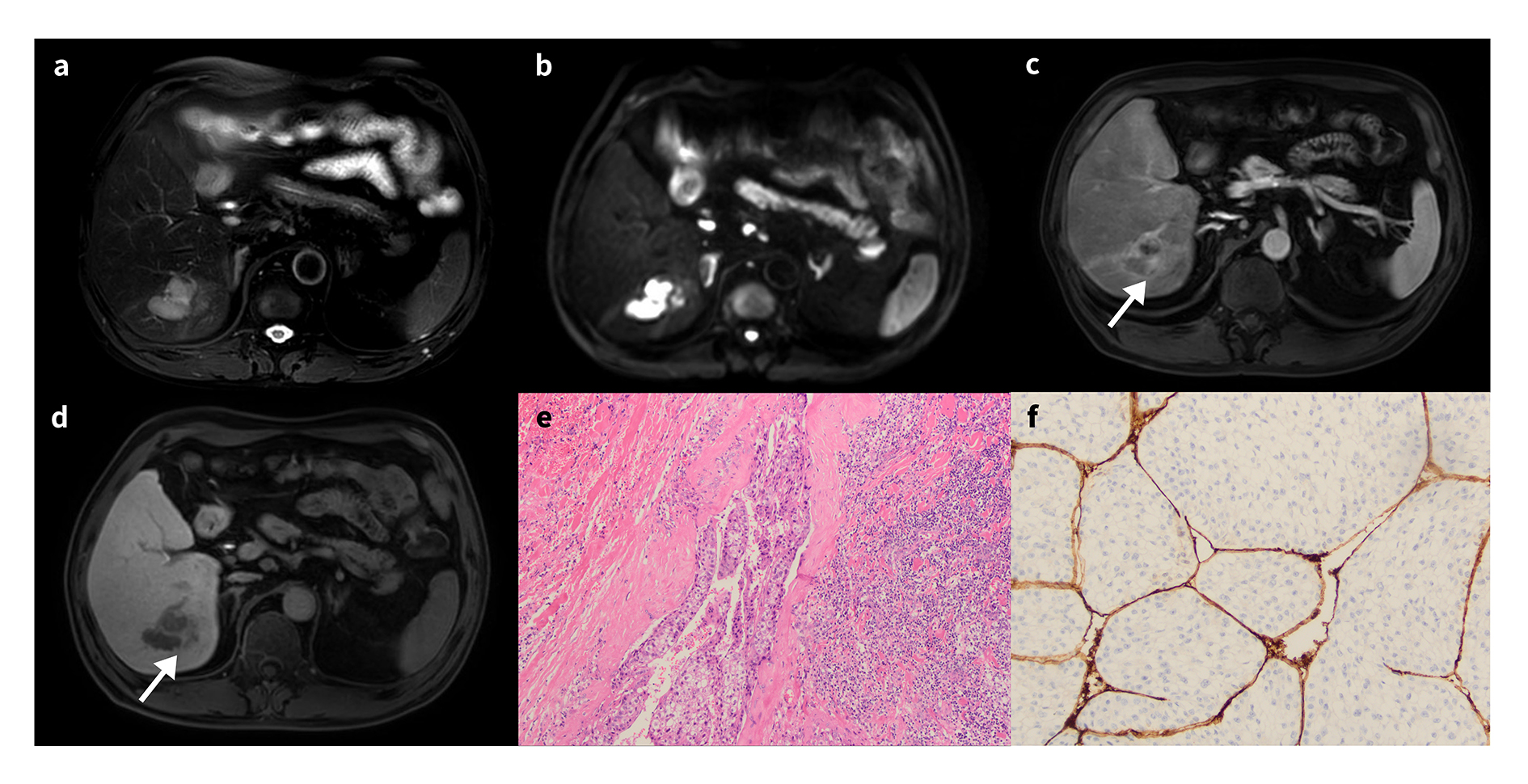
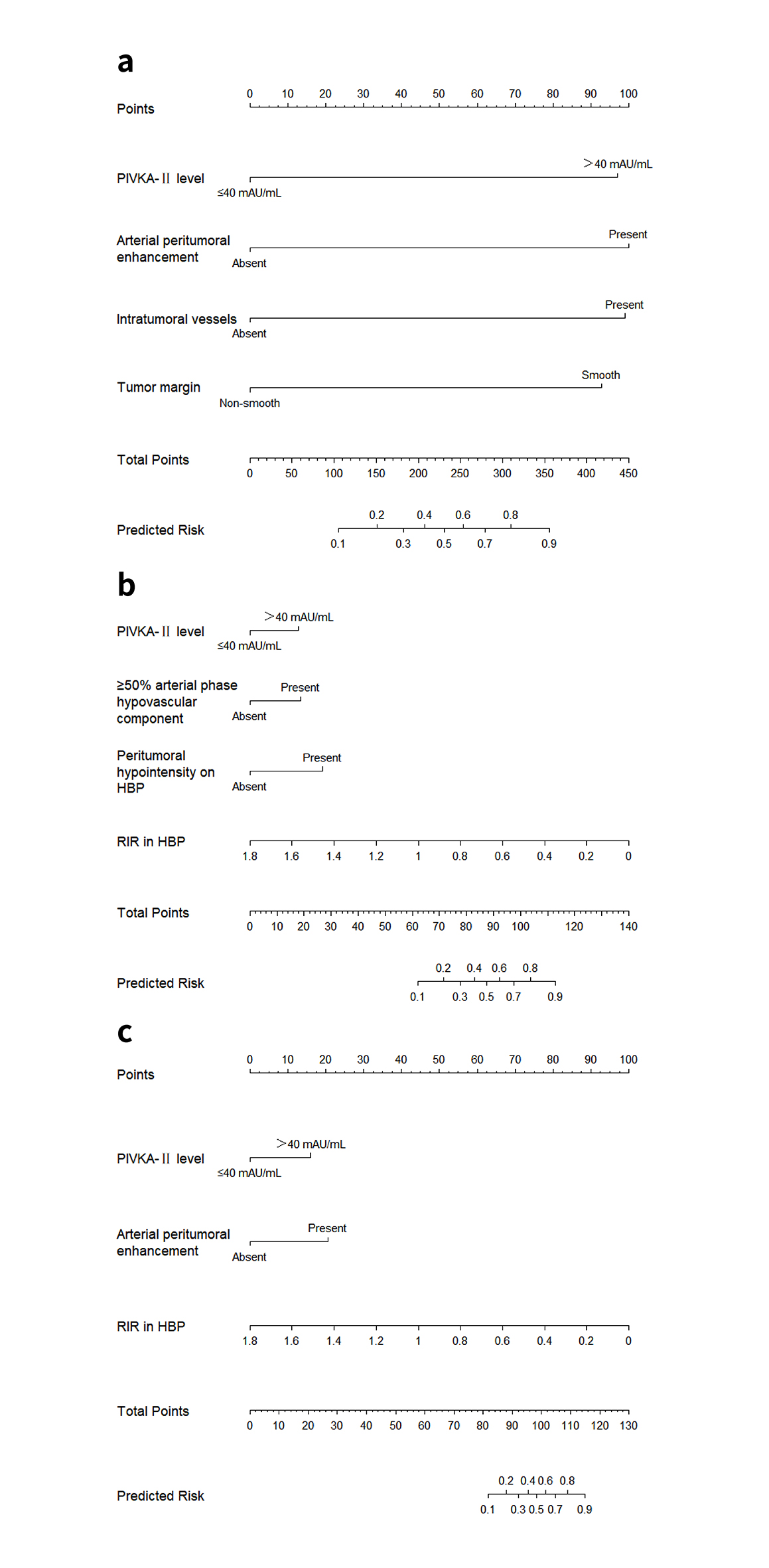
Serum PIVKA-II level >40 mAU/mL, arterial peritumoral enhancement, intratumoral vessels, and nonsmooth tumor margins were independently associated with MVI-HCC. Independent risk factors for diagnosing VETC-HCC were PIVKA-II level >40 mAU/mL, the ≥50% arterial phase hypovascular component, peritumoral hypointensity on HBP, and lower RIR on HBP images. PIVKA-II level >40 mAU/mL, arterial peritumoral enhancement, and lower RIR on HBP images were significant factors for estimating VETC+/MVI+ HCCs. Three nomograms incorporating these indicators showed good performance in the training and internal validation cohorts. Significant differences in recurrence rates between the nomogram-evaluated high- and low-risk stratification were found.Discussion
PIVKA-II elevation is related to undesirable biological behaviors such as histological vascular invasion, and metastasis of cancer cells, and has the potential to reflect the progression of HCC. 11,12 Arterial peritumoral enhancement,13 intratumoral vessels,14 and unsmooth tumor margin13-16 have been reported as independent risk factors for MVI, which is consistent with our results. Most massive macrotrabecular-massive (MTM) patterns exhibit VETC+ expression.17-19 Rhee et al.18 and Cha et al.19 observed that MTM-HCC was accompanied by ≥ 50% of arterial phase hypovascular components, which is consistent with our study. This