4093
Redesigning Parallel-transmit Pulses in Runtime to Correct for the Effect of Patient Motion on B1+-maps for Ultrahigh-field MRI.1CUBRIC, School of Psychology, Cardiff University, Cardiff, United Kingdom
Synopsis
Keywords: RF Pulse Design & Fields, High-Field MRI, motion
Motivation: Low-field motion-tracking methods are insufficient at ultrahigh-field as motion also affects flip-angle .
Goal(s): Our goal was to develop a method that can redesign pulses for ultrahigh-field MRI within 1 second.
Approach: We implemented a method to rapidly recalculate the post-motion basis-functions needed for pulse design and complemented it with dictionary matching to reduce pulse computation times a of small-tip-angle multi-spoke multi-slice parallel-transmit pulse design method.
Results: With basis-functions recalculated in 0.13 seconds/slice and pulses reoptimized in 0.18 seconds/slice, multi-slice multi-spoke parallel-transmit pulses can be redesigned in runtime using the proposed method. Redesigned pulses significantly reduce motion-induced error, yielding consistent excitation with pre-motion excitation.
Impact: A pulse design method is developed that can redesign practical parallel-transmit pulses in under a second. It can correct for motion-related flip angle distortions at ultrahigh-field and will help facilitate scanning of patients who cannot remain still (e.g., paediatric, dementia).
Introduction
Ultrahigh-field (UHF-) MRI suffers from artificial contrast variations due to the wavelength being comparable to body dimensions. Parallel-transmit (pTx) pulses can mitigate these variations and achieve homogeneous excitation1-3. However, pTx pulses are highly sensitive to patient motion4. With several patient populations (e.g., paediatric5-8, Parkinson’s9, Alzheimer’s10), extended scan durations11 may become intolerable, requiring sedation. Because sedatives may have side effects, even requiring hospital admittance in some cases5-7, it is necessary to solve patient motion at the sequence level. Although numerous methods exist to track and correct patient motion at lower field strengths12-17, pTx pulses also need to be redesigned to recover excitation homogeneity after motion for UHF-MRI. This study proposes a method that can redesign pTx pulses in under a second for patient-motion-corrected pTx pulse redesign during the scan.Methods
Ref.18 proposed splitting the pulse design problem into two stages. In the precomputation stage, all relevant definitions were initialized, slice-selective pulse dictionaries were generated for satisfying SAR and system limits, spatial encoding functions (SEFs) that characterize the spatial variations generated by the gradients and the RF coils were prepopulated. In runtime, spokes were selected and channel-weights were optimized using an adaptation of the Spatial Domain Method19, MPgCG-pTx20,21, SAR and system limits were enforced, and pulses were written in a scanner-readable format. While the method could design practical initial pulses in under a second, pulses could not be redesigned due to three reasons:- Problem-1: Patient motion affects B1+-maps, and therefore, the basis-functions of the optimisation problem (SEFs). This change cannot be calculated or experimentally measured.
- Problem-2: The precomputations in Ref.18, which included generating the SEFs, took ~2.2 seconds per simultaneously-excited slice, making redesigning the pulses infeasible.
- Problem-3: The method did not have B0 off-resonance correction.
This study proposes using the deep learning method developed in Ref.22 to estimate the motion-related changes in B1+-maps from centred measurements to address Problem-1. While loading the networks onto the GPUs takes ~0.5 seconds, this step can be done before runtime, and therefore, does not affect pulse redesign. Then, B1+-maps are estimated during runtime (<0.05 seconds), downsampled from 256x256 (network output) to desired resolution and converted to SEFs (~0.13 seconds/slice). B0 off-resonance correction is performed by incorporating the phase evolution between the temporal-centres of each spoke into the SEFs using the spoke length of the initial pulse as reference. During pulse design, spokes are selected and channel weights are optimized from scratch using MPgCG-pTx. To enforce SAR and system limits, precomputed dictionaries are used to select slice-selective pulse envelopes. Pulse waveforms are written into scanner-readable files to complete runtime (Figure 1).
