4090
Dynamic pTx pulse design with accelerated B1+-mapping for cardiac imaging at 7T1Institute of Radiology, University Hospital Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen, Germany, 2Siemens Healthcare GmbH, Erlangen, Germany, 3Electrical Engineering and Information Technology, FH Aachen - University of Applied Sciences, Aachen, Germany, 4Rapid Biomedical GmbH, Rimpar, Germany, 5Physikalisch-Technische Bundesanstalt (PTB), Berlin, Germany, 6Division of Medical Physics in Radiology, German Cancer Research Centre (DKFZ), Heidelberg, Germany, 7Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States
Synopsis
Keywords: Parallel Transmit & Multiband, Parallel Transmit & Multiband
Motivation: Subject-specific pTx methods can counteract excitation inhomogeneities in UHF body imaging, but require lengthy calibration times. Calibrationless universal approaches exist but yield reduced homogeneity for similar SAR levels.
Goal(s): Our aim was to evaluate the possibility of shortening the calibration time by accelerating the B1+-mapping process.
Approach: For 35 heart subjects, tailored pTx pulses were designed on B1+-maps with different undersampling and their performance was compared to universal approaches regarding flip angle homogeneity and SAR.
Results: Tailored pulses designed on accelerated, undersampled B1+-maps (TA=30s) result in improved homogeneity compared to universal pulses or in a roughly 2.5-fold reduction of SAR at comparable homogeneity.
Impact: Subject-specific pTx pulses optimized on accelerated, undersampled B1+-maps allow for improved homogeneity or reduced SAR compared to universal pulses. Reduced SAR could benefit body imaging at 7T, since SAR limitations often prevent the optimal choice of acquisition parameters at UHF.
Introduction
Body imaging at 7T suffers from flip angle (FA) inhomogeneities caused by the shorter, field strength dependent excitation wavelength. Parallel transmission (pTx) methods1 can counteract these inhomogeneities, but subject-specific solutions require long calibration times for mapping the channel-wise transmit (B1+) fields. In this work, we investigate the possibility of accelerating the B1+-mapping via undersampling and compare our approach to calibrationless universal pTx approaches2,3.Methods
For the measurement of 3D channel-wise relative B1+-maps, a method based on the small FA regime4 was used. The sequence was implemented with a density-adapted 3D-radial readout5 (DA-3D-Rad) and measured with following parameters: TE/TR = 2.02/4.5ms, FOV = (320mm)3, nominal resolution = (4mm)3, nominal FA = 8°, projections = 10000, TA = 6min. The projections were measured in the golden angle scheme6 to