4101
Adiabatic pulses for outer volume suppression in non-contrast coronary Magnetic Resonance Angiography1TU Delft, Delft, Netherlands, 2LUMC, Leiden, Netherlands, 3HollandPTC, Delft, Netherlands
Synopsis
Keywords: RF Pulse Design & Fields, Cardiovascular
Motivation: Large field-of-views in body imaging, e.g. coronary magnetic resonance angiography (MRA), are a limiting factor for short scan times, but this can be mitigated with outer volume suppression (OVS) and high parallel imaging acceleration rates.
Goal(s): Evaluate the use of adiabatic pulses for OVS in accelerated coronary MRA.
Approach: Two single-band adiabatic pulses and a dual-band adiabatic (DBA) pulse were optimized in terms of stop-band flip angle and evaluated in spoiled GRE-based coronary MRA.
Results: Adiabatic pulses demonstrate thorough signal suppression in stop-bands and a significant reduction of fold-over artifacts in vivo, with DBA bearing the promise of slightly improved homogeneity.
Impact: Single and dual-band adiabatic pulses provide robust outer volume suppression in accelerated coronary imaging, successfully mitigating residual fold-over artifacts.
Introduction
Coronary Magnetic Resonance Angiography (MRA), is a viable alternative to CT for coronary artery stenosis assessment1. However, in coronary imaging, the volume of interest is relatively small compared to the field-of-view (FOV) that encompasses the entire chest, resulting in scan time and resolution trade-offs. To achieve smaller FOVs or high parallel imaging