4107
Diffusion Tensor Imaging Along the Perivascular Space Index in Idiopathic Intracranial Hypertension1Department of Biomedical Engineering, University of Rochester, Rochester, NY, United States, 2Department of Imaging Sciences, University of Rochester, Rochester, NY, United States, 3Department of Neurology, University of Rochester, Rochester, NY, United States, 4Department of Electrical and Computer Engineering, University of Rochester, Rochester, NY, United States, 5Department of Physics and Astronomy, University of Rochester, Rochester, NY, United States
Synopsis
Keywords: Biomarkers, Diffusion/other diffusion imaging techniques, Idiopathic Intracranial Hypertension, DTI-ALPS
Motivation: Idiopathic intracranial hypertension (IIH) is caused by elevated intracranial pressure of unknown etiology. In recent years, growing evidence has suggested that impaired glymphatic clearance may mediate IIH pathogenesis.
Goal(s): We hypothesized that individuals with IIH would exhibit impaired glymphatic outflow, which could be directly measured using diffusion tensor imaging along the perivascular space (DTI-ALPS).
Approach: This work used DTI-ALPS to investigate glymphatic clearance in individuals with IIH, and its association with symptom severity and comorbidities.
Results: Impaired glymphatic clearance was directly related to the clinical severity of IIH, as suggested by a lower DTI-ALPS index.
Impact: We employed perivascular diffusion tensor imaging to study glymphatic flow in IIH patients. Lower ALPS index correlated with greater clinical severity, offering insights into IIH's pathomechanism and its potential for diagnosis and treatment evaluation.
Introduction