study found that peritumoral hypointensity in HBP images was significantly associated with VETC. Previous studies have shown that peritumoral hypointensity on HBP images was significantly associated with MVI and high tumor grade,15,20 implying that this variable has the potential to reflect the malignant biological behavior of HCC. Our study found that VETC+ HCCs had significantly lower RIR on HBP images than VETC-negative HCCs, which is consistent with the study of Fan et al.,17 who found that a tumor-to-liver SI ratio of 0.585 or less on HBP images was a significant independent risk factor for predicting VETC+ HCCs. Moreover, Zheng et al.21 reported that HCCs with a lower tumor-to-liver signal ratio on HBP images exhibited greater aggressiveness, higher tumor grade, and shorter RFS. This supports the theory that VETC is a potent predictor of aggressive HCC.9 Multivariable logistic regression analysis showed that arterial peritumoral enhancement and lower RIR on HBP images were independent risk factors for MVI+/VETC+ HCCs. Yang et al.22 proposed that AFP >400 ng/mL, intratumor vascularity, and enhancement pattern can be used to characterize the positive VETC and/or MVI (VM patterns), and intratumor vascularity was associated with RFS. Notably, how our research differs from theirs may be related to the different groupings of cases included in the study by Yang et al.22, who put VETC+/MVI-, VETC-/MVI+ and MVI+/VETC+ together in a group. Another difference is that our study used GA-enhanced MRI.Conclusion