acceleration rates, outer volume suppression (OVS) has been proposed2. However, OVS pulse performance remains limited due to strong field inhomogeneities near the bore edge. Adiabatic RF pulses are a suitable choice due to their recognized resilience against off-resonance3. In this work, we evaluate the use of adiabatic pulses for OVS suppression in accelerated coronary MRA. Adiabatic OVS pulses are optimized in terms of stop-band flip angle (FA) and dual-band adiabatic (DBA) pulses are proposed to achieve simultaneous and homogenous suppression of signals from both sides of the heart.Methods
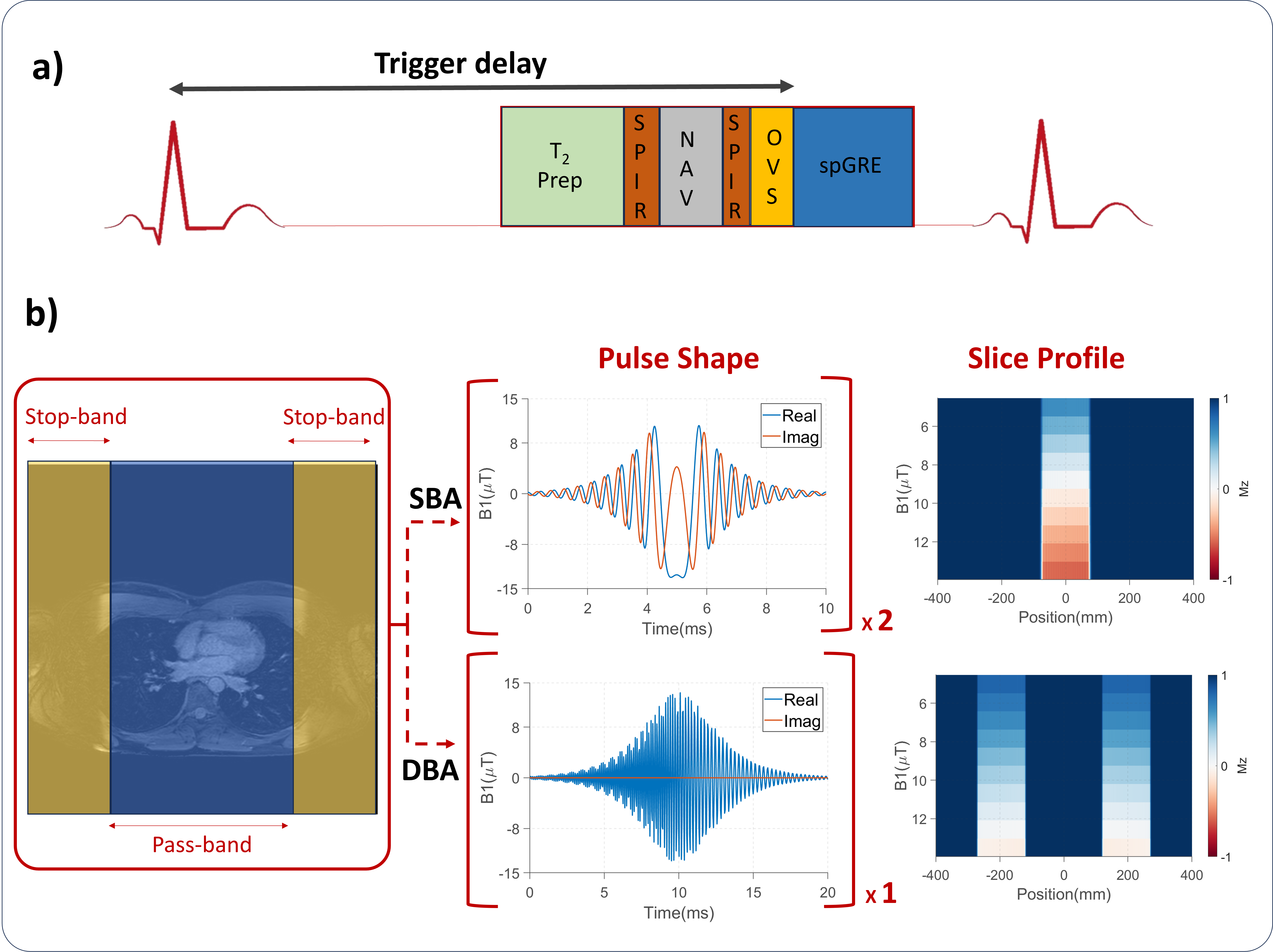
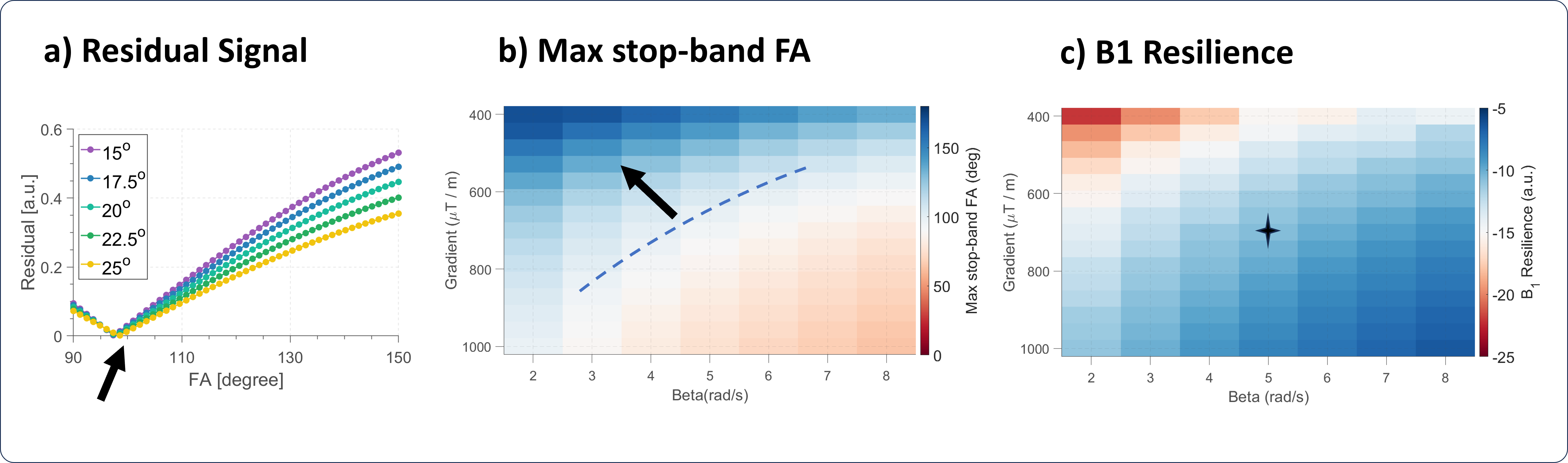
Hyperbolic secant pulses (duration=10ms; thickness=150mm) were used as stop-band for single-band adiabatic (SBA) OVS. DBA pulses were obtained by combining frequency-shifted SBA pulses with one band being time-reversed4,5 (Fig1b). The optimal OVS FA was determined based on Bloch simulations of a spoiled gradient echo (spGRE) coronary MRA sequence. For a range of pulse parameters, SBA and DBA pulse amplitudes were optimized to achieve the desired stop-band FA using single isochromat simulation6,7. With fixed timing and stop-pass band geometry, SBA and DBA pulses were characterized by two degrees of freedom: pulse shape β and the selection gradient strength. Pulse optimization was performed based on two performance criteria: 1) The maximum stop-band FA was calculated for each parameter combination, using a maximum pulse amplitude of 13.5μT; 