The effect of number of spokes, simultaneously-excited slices (SMS), virtual observation points23, candidate spokes in k-space, coils; resolution; B0 off-resonance correction; and SAR reduction method on computation time was investigated. Monte-Carlo simulations were performed on a 64-bit computer with Intel Skylake-Architecture (2015) i7-6700 CPU and 32 GB RAM with n=100 runs/case. 50% of cases were retrospectively discarded due to irrelevant processes competing for system resources, to investigate the performance of a dedicated system. Here, computation times exclude deep learning estimation times. A simulated example case shows the effect of rightward 10 mm motion on the excitation profile and the correction with runtime pulse redesign.
Results and Discussion
Figure 2 shows pulse redesign computation times for various pulse parameters. Pulse computation time increases quadratically with resolution and the number of spokes. Figure 3 shows that additional time required to recompute the SEFs changes weakly with number of spokes/VoPs, linearly with number of candidate-spokes/simultaneously-excited slices/coils, and quadratically with resolution.Figure 4 exemplifies the effect of rightward 10mm motion on flip angle. Pulse redesign reduces the error in magnitude (panels:D-E) and phase profiles (panels:I-J). While the global phase offset (Panel-M) can be corrected by gradient adjustments, pulse redesign reduces the spread of phase and magnitude values, thereby increasing consistency with pre-motion flip angle distribution (panels L,N).
Figure 5A-D shows that the pulse-redesign may change pulses considerably; in terms of peak local SAR (panels:A-B, difference=13%), power distribution across channels (panel:C), and the selected spokes (panel:D).
Figure 5E illustrates the effect of motion (rightward:10 mm) on the flip-angle nRMSE for pulses with 1-5 spokes and 1-5 simultaneously-excited slices, which would lead to artefacts if motion happened mid-acquisition. Redesigning the pulse yielded statistically significant (Wilcoxon signed-rank test for p=0.05) reductions in the motion-caused error across all cases. For 2+ spokes, redesigned pulses yielded very similar nRMSE values to the pre-motion excitations.
Conclusion
The proposed method can redesign practical pTx pulses (e.g., 3-spoke 3-slice) during runtime (<1 second), enabling sedative-free motion-corrected imaging for patients who cannot remain still.Acknowledgements
No acknowledgement found.References
1 Katscher, U. & Bornert, P. Parallel RF transmission in MRI. NMR Biomed 19, 393-400, doi:10.1002/nbm.1049 (2006).
2 Setsompop, K. et al. Parallel RF transmission with eight channels at 3 Tesla. Magn Reson Med 56, 1163-1171, doi:10.1002/mrm.21042 (2006).
3 Gras, V., Vignaud, A., Amadon, A., Le Bihan, D. & Boulant, N. Universal pulses: A new concept for calibration-free parallel transmission. Magn Reson Med 77, 635-643, doi:10.1002/mrm.26148 (2017).
4 Kopanoglu, E., Plumley, A. J. D., Erturk, A., Deniz, C. M. & Wise, R. G. in Proceedings of the 27th Annual Meeting of ISMRM. 4686 (2019).
5 Malviya, S. et al. Sedation and general anaesthesia in children undergoing MRI and CT: adverse events and outcomes. Br J Anaesth 84, 743-748, doi:10.1093/oxfordjournals.bja.a013586 (2000).
6 Havidich, J. E. et al. Preterm Versus Term Children: Analysis of Sedation/Anesthesia Adverse Events and Longitudinal Risk. Pediatrics 137, e20150463, doi:10.1542/peds.2015-0463 (2016).
7 Mallory, M. D., Travers, C., McCracken, C. E., Hertzog, J. & Cravero, J. P. Upper Respiratory Infections and Airway Adverse Events in Pediatric Procedural Sedation. Pediatrics 140, doi:10.1542/peds.2017-0009 (2017).
8 Boriosi, J. P., Eickhoff, J. C., Klein, K. B. & Hollman, G. A. A retrospective comparison of propofol alone to propofol in combination with dexmedetomidine for pediatric 3T MRI sedation. Paediatr Anaesth 27, 52-59, doi:10.1111/pan.13041 (2017).
9 Schwarz, S. T. et al. The 'swallow tail' appearance of the healthy nigrosome - a new accurate test of Parkinson's disease: a case-control and retrospective cross-sectional MRI study at 3T. PLoS One 9, e93814, doi:10.1371/journal.pone.0093814 (2014).