Preoperative noninvasive models combining the GA-enhanced MRI signature and clinical variables have potential to preoperatively diagnose MVI, VETC, and VETC+/MVI+ in HCC.Acknowledgements
Not applicable.References
1. Zhang T, Guo J, Gu J, et al. KIAA0101 is a novel transcriptional target of FoxM1 and is involved in the regulation of hepatocellular carcinoma microvascular invasion by regulating epithelial-mesenchymal transition. J Cancer 2019;10 (15):3501-3516.
2. Chong HH, Yang L, Sheng RF, et al. Multi-scale and multi-parametric radiomics of gadoxetate disodium-enhanced MRI predicts microvascular invasion and outcome in patients with solitary hepatocellular carcinoma ≤ 5 cm. Eur Radiol 2021;31(7):4824-4838.
3. Wang L, Feng B, Li D, et al. Risk stratification of solitary hepatocellular carcinoma ≤ 5 cm without microvascular invasion: prognostic values of MR imaging features based on LI-RADS and clinical parameters. Eur Radiol 2023;33(5):3592-3603.
4. Qu Q, Lu M, Xu L, et al. A model incorporating histopathology and preoperative gadoxetic acid-enhanced MRI to predict early recurrence of hepatocellular carcinoma without microvascular invasion after curative hepatectomy. Br J Radiol 2023;96(1144):20220739.
5. Sugino T, Yamaguchi T, Hoshi N, et al. Sinusoidal tumor angiogenesis is a key component in hepatocellular carcinoma metastasis. Clin Exp Metastasis 2008;25(7):835-41.
