4136
Comparative Analysis of Contrast Agents for HCC Diagnosis Using LI-RADS 2018v1The University of Hong Kong -Shenzhen Hospital, Shenzhen, China, 2Southern Medical University, GuangZhou, China, 3Shenzhen Second People's Hospital, Shenzhen, China, 4Sourth Medical University, GuangZhou, China, 5Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Liver, Liver
Motivation: Enhance precision in hepatocellular carcinoma (HCC) diagnosis by determining the superior contrast agent.
Goal(s): Compare Gd-EOB-DTPA and Gd-BOPTA efficiency in displaying LI-RADS-recommended HCC features.
Approach: Retrospective analysis of 98 HCC lesions using Gd-EOB-DTPA-MR and Gd-BOPTA-MR, assessing enhancement patterns and lesion-to-liver contrast.
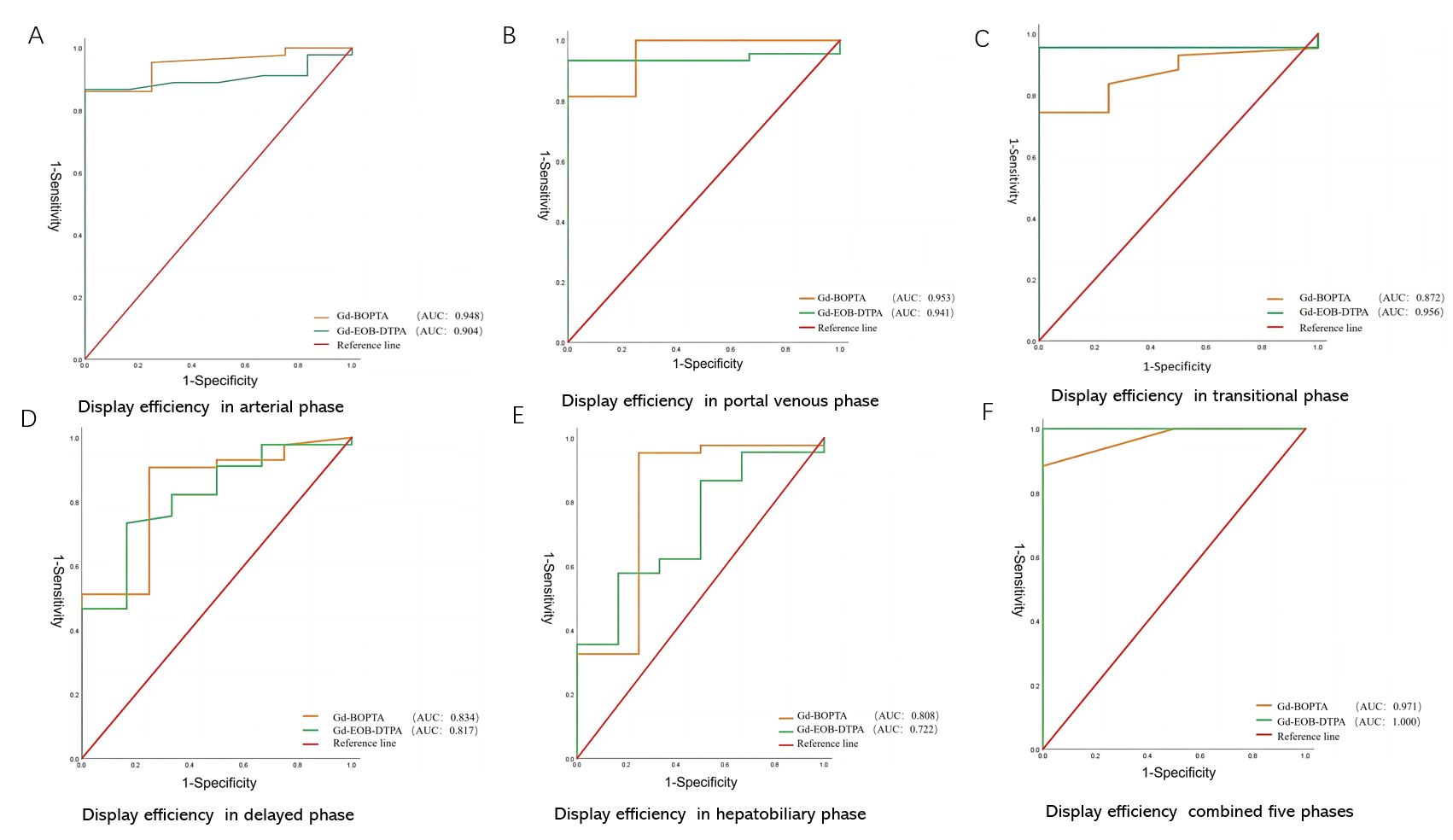
Results: Significantly varied capsule enhancement and lesion-to-liver contrast were observed in specific phases. Both agents demonstrated effective display capabilities (AUC>0.750) and excellent overall performance (AUC>0.950) across all phases.