10 Prasher, V. et al. Magnetic resonance imaging, Down's syndrome and Alzheimer's disease: research and clinical implications. J Intellect Disabil Res 47, 90-100, doi:10.1046/j.1365-2788.2003.00445.x (2003).
11 Van Essen, D. C. et al. The WU-Minn Human Connectome Project: an overview. Neuroimage 80, 62-79, doi:10.1016/j.neuroimage.2013.05.041 (2013).
12 Pipe, J. G. Motion correction with PROPELLER MRI: application to head motion and free-breathing cardiac imaging. Magn Reson Med 42, 963-969, doi:10.1002/(sici)1522-2594(199911)42:5<963::aid-mrm17>3.0.co;2-l (1999).
13 Maclaren, J., Herbst, M., Speck, O. & Zaitsev, M. Prospective motion correction in brain imaging: a review. Magn Reson Med 69, 621-636, doi:10.1002/mrm.24314 (2013).
14 Wallace, T. E., Afacan, O., Waszak, M., Kober, T. & Warfield, S. K. Head motion measurement and correction using FID navigators. Magn Reson Med 81, 258-274, doi:https://doi.org/10.1002/mrm.27381 (2019).
15 Afacan, O., Wallace, T. E. & Warfield, S. K. Retrospective correction of head motion using measurements from an electromagnetic tracker. Magn Reson Med 83, 427-437, doi:https://doi.org/10.1002/mrm.27934 (2020).
16 Zaitsev, M., Dold, C., Sakas, G., Hennig, J. & Speck, O. Magnetic resonance imaging of freely moving objects: prospective real-time motion correction using an external optical motion tracking system. NeuroImage 31, 1038-1050, doi:https://doi.org/10.1016/j.neuroimage.2006.01.039 (2006).
17 Aksoy, M. et al. Real-time optical motion correction for diffusion tensor imaging. Magn Reson Med 66, 366-378, doi:https://doi.org/10.1002/mrm.22787 (2011).
18 Kopanoglu, E. in Proceedings of the Joint Meeting of ISMRM and ESMRMB. 3392 (2018).
19 Grissom, W. et al. Spatial domain method for the design of RF pulses in multicoil parallel excitation. Magn Reson Med 56, 620-629, doi:10.1002/mrm.20978 (2006).
20 Kopanoglu, E. & Constable, R. T. Radiofrequency pulse design using nonlinear gradient magnetic fields. Magn Reson Med 74, 826-839, doi:10.1002/mrm.25423 (2015).
21 Kopanoglu, E., Deniz, C. M., Erturk, M. A. & Wise, R. G. Specific absorption rate implications of within-scan patient head motion for ultra-high field MRI. Magn Reson Med 84, 2724-2738, doi:10.1002/mrm.28276 (2020).
22 Plumley, A. et al. Rigid motion-resolved B 1 + prediction using deep learning for real-time parallel-transmission pulse design. Magn Reson Med 87, 2254-2270, doi:10.1002/mrm.29132 (2022).
23 Eichfelder, G. & Gebhardt, M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med 66, 1468-1476, doi:10.1002/mrm.22927 (2011).