enable retrospective undersampling. All measurements were carried out at 7T (MAGNETOM Terra, Siemens Healthcare GmbH, Erlangen, Germany) with an 8Tx/16Rx transceiver array (Rapid Biomedical GmbH, Rimpar, Germany). B1+-maps of the heart were acquired for 35 healthy subjects (12 female, 23 male, age = 28.1 ± 8.2 years, BMI = 23.4 ± 3.2 kg/m2). The raw data of the relative B1+-maps were reconstructed with different USFs (1, 2-20, steps of 2) and the sum of magnitudes of the fully sampled maps were used to define a 3D ROI covering the heart. All B1+-maps were normalized by the ROI-mean signal intensity of their sum of magnitudes and multiplied with a scaling factor calculated from an AFI7 measurement of one subject, to obtain absolute B1+-estimations8. Dynamic pTx pulses with a kT-point trajectory9 were optimized, consisting of four rectangular subpulses with a duration of 0.15 ms each, three intervening gradient blips of 0.09 ms3, target FA of 5° and initial specific energy dose (SED, proportional to SAR) limit of 0.1256 J/kg. At first, a universal pulse2 (UP) was designed with the complete library of 35 heart subjects (UP35-4kT). The UP was then used as a starting value to optimize tailored-4kT pulses for each subject and USF. All pulses were evaluated by simulating them on the corresponding fully sampled B1+-maps and calculating