Idiopathic intracranial hypertension (IIH) is a clinical diagnosis characterized by symptoms caused by elevated intracranial pressure (ICP), such as headache and visual disturbances1. However, the pathophysiology of IIH remains poorly elucidated. Proposed mechanisms, such as CSF hypersecretion2 and reduced CSF absorption via arachnoid granulations3, cannot fully explain symptom severity or disease onset. Recent evidence suggests that impaired glymphatic outflow may be responsible for IIH4. The glymphatic system is a pathway within the brain for fluid transport and waste clearance between the subarachnoid cerebrospinal fluid (CSF) and interstitial fluid (ISF) via the venous sinuses5. However, further human research is needed to establish a definitive association between IIH and impaired glymphatic clearance. Diffusion tensor imaging along the perivascular space (DTI-ALPS) is a non-invasive imaging method that serves as a proxy to quantify the degree of glymphatic clearance along the perivascular space6. This work used DTI-ALPS to investigate glymphatic clearance in a cohort of patients with IIH and its relationship with clinical severity and comorbidities.Methods
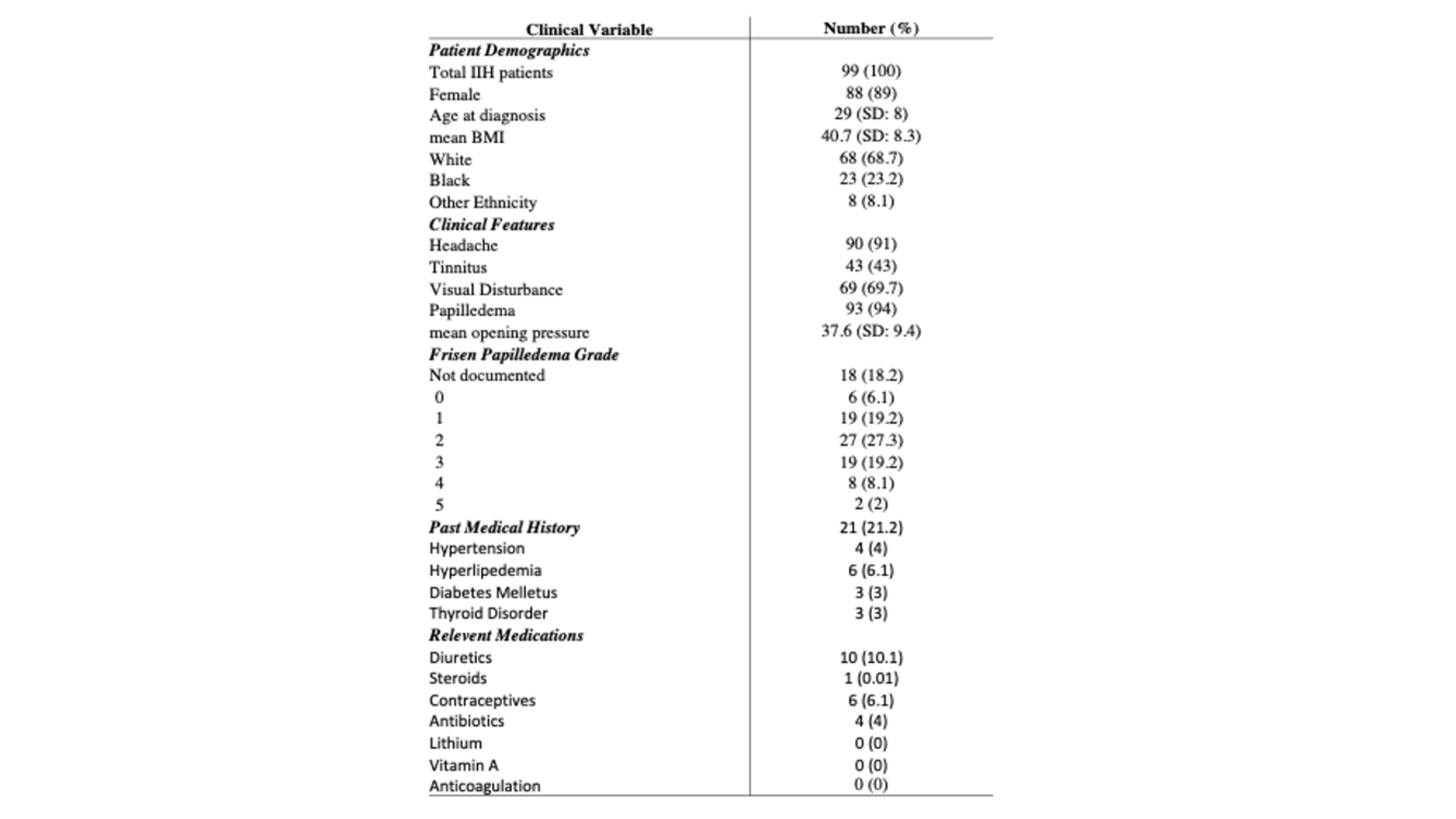
Cohort: 99 patients with clinically diagnosed IIH were retrospectively identified. All subjects had previously undergone MRI as part of a standardized MRI protocol, including structural T1w imaging and diffusion-weighted imaging (DWI) with either 12 or 14 directions. Controls (n=6)were identified as those with no significant medical history, including no history of chronic headaches, and had normal brain MRIs. IIH patients clinical characteristics and their Frisen papilledema grade and lumbar puncture opening pressure (OP) were collected at their initial presentation.Image Acquisition: All images were acquired on a 3T GE Discovery 750 MRI system (GE Healthcare, Milwaukee, WI, USA) with an 8-channel head coil. Anatomical T1w imaging and DTI was acquired with protocol consisting of 12 or 14 directions with b=1000 s/mm2 and 4 b=0 reference images.