Figures
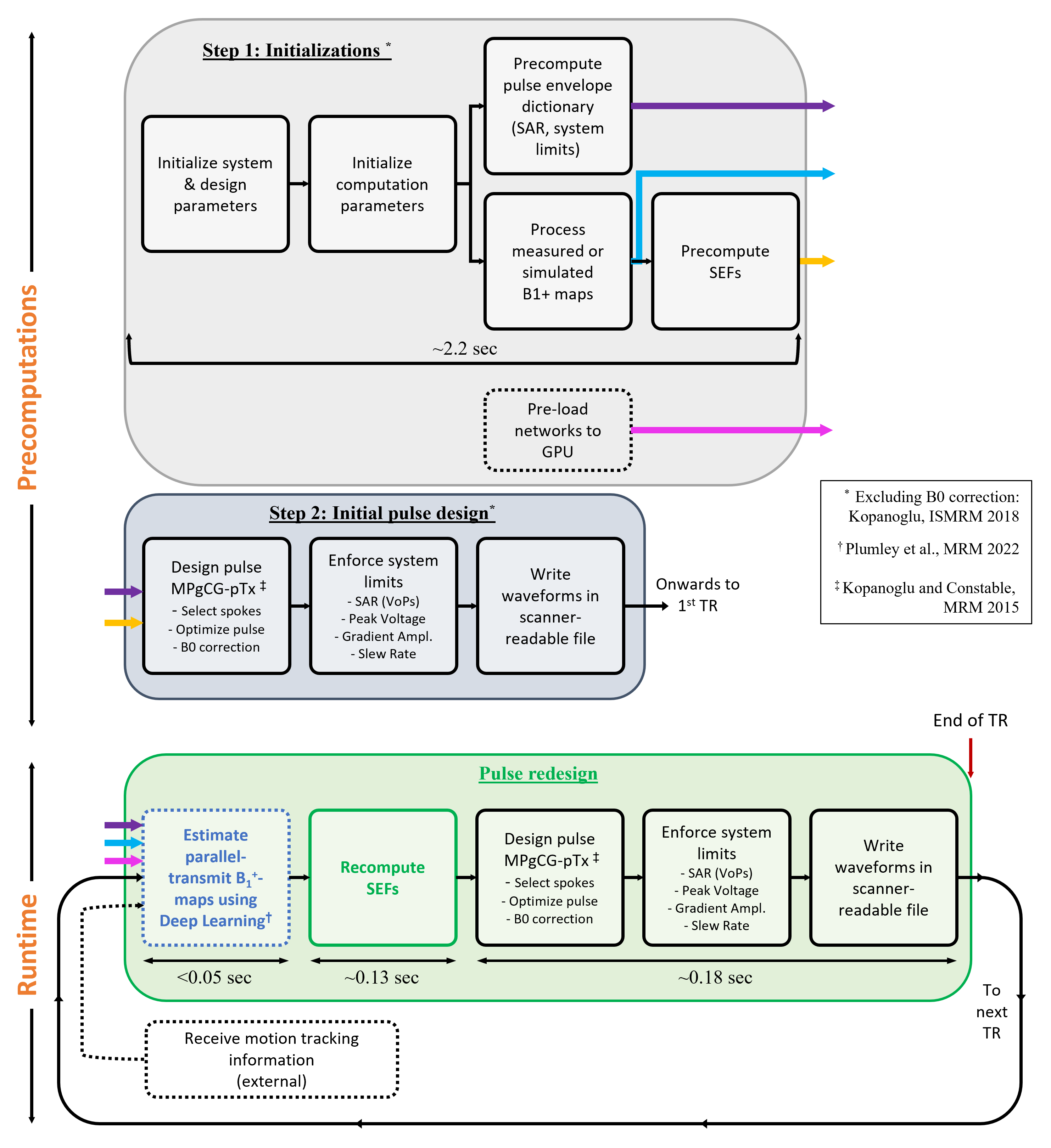
Figure 1: Proposed pulse design pipeline. In runtime SEFs are recomputed, pulses designed, system and SAR limits enforced, and waveforms written into scanner-readable format. Coloured arrows indicate data passed in/out of processes. B1+-maps are measured and processed only once (turquoise arrow). The deep learning method (developed, not yet integrated into the pipeline) can estimate post-motion B1+-maps from pre-motion B1+-maps. Listed computation times are for single-slice excitation.