Impact: These findings offer crucial insights for clinicians and researchers, facilitating informed selection of contrast agents for accurate HCC diagnosis. Future investigations may focus on refining imaging protocols, ultimately improving patient care and management decisions.
Introduction
Primary hepatic carcinoma (PHC) is the fourth most prevalent malignancy in China, contributing significantly to cancer-related mortality. Hepatocellular carcinoma (HCC), the primary type of PHC, poses a global health challenge with escalating incidence and mortality rates annually.Detecting early-stage HCC remains challenging due to the lack of specific symptoms, emphasizing the critical role of magnetic resonance imaging (MRI) . Gadobenate dimeglumine (Gd-BOPTA) and gadolinium ethoxybenzyl dimeglumine (Gd-EOB-DTPA) are the common contrast agents, with superior diagnostic potential over nonspecific dynamic enhanced MR.The Liver Imaging Reporting and Data System (LI-RADS 2018v) highlights nonrim arterial hyperenhancement (nonrim APHE), capsule enhancement, and nonperipheral washout as essential diagnostic features for HCC This study aims to evaluate the capabilities of Gd-BOPTA and Gd-EOB-DTPA in showcasing these features, thereby aiding in better contrast agent selection for clinical use.Methods
2.1. Patients:The study, approved by the Institutional Review Board, included 89 patients diagnosed with PHC confirmed as HCC by pathology. Exclusions comprised 187 biopsy-only cases, 39 patients with only extracellular contrast MR, and 190 patients with only enhanced CT. Multifocal liver cancer cases were evaluated for distinct pathological grades. Ninety-eight lesions were analyzed.2.2. MRI:Liver MRI was conducted using 3.0 T or 1.5 T scanners with a standardized protocol, including various sequences for imaging.
2.3. Image Analysis:Two radiologists with 16 and 6 years of experience manually measured regions of interest. Lesion-to-liver contrast (LLC) was computed, and lesion visibility was assessed in five enhancement phases. A third radiologist intervened in case of discrepancies.
2.4. Histopathologic Diagnosis:Histopathological analysis served as the reference for lesion diagnosis.
2.5. Statistical Analysis:Descriptive data were presented as percentages. Statistical tests, including the independent sample t-test and rank-sum test, were used for data analysis. SPSS version 26 was employed, and a P-value < 0.05 was considered significant. The efficiency of Gd-BOPTA-MR and Gd-EOB-DTPA-MR for HCC was evaluated via receiver operating characteristic (ROC) curve analysis.
Results
3.1. Patients and Lesions:Among 81 patients, 51.9% (42 patients) underwent Gd-EOB-DTPA-MR examination, averaging 55.45 years (SD 12.28). Of these, 40 had a chronic hepatitis history, and 24 showed elevated alpha-fetoprotein (AFP) levels. The remaining 48.1% (39 patients) underwent Gd-BOPTA-MR examination, with an average age of 56.95 years (SD 10.51). Chronic hepatitis history was present in 34 patients, and 24 patients exhibited elevated AFP levels. The Mann‒Whitney U test indicated no significant differences in the pathological and clinical liver function grading of the 106 lesions between the two groups (P>0.05) (Table 2).3.2. Imaging Features of HCC:
3.2.1. Capsule Enhancement:Significant disparities were observed between the two contrast agents (P<0.05) according to the Mann‒Whitney U test.