6. Fang JH, Zhou HC, Zhang C, et al. A novel vascular pattern promotes metastasis of hepatocellular carcinoma in an epithelial-mesenchymal transition-independent manner. Hepatology 2015;62(2):452-65.
7. Fang JH, Xu L, Shang LR, et al. Vessels That Encapsulate Tumor Clusters (VETC) Pattern Is a Predictor of Sorafenib Benefit in Patients with Hepatocellular Carcinoma. Hepatology 2019;70(3):824-839.
8. Lin WP, Xing KL, Fu JC, et al. Development and Validation of a Model Including Distinct Vascular Patterns to Estimate Survival in Hepatocellular Carcinoma. JAMA Netw Open 2021;4(9):e2125055.
9. Renne SL, Woo HY, Allegra S, et al. Vessels Encapsulating Tumor Clusters (VETC) Is a Powerful Predictor of Aggressive Hepatocellular Carcinoma. Hepatology 2020;71(1):183-195.
10. Lu L, Wei W, Huang C, et al. A new horizon in risk stratification of hepatocellular carcinoma by integrating vessels that encapsulate tumor clusters and microvascular invasion. Hepatol Int 2021;15(3):651-662.
11. Yang Y, Li G, Lu Z, Liu Y, Kong J, Liu J. Progression of Prothrombin Induced by Vitamin K Absence-II in Hepatocellular Carcinoma. Front Oncol 2021;11:726213.
12. Matsubara M, Shiraha H, Kataoka J, et al. Des-γ-carboxyl prothrombin is associated with tumor angiogenesis in hepatocellular carcinoma. J Gastroenterol Hepatol 2012;27(10):1602-8.
13. Lee S, Kim SH, Lee JE, Sinn DH, Park CK. Preoperative gadoxetic acid-enhanced MRI for predicting microvascular invasion in patients with single hepatocellular carcinoma. J Hepatol 2017;67(3):526-534.
14. Jiang H, Wei J, Fu F, et al. Predicting microvascular invasion in hepatocellular carcinoma: A dual-institution study on gadoxetate disodium-enhanced MRI. Liver Int 2022;42(5):1158-1172.
15. Liang X, Shi S, Gao T. Preoperative gadoxetic acid-enhanced MRI predicts aggressive pathological features in LI-RADS category 5 hepatocellular carcinoma. Clin Radiol 2022;77(9):708-716.
16. Hu H, Zheng Q, Huang Y, et al. A non-smooth tumor margin on preoperative imaging assesses microvascular invasion of hepatocellular carcinoma: A systematic review and meta-analysis. Sci Rep 2017;7(1):15375.
17. Fan Y, Yu Y, Hu M, et al. Imaging features based on Gd-EOB-DTPA-enhanced MRI for predicting vessels encapsulating tumor clusters (VETC) in patients with hepatocellular carcinoma. Br J Radiol 2021;94(1119):20200950.
18. Rhee H, Cho ES, Nahm JH, et al. Gadoxetic acid-enhanced MRI of macrotrabecular-massive hepatocellular carcinoma and its prognostic implications. J Hepatol 2021;74(1):109-121.
19. Cha H, Choi JY, Park YN, et al. Comparison of imaging findings of macrotrabecular-massive hepatocellular carcinoma using CT and gadoxetic acid-enhanced MRI. Eur Radiol 2023;33(2):1364-1377.
20. Ahn SJ, Kim JH, Park SJ, Kim ST, Han JK. Hepatocellular carcinoma: preoperative gadoxetic acid-enhanced MR imaging can predict early recurrence after curative resection using image features and texture analysis. Abdom Radiol (NY) 2019;44(2):539-548.
21. Ye Z, Cao L, Wei Y, et al. Preoperative prediction of hepatocellular carcinoma with highly aggressive characteristics using quantitative parameters derived from hepatobiliary phase MR images. Ann Transl Med 2020;8(4):85.
22. Yang J, Dong X, Wang G, et al. Preoperative MRI features for characterization of vessels encapsulating tumor clusters and microvascular invasion in hepatocellular carcinoma. Abdom Radiol (NY) 2023;48(2):554-566.
Figures