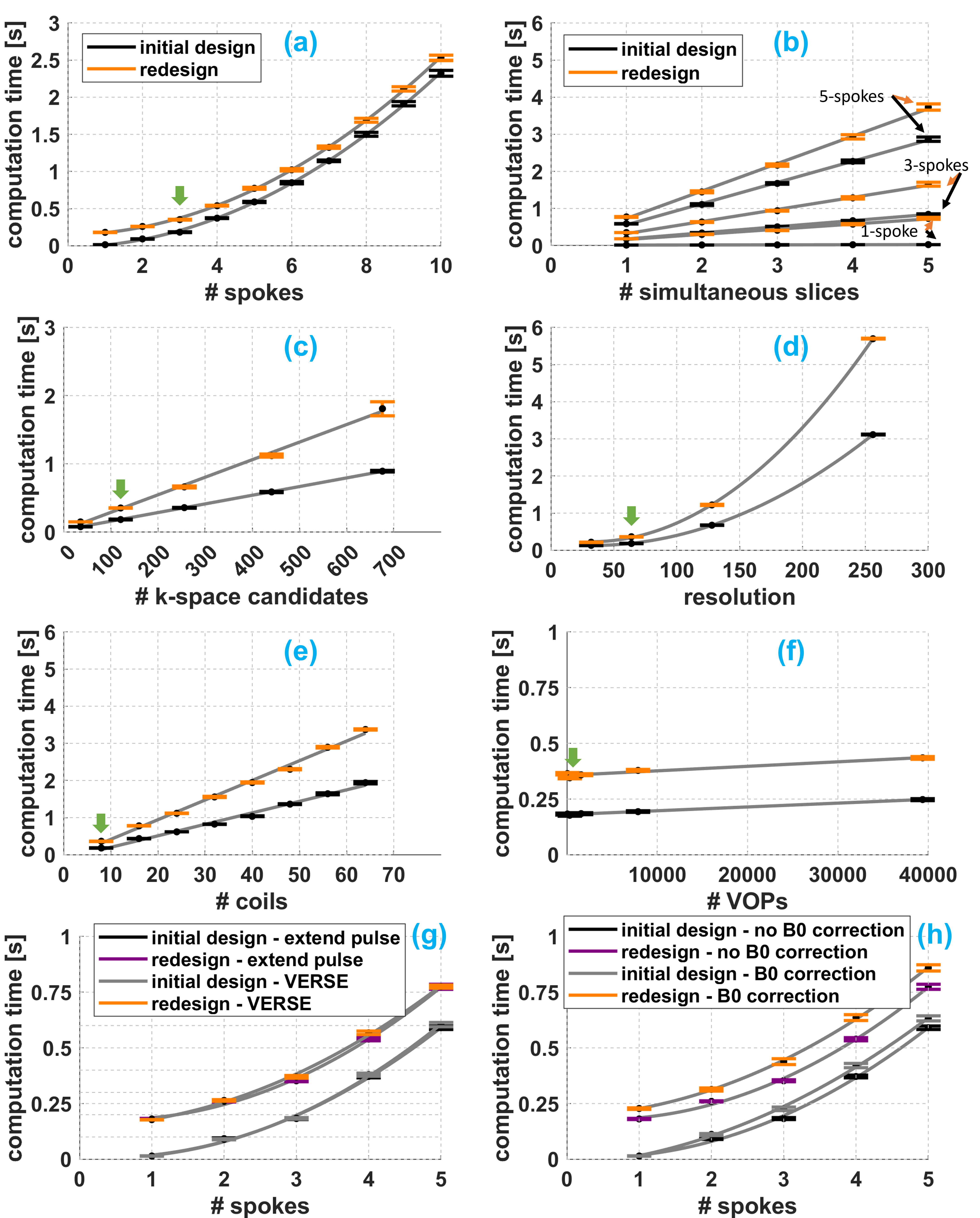
Figure 2: The effect of various pulse design parameters on pulse computation time was investigated, for the initial pulse design (black, purple) and runtime pulse redesign (orange, pink). Green arrows in panels (a)-(f) indicate the default values used for the other investigations. For an 8-channel parallel-transmit array, 3-spoke 3-slice SMS parallel-transmit pulses with VOP-informed SAR suppression via VERSE can be redesigned during the scan in <1 second.