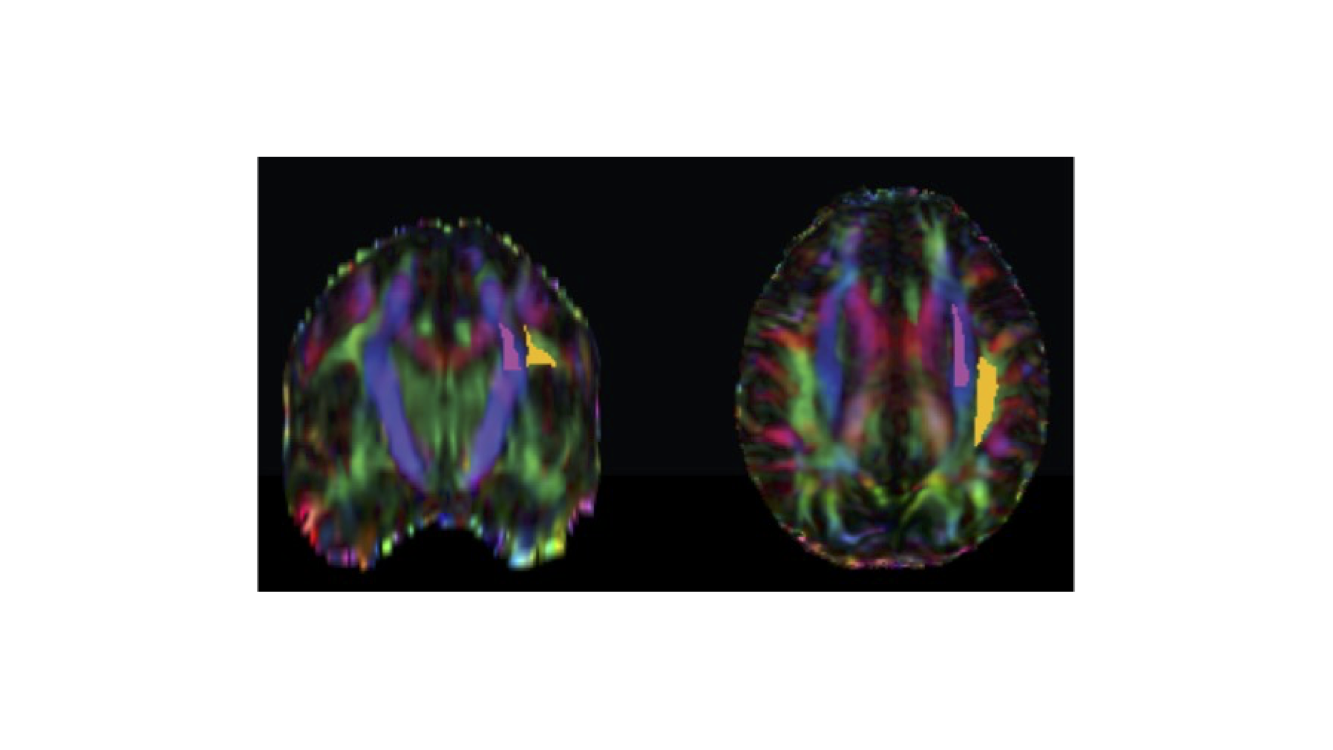
MRI Analysis: All DWI data were corrected for eddy current-induced distortion using EDDY_CORRECT in FSL7, and susceptibility-induced distortion was corrected using the INVERSION algorithm consisting of inverse contrast normalization of T1w data and diffeomorphic co-registration using symmetric normalization8 in ANTs9. Diffusivity maps along the x-axis (Dxx), y-axis (Dyy) and z-axis (Dzz) were computed in addition to fractional anisotropy (FA) using DIPY. All maps were co-registered to the FA map template FMRIB58 using ANTs9. Modified JHU ICBM white matter labels were used for the projection (superior corona radiata) and association (superior longitudinal fasciculus) fibers in the periventricular area (Figure 1). The ALPS index was then defined accordingly:
$$ALPS index = \frac{mean(Dxx_{proj}, Dxx_{assoc})}{mean(Dyy_{proj},Dzz_{assoc})}$$
Statistical Analysis:
Correlations among continuous variables (opening pressure, Frisen papilledema grade, and ALPS index) were perform using linear regression. An unpaired, two-tailed t-test or one-way ANOVA were used to assess differences between and among groups. All statistical analyses were completed using R: A language and environment for statistical computing (R Foundation for Statistical Computing, Vienna, Austria. URL: https://www.R-project.org/).