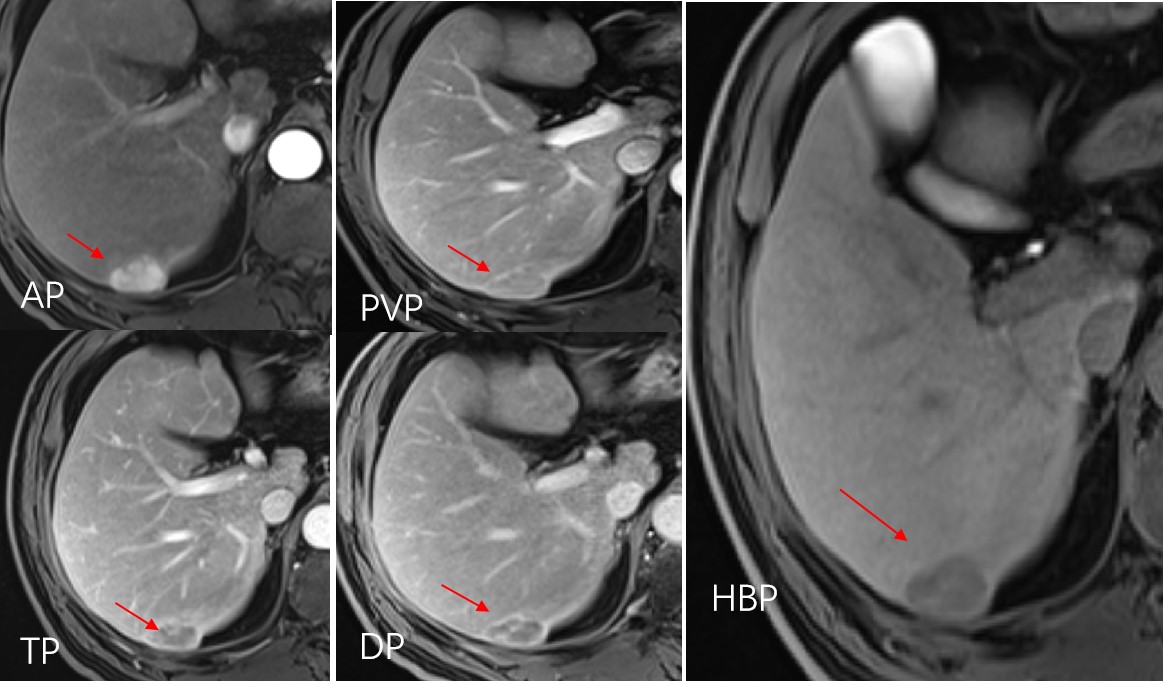
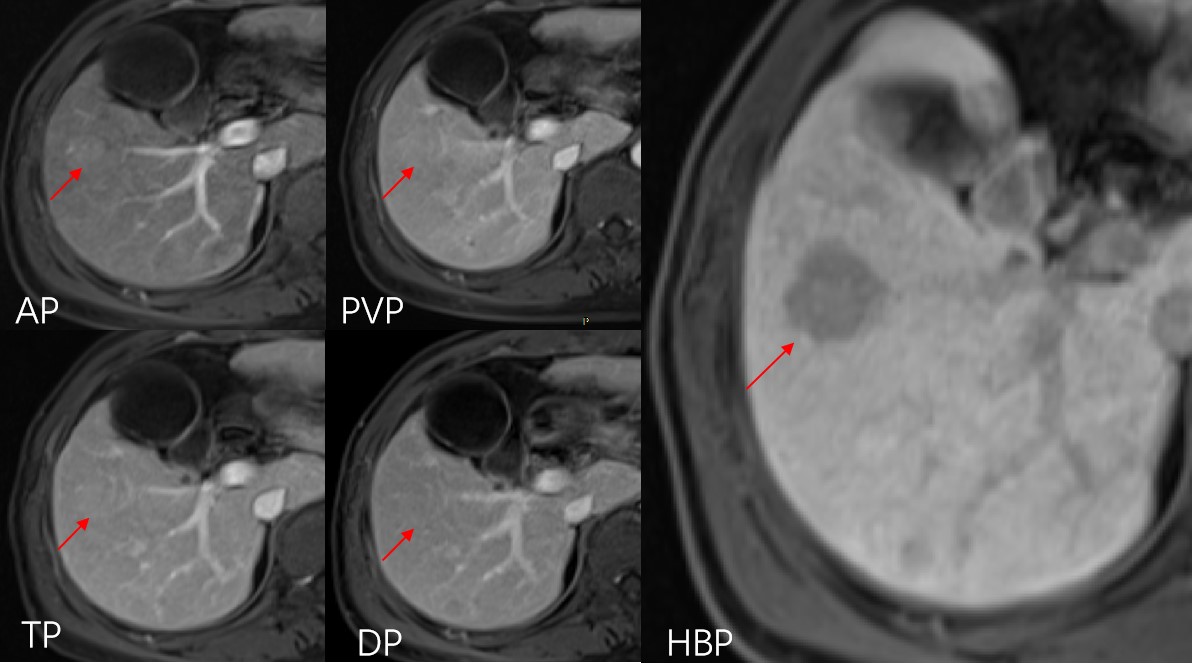
3.2.2. Lesion-to-Liver Contrast (LLC):For the LLC, the Mann‒Whitney U test revealed no significant difference during the TP and HBP phases between Gd-BOPTA MR and Gd-EOB-DTPA MR. However, significant differences were noted in the LLC during other dynamic enhancement phases and Figs 1 and 2. ROC curve analysis demonstrated differences in display efficiency between Gd-EOB-DTPA MR and Gd-BOPTA MR in terms of the LLC, as depicted in Fig 3. Excellent interobserver agreement was evident, with intra/interclass correlation coefficients (ICCs) exceeding 0.80.
Discussion
Capsule enhancement, observed in 43% to 64% of HCC cases, features both normal and pseudocapsules, composed of sinusoids, fibrosis, or a combination. Typically visible in PVP or TP/DP images, it appears as a smooth, uniform boundary encircling the lesion. Our study demonstrated an incidence of enhanced capsules at approximately 47% (46/98), with Gd-BOPTA-MR displaying significantly better visibility (76%) than Gd-EOB-DTPA-MR (20%), aligning with earlier research. Pharmacokinetic discrepancies contribute to this difference, as Gd-BOPTA exhibits lower hepatocyte uptake (3-5%) compared to Gd-EOB-DTPA (50%), leading to faster and higher liver parenchyma signal enhancement for Gd-EOB-DTPA. Additionally, the higher dose of BOPTA may contribute to enhanced capsule visibility.Regarding nonrim APHE and nonperipheral "washout," significant differences were