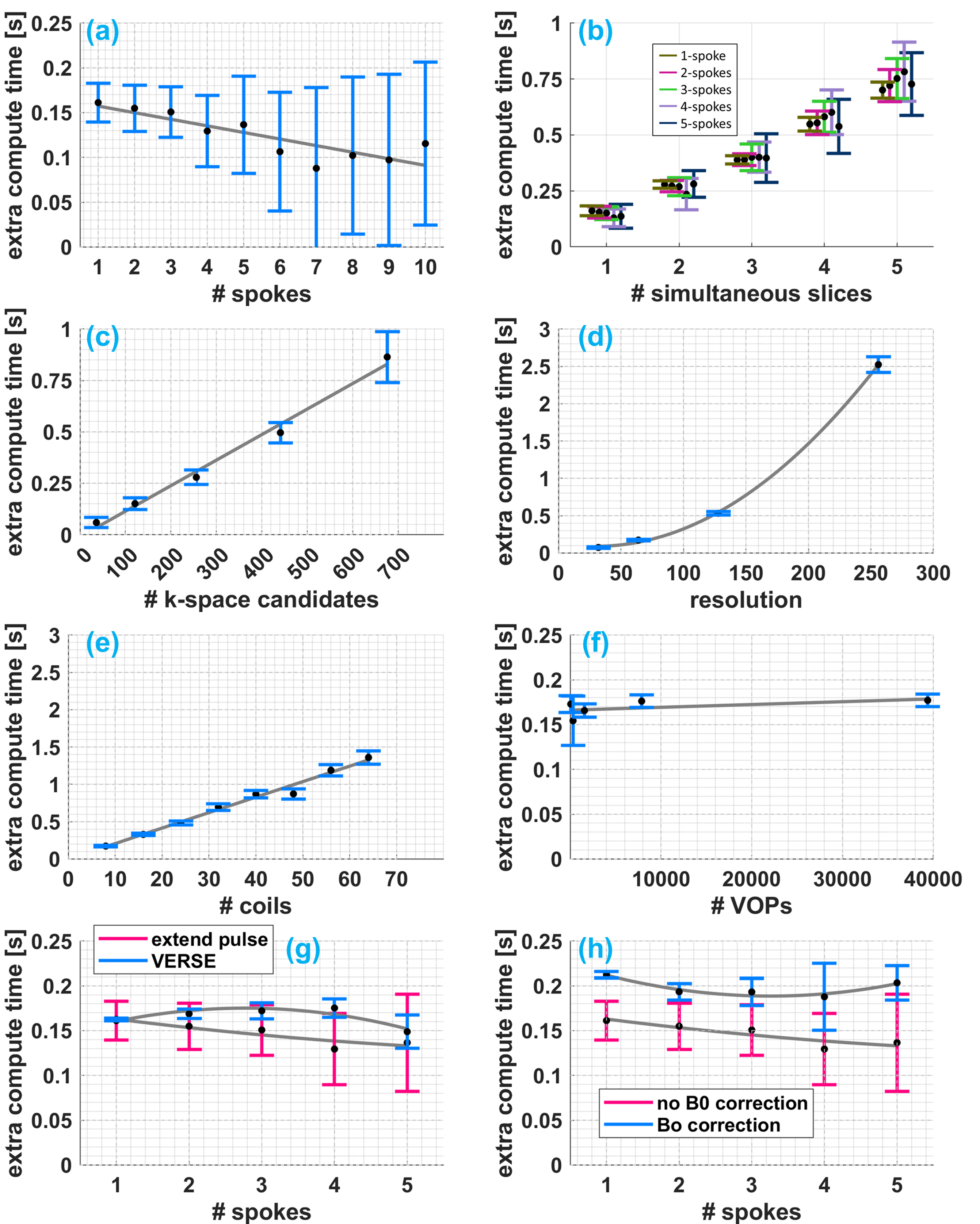
Figure 3: The additional time required to recompute the SEFs is shown with respect to various design parameters. The additional time cost has a weak dependence on the number of spokes, the number of VOPs and the SAR reduction method. B0 off-resonance correction increases pulse design time by ~0.05 seconds. The additional time cost increases linearly with number of simultaneously-excited slices (~0.13 seconds/slice), number of candidate spokes (~1.2 milli-seconds/candidate-spoke), number of coils (~0.02 seconds/coil); and quadratically with computation resolution.