Results
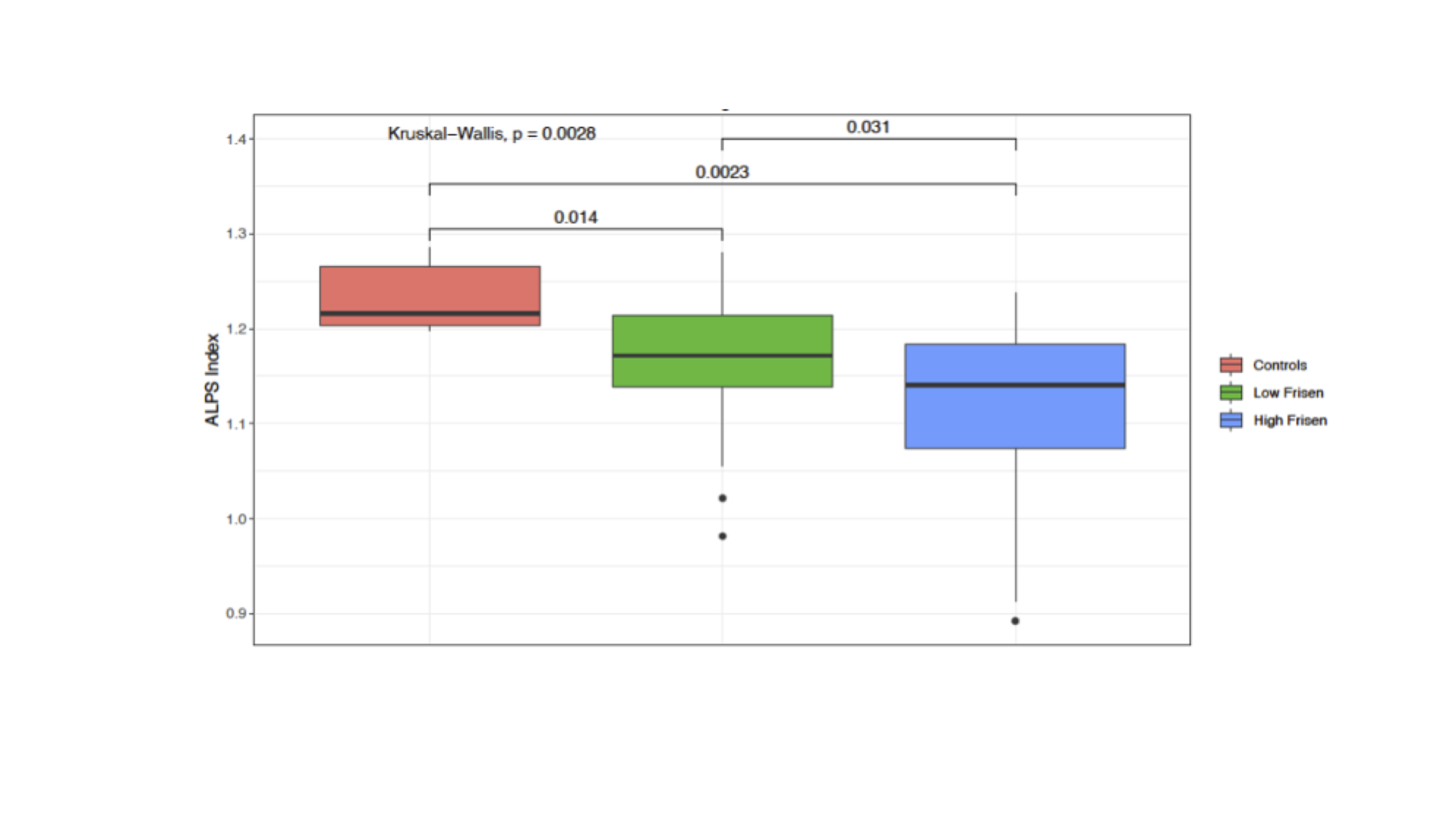
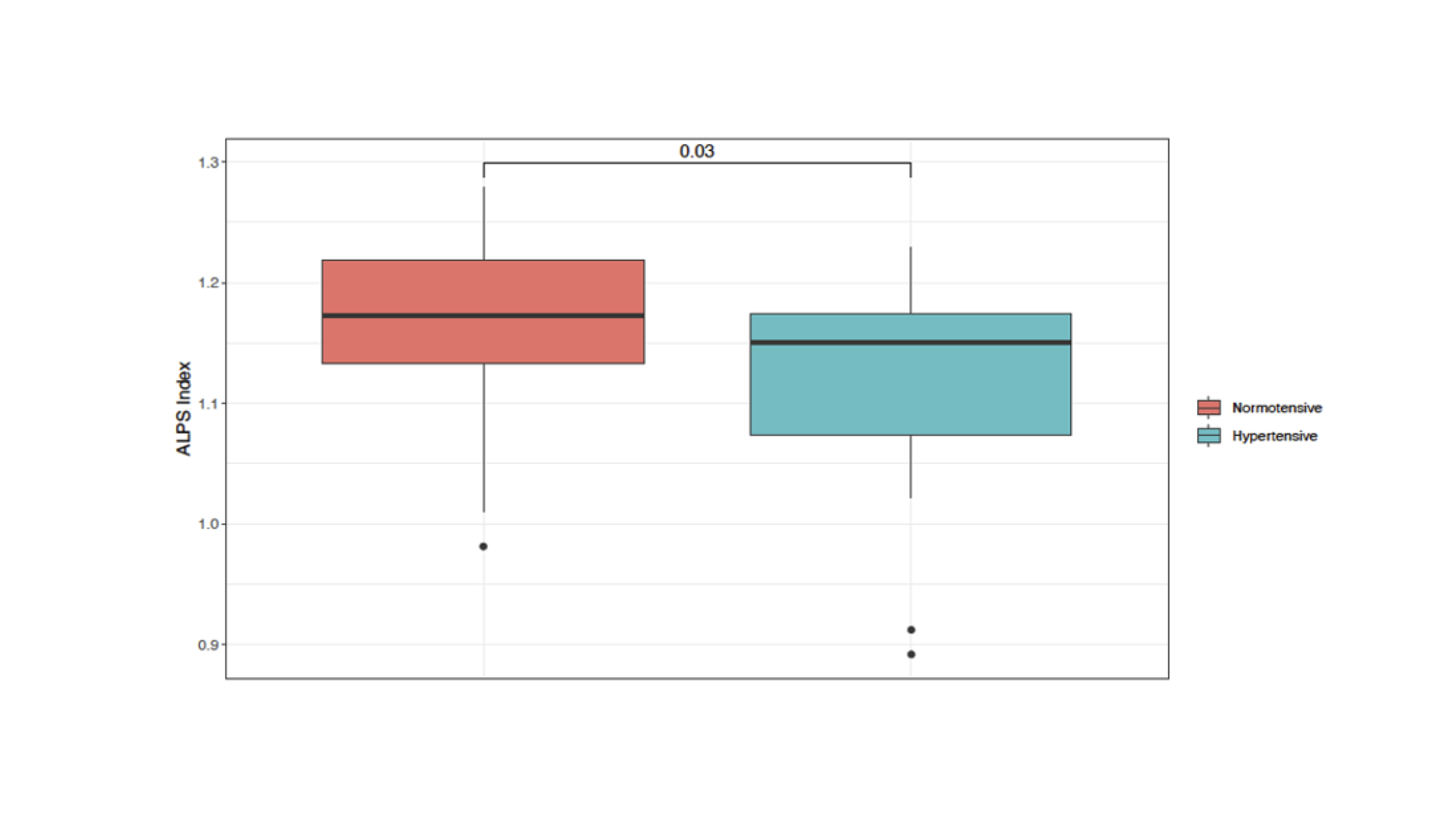
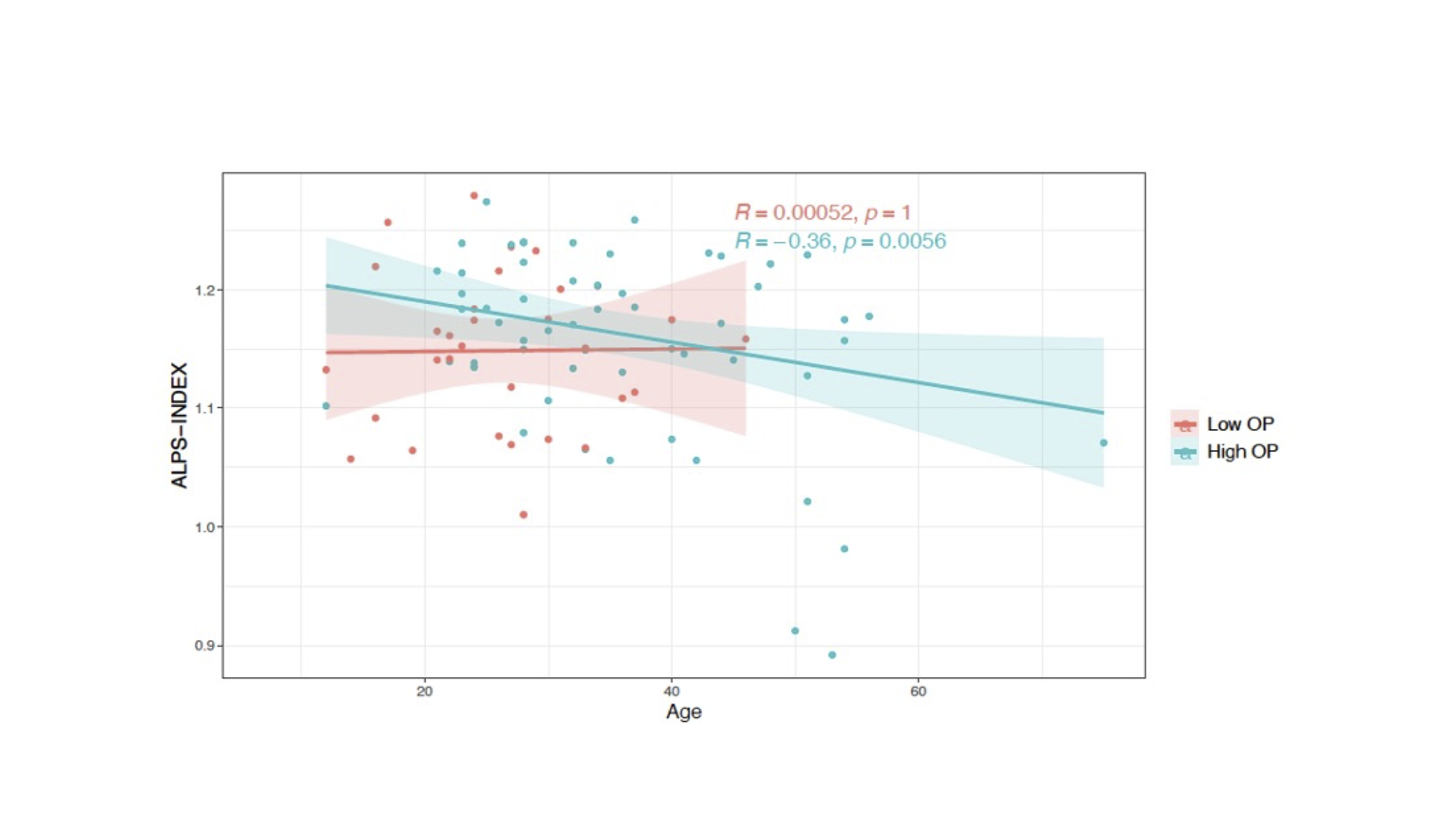
Clinical characteristics are summarized in Figure 2. Additionally, Individuals with IIH were stratified to those with low grade (Frisen grade 0-2) and high grade (Frisen grade 3-5) papilledema. The ALPS index of the control group was significantly higher than IIH patients with either low- or high-grade papilledema. Furthermore, those with high-grade papilledema had a significantly lower ALPS index than those with low grade papilledema (Figure 3). Moreover, we observed a significantly lower ALPS index in patients with IIH who also had a history of hypertension (Figure 4). Further, an interaction between age and opening pressure exists in individuals with IIH (Figure 5).Discussion
This work used the DTI-ALPS index to evaluate the relationship between glymphatic outflow in individuals with IIH and clinical severity. In general, we found that individuals