observed in LLC between Gd-BOPTA and Gd-EOB-DTPA during dynamic enhancement in the arterial phase (AP), likely due to variations in pharmacokinetics and acquisition time. Differences in LLC during PVP and DP were also noted, influenced by the contrast agents' pharmacokinetics and acquisition times. Both contrast agents exhibited similar LLC during the HBP phase.In summary, our study highlights the distinct capabilities of Gd-BOPTA and Gd-EOB-DTPA in displaying specific HCC features, indicating the importance of selecting the appropriate contrast agent based on individual clinical requirements.Conclusion
This study underscores the significance of choosing the appropriate contrast agent for accurate HCC diagnosis. The comprehensive analysis of gadobenate dimeglumine and gadolinium ethoxybenzyl dimeglumine's efficacy in displaying LI-RADS 2018v features enhances our understanding of their diagnostic utility, thus facilitating informed clinical decision-making and patient management.Acknowledgements
NoneReferences
1.Medical Administration of the State Health Commission of the People's Republic of China. Standardization for diagnosis and treatment of hepatocellular carcinoma (2022 edition) [J]. Chinese Journal of Liver Diseases, 2022, 30(4): 367-388.
2. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2019, 394(10204): 1145-1158.
3.Bray Freddie,Ferlay Jacques,Soerjomataram Isabelle et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries.[J] .CA Cancer J Clin, 2018, 68: 394-424.
Figures