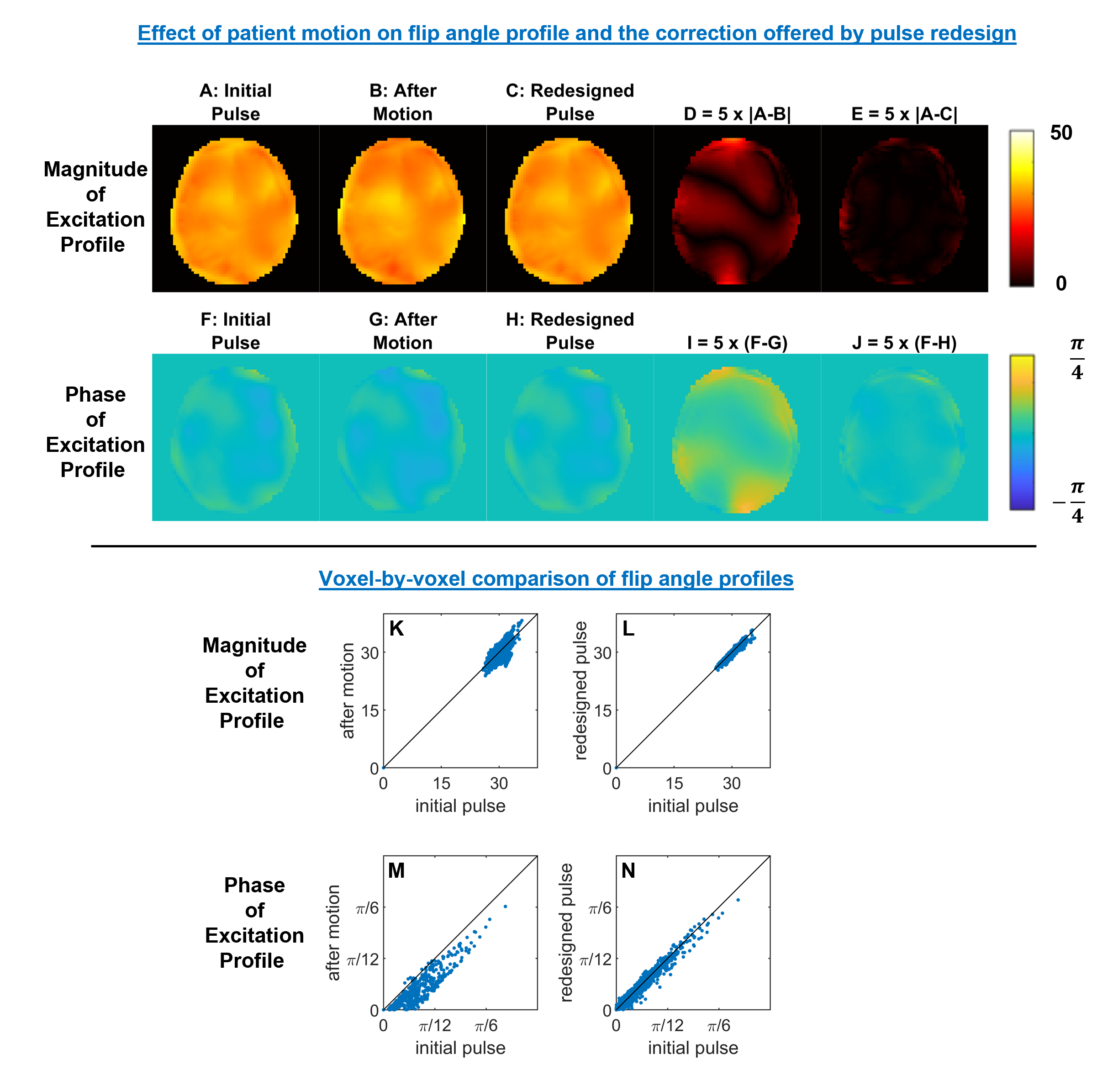
Figure 4: Effect of simulated patient motion and runtime pulse redesign on the excitation profile (A,F). Rightward 10 mm patient motion affects both magnitude and phase (B,G; errors: D,I). Redesigning the pulse in runtime (C,H) reduces both magnitude and phase error (E,J). K-N: Voxel-by-voxel comparison of the excitation profiles. While the phase offset in panel-M could be reduced by gradient readjustments, redesigning the pulse also reduces the spread of both magnitude and phase values around the diagonal (i.e. post-motion profile more closely resembles the pre-motion profile).