2) B1+ resilience was determined as the slope of the stop-band FA as a function of the effective B1+ amplitude taken from single isochromat simulations evaluated at the desired stop-band FA. The optimal parameter combination was chosen to yield maximum B1+ resilience while having a maximum stop-band FA higher than the desired FA.Imaging was performed at 3T (Ingenia, Philips) using a 3D free-breathing ECG-triggered spGRE sequence (res=1.5x1.5x1.5mm3, TE/TR=1.2/4.2ms, FOV=400x400x135mm3). SENSE factors = 4/1.5 in phase- and slice-encoding, respectively with the OVS pulses being played before imaging readout (Fig1a). DBA and SBA pulses were compared in a torso-shaped ballistic gel phantom (T1=260ms) placed between two water bottles to provide a large FOV. In vivo imaging was obtained in 3 healthy subjects (2 males, 29.3±1.3y). For phantoms and in vivo, residual signal in the stop-bands was quantified relative to the signal of a reference acquisition without OVS.
Results
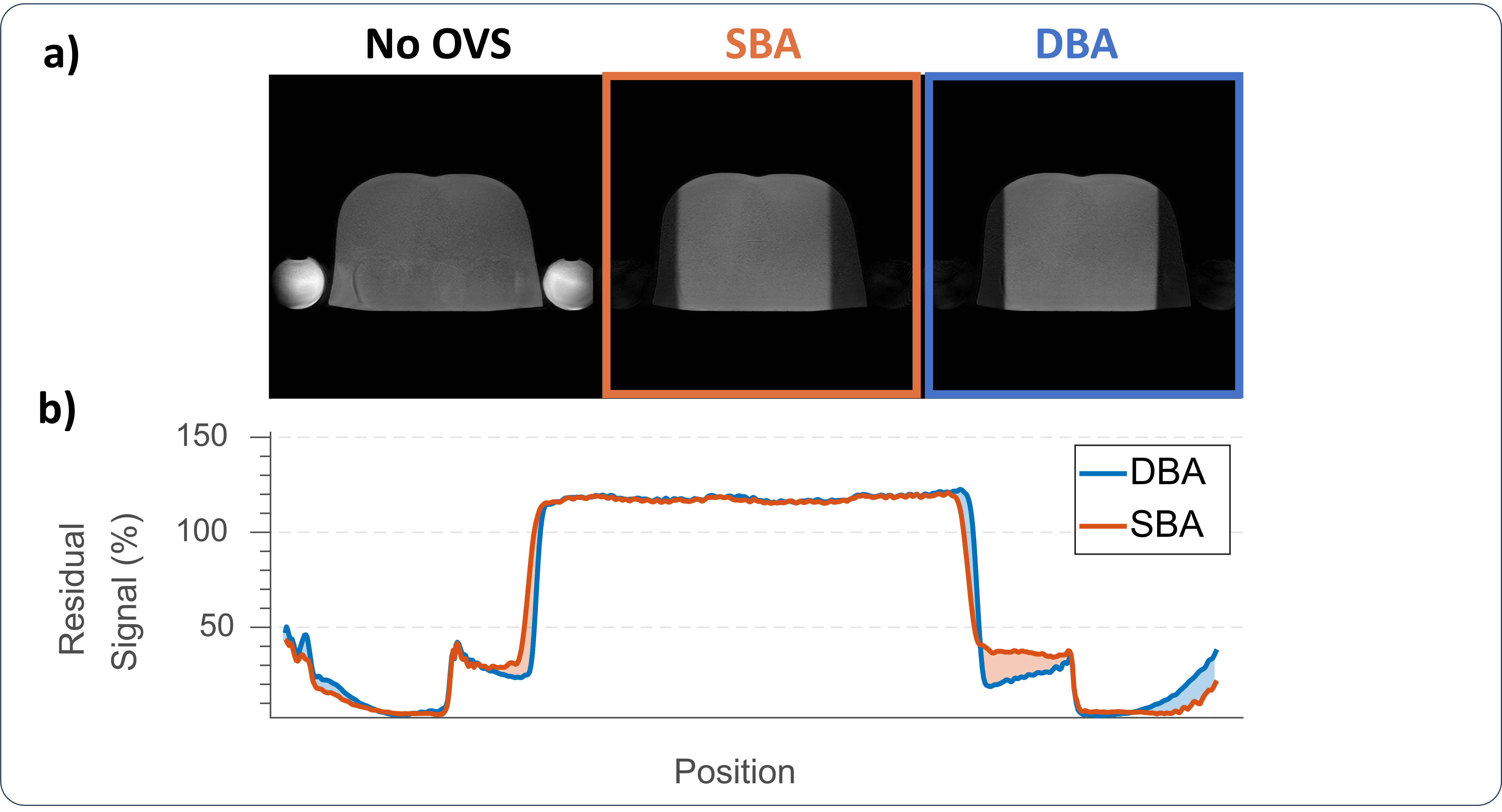
Simulations suggest minimal residual signal with stop band FA=93°in the simulated spGRE coronary MRA sequence (Fig. 2a). Additionally, the effective imaging FA results in a minor difference for the optimal stop-band FA. Higher gradient strength and higher β result in increased B1+ resilience, albeit at the expense of reduced maximum stop-band FA (Fig2b-c). To achieve the desired stop-band FA, within the B1+ limits, 700μT/m and 5rad/s were selected as the optimal parameters (Fig2c).Good suppression