with IIH had significantly lower glymphatic clearance as measured using the ALPS index compared with controls, and that glymphatic clearance was further impaired in those with high-grade papilledema compared to those with low-grade (p=0.031). Additionally, we observed that individuals with IIH with a history of hypertension had poorer glymphatic clearance than those with IIH and no history of hypertension (p=0.03). While obesity is an independent risk factor for IIH and hypertension, and often seen with both, this association suggests that hypertension may further contribute to elevated ICP, thereby worsening glymphatic outflow. The ALPS index was also significantly correlated with age in individuals with IIH and high lumbar puncture opening pressure (p=0.0056), but not in those with low opening pressure (p=1).Conclusion
This work utilized the DTI-ALPS index to investigate the association between IIH and glymphatic outflow and its association with clinical severity and comorbid conditions. In general, impaired glymphatic clearance was observed in those with IIH and was directly associated with the degree of disease severity.Acknowledgements
No acknowledgement found.References
1. Markey KA, Mollan SP, Jensen RH, Sinclair AJ. Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol. Jan 2016;15(1):78-91. doi:10.1016/S1474-4422(15)00298-7
2. Iencean SM. Simultaneous hypersecretion of CSF and of brain interstitial fluid causes idiopathic intracranial hypertension. Med Hypotheses. Nov-Dec 2003;61(5-6):529-32. doi:10.1016/s0306-9877(03)00209-3
3. Boulton M, Armstrong D, Flessner M, Hay J, Szalai JP, Johnston M. Raised intracranial pressure increases CSF drainage through arachnoid villi and extracranial lymphatics. Am J Physiol. Sep 1998;275(3):R889-96. doi:10.1152/ajpregu.1998.275.3.R889
4. Steinruecke M, Tiefenbach J, Park JJ, Kaliaperumal C. Role of the glymphatic system in idiopathic intracranial hypertension. Clin Neurol Neurosurg. Nov 2022;222:107446. doi:10.1016/j.clineuro.2022.107446
5. Jessen NA, Munk AS, Lundgaard I, Nedergaard M. The Glymphatic System: A Beginner's Guide. Neurochem Res. Dec 2015;40(12):2583-99. doi:10.1007/s11064-015-1581-6
6. Taoka T, Masutani Y, Kawai H, et al. Evaluation of glymphatic system activity with the diffusion MR technique: diffusion tensor image analysis along the perivascular space (DTI-ALPS) in Alzheimer's disease cases. Jpn J Radiol. Apr 2017;35(4):172-178. doi:10.1007/s11604-017-0617-z
7. Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM. Fsl. Neuroimage. Aug 15 2012;62(2):782-90. doi:10.1016/j.neuroimage.2011.09.015
8. Bhushan C, Haldar JP, Choi S, Joshi AA, Shattuck DW, Leahy RM. Co-registration and distortion correction of diffusion and anatomical images based on inverse contrast normalization. Neuroimage. Jul 15 2015;115:269-80. doi:10.1016/j.neuroimage.2015.03.050
9. Avants B, Tustison N, Song G. Advanced normalization tools (ANTS). Insight J. 11/30 2008;1–35doi:10.54294/uvnhin
Figures