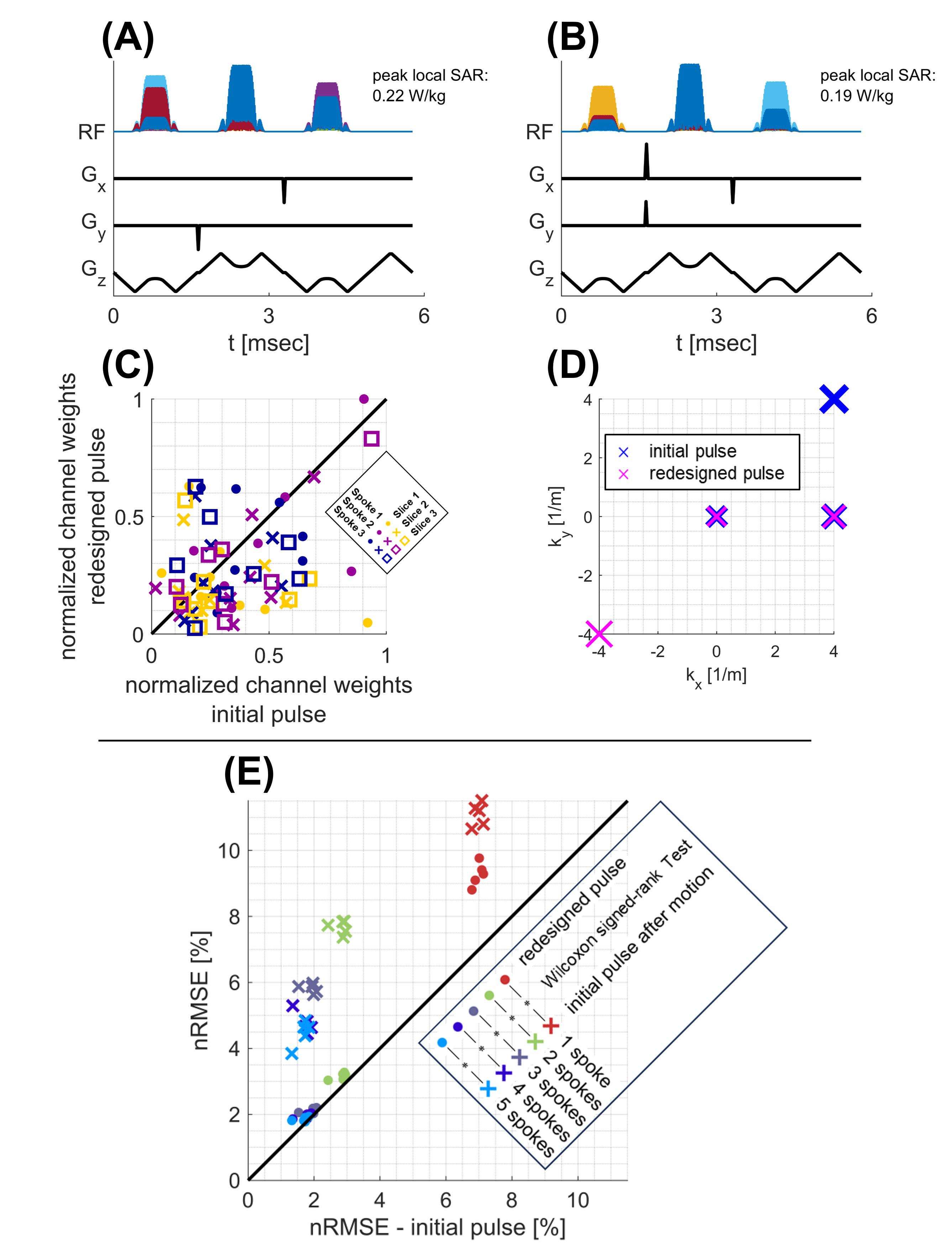
Figure 5: (A-D) Example 3-spoke 3-slice SMS pTx pulses show that the selected spoke locations (D) and the power distribution across channels (C) vary between initial and redesigned pulses (after rightward 10mm motion). (E) nRMSE in magnitude profiles with respect to homogeneous excitation. nRMSE was averaged across slices for SMS. The reduction in nRMSE after redesigning the pulse was statistically significant in all cases (Wilcoxon signed-rank test was applied without averaging across slices for SMS cases).