was obtained in the phantom for both pulses (residual signal: SBA=22.4%, DBA=19.3%). Differential relaxation, resulting from the time gap between the two stop-bands with SBA, causes slightly suboptimal suppression in the right stop-band and increased residuals compared with DBA in the torso (SBA=31.8%, DBA=17.9%) (Fig. 3).
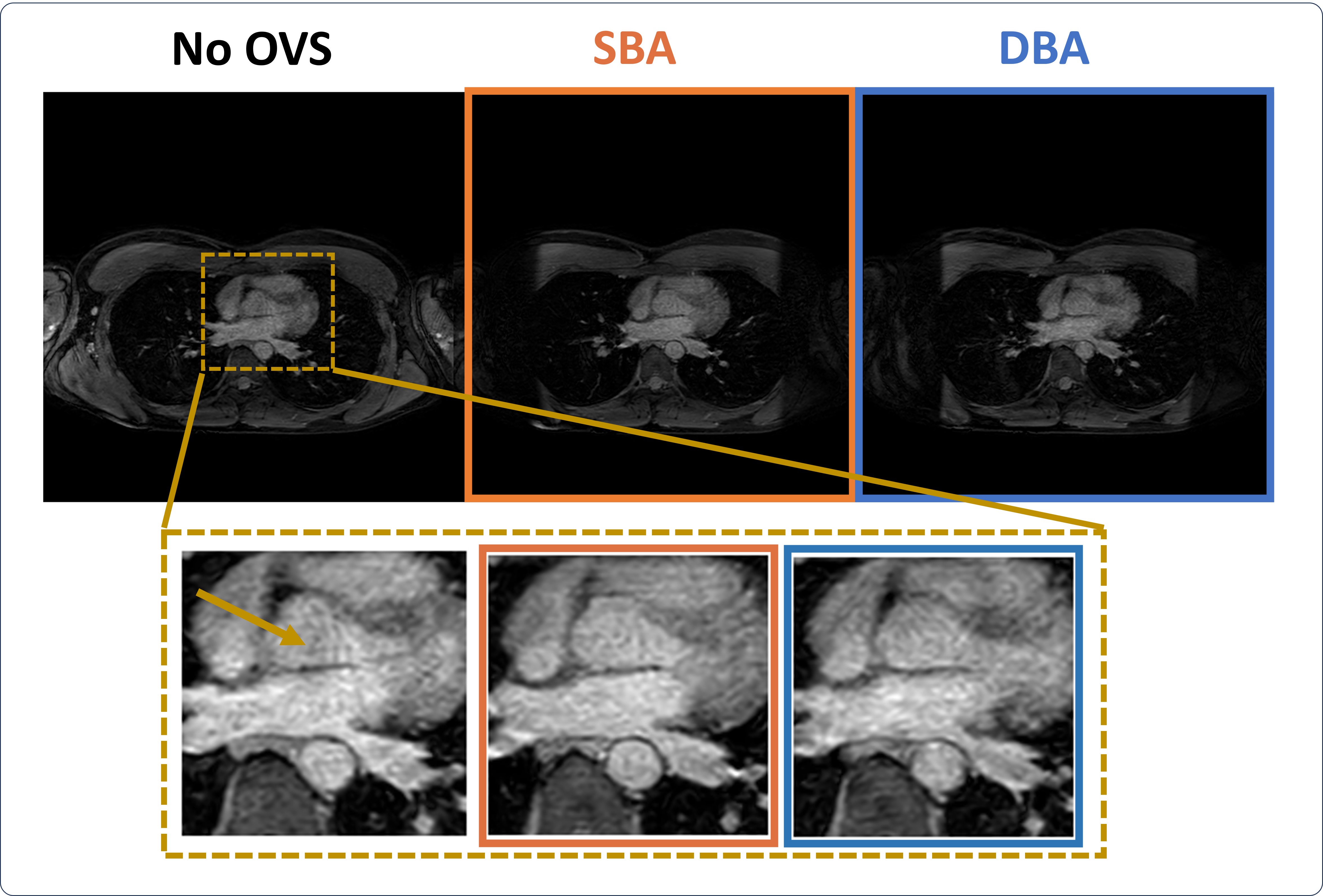
Coronary images, with high SENSE rates, using DBA and SBA show thorough suppression of the signal in the stop-bands and noticeable fold-over artifact alleviation (Fig. 4).
Discussion
Different sequence schemes require different stop-band FAs for ideal signal suppression due to a differential amount of magnetization recovery between the OVS readout and the k-space center. Thus, the readout type, the k-space ordering, the acquisition window duration, and the relaxation times of the target tissue are important factors for the ideal stop-band FA. In this work, we used Bloch simulations to tailor the stop-band FA to the proposed sequence. Driving the adiabatic pulses with low amplitudes in a sub-adiabatic regime achieved the pre-determined optimized stop-band FA. Thus, with tailored optimization, adiabatic pulses provide a promising candidate for robust OVS in cardiac MRI.Compared with SBA pulses, DBA pulses have the advantage of simultaneous suppression of both bands. This can lead to more homogenous suppression across the two bands, especially for tissues with short T1, as shown in phantom. However, large B1+ amplitudes may be required for DBA pulses, thus, the optimal pulse choice may also depend on the desired stop-band FA.
Conclusion
Adiabatic dual-band and single-band OVS pulses have shown thorough and homogenous suppression across two stop-bands, enabling the use of high parallel imaging acceleration factors in coronary MRA without fold-over artifacts.Acknowledgements
Funded by the European Union (ERC, VascularID, StG 101078711), and NWOReferences
[1] Hajhosseiny, Reza, et al. "Coronary magnetic resonance angiography: technical innovations leading us to the promised land?." Cardiovascular Imaging 13.12 (2020): 2653-2672.
[2] Le Roux, Patrick, et al. "Optimized outer volume suppression for single‐shot fast spin‐echo cardiac imaging." Journal of Magnetic Resonance Imaging 8.5 (1998): 1022-1032.
[3] Tannús, Alberto, and Michael Garwood. "Adiabatic pulses." NMR in Biomedicine: An International Journal Devoted to the Development and Application of Magnetic Resonance In Vivo 10.8 (1997).
[4] Kupce, E., and R. Freeman. "Adiabatic pulses for wideband inversion and broadband decoupling." Journal of Magnetic Resonance, Series A 115.2 (1995): 273-276.
[5] Ouwerkerk, R., and R. A. Edden. "Multi-Band Adiabatic Pulses." Seattle, WA, USA (2006): 3006.
[6] Warnking, Jan M., and G. Bruce Pike. "Bandwidth‐modulated adiabatic RF pulses for uniform selective saturation and inversion." Magnetic Resonance in Medicine[7]Abo Seada, Samy, et al. "Optimized amplitude modulated multiband RF pulse design." Magnetic resonance in medicine 78.6 (2017): 2185-2193.
Figures