the CoVs of the resulting FA distributions. The pulses were also compared to a vendor provided default phase shim, intended for cardiac imaging. Additionally, for USF1 and USF12, tailored-4kT pulses were designed for which the SED limit was gradually lowered until the resulting median CoV equaled that of the UPs. Validation measurements of this approach were performed for one subject with a DA-3D-Rad sequence (TE/TR = 2.02/7 ms, FOV = (320 mm)3, nominal resolution = (1.4 mm)3, nominal FA = 5°, TA = 7 min).Results
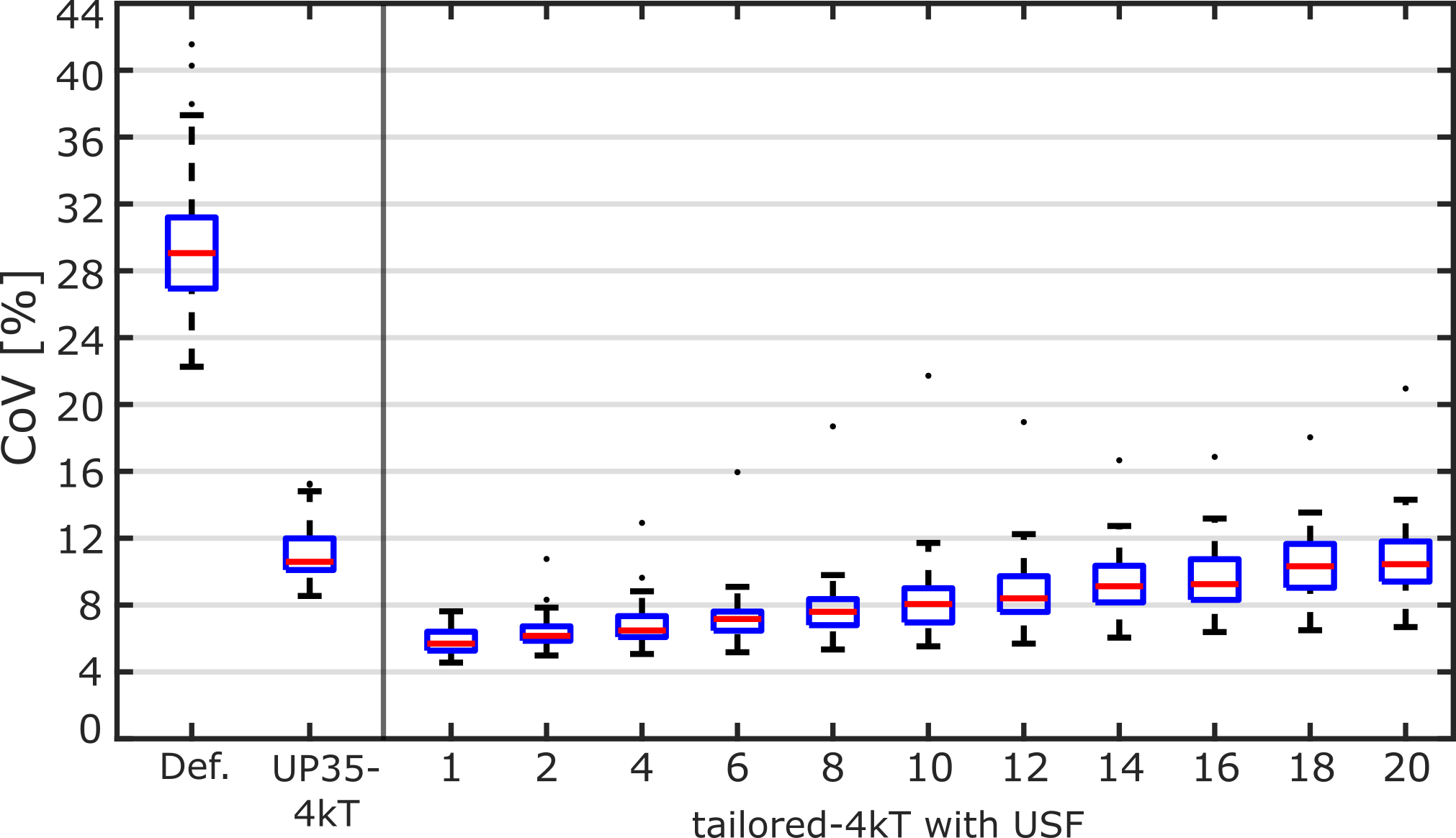
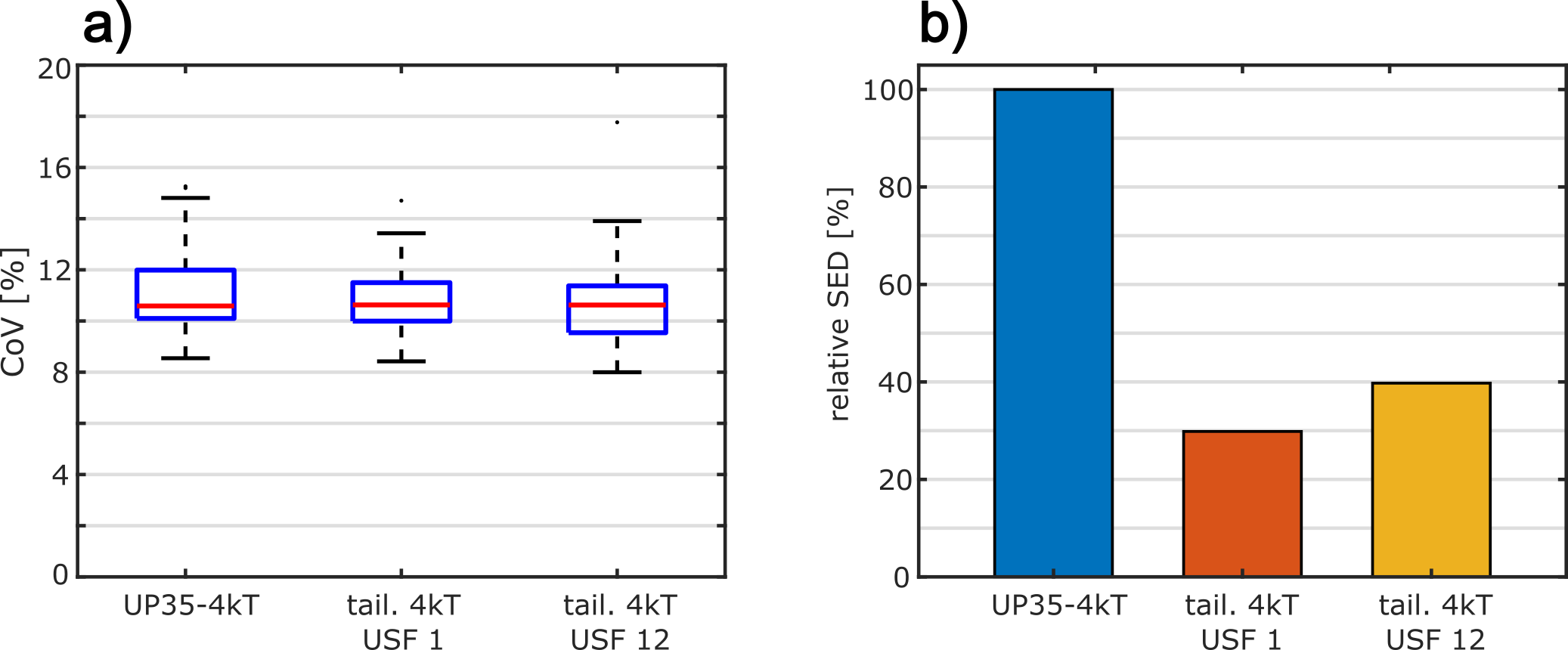
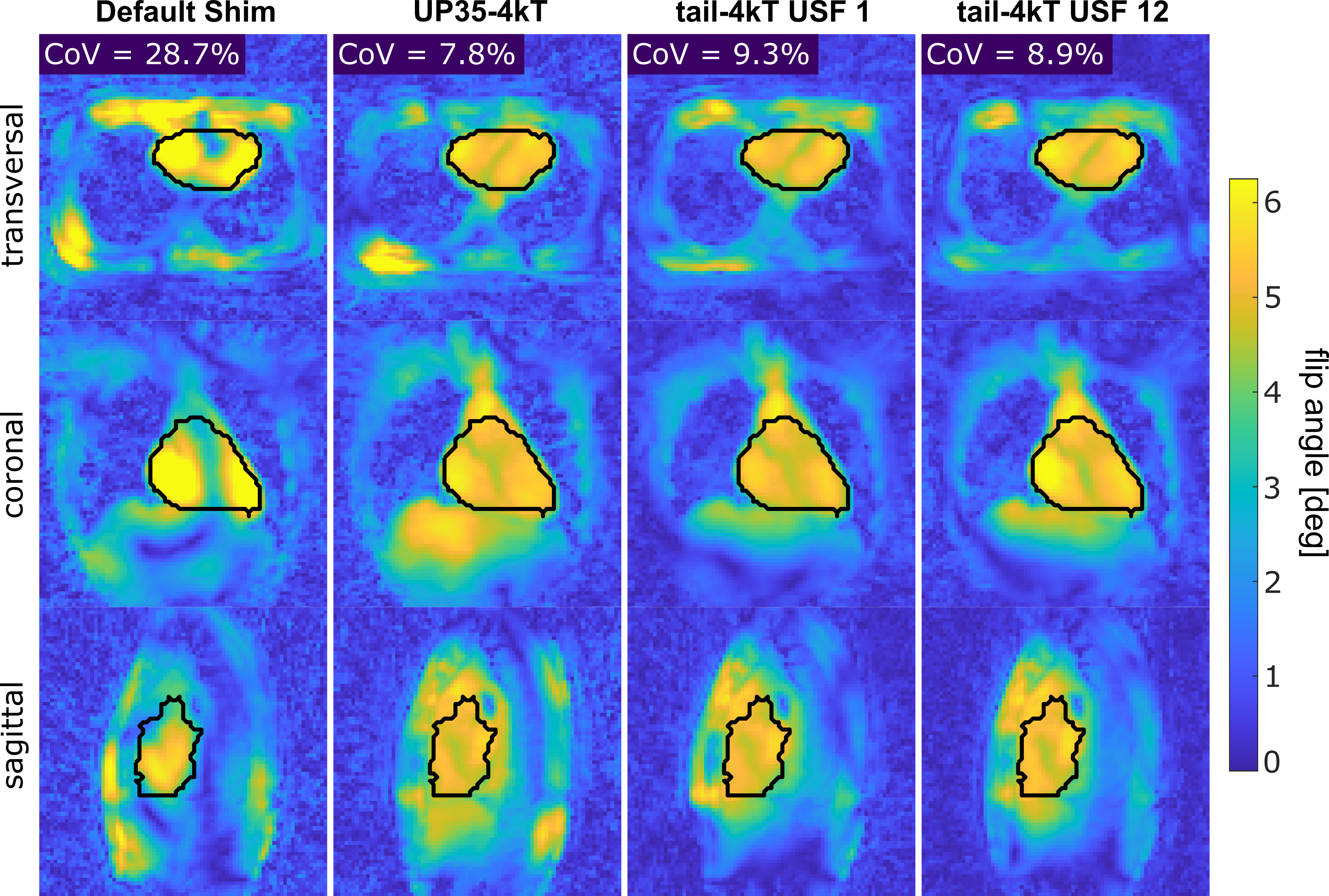
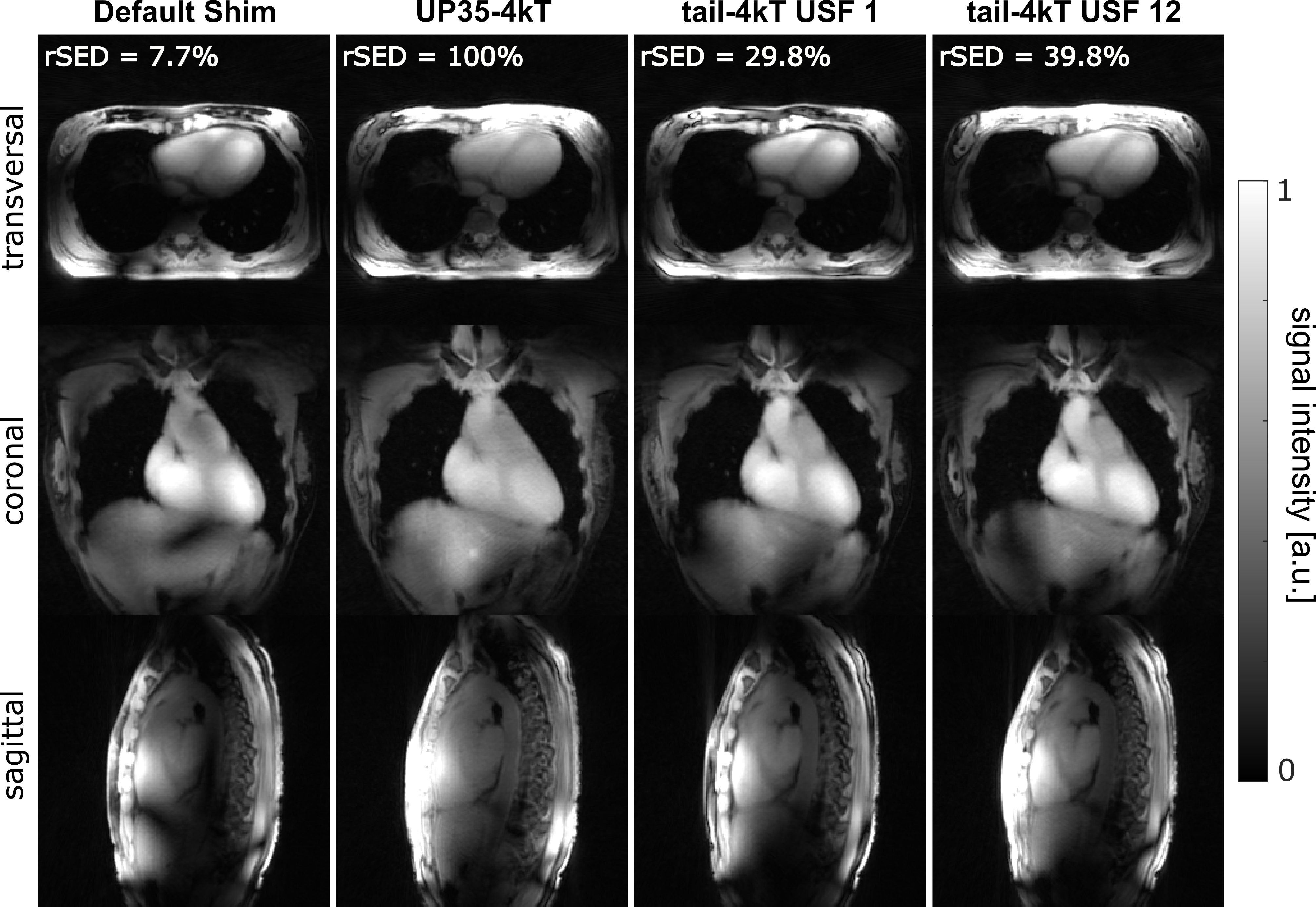
Figure 1 depicts the coefficients of variation (CoVs) of the different pulses for all 35 heart subjects. Compared to the default phase shim, UP35-4kT achieves a reduction of the median CoVs to 10.6% as well as smaller intersubject-variations. Tailored-4kT pulses with USF1 result in a further reduction to a median of 5.7%. The median CoVs and intersubject-variations of the tailored-4kT pulses increase with rising USF. From USF2 onward one strong outlier can be observed. A B1+-mapping time of 30s (≙ USF12) results in a median CoV of 8.4%. Figure 2 shows the SED values of tailored-4kT pulses with USF1 and USF12 optimized to yield an equal median CoV as the UP35-4kT. Relative to the UP, these pulses result in a mean SED of 29.84% ± 0.02% and 39.75% ± 0.04% respectively. A FA simulation of all four pulses is shown in Figure 3 for the subject of the validation measurements and the corresponding DA-3D-Rad images are depicted in Figure 4. In general, simulations and measurements show a good agreement. For the default shim, signal dropouts in the heart are visible, whereas the dynamic pulses result in a homogeneous excitation, although at different SED levels.Discussion and Conclusion
Compared to the vendor provided shim, the homogeneity for cardiac MRI could be substantially improved with the universal 4kT-pulse. Tailored pulses achieved a further improvement, but come at the cost of additional calibration time. As the results illustrate, calibration time could be shortened by accelerating the B1+-mapping via undersampling. Tailored pulses with a B1+-mapping time of 30s still showed improved homogeneity compared to the UP. However, a more important benefit of tailored pulses might be the reduction of SED. Compared to the UP35-4kT, tailored-4kT pulses based on B1+-maps acquired in 30s resulted in a roughly 2.5-fold SED reduction while maintaining comparable homogeneity. The strong outlier visible in Figure 1 may have been caused by patient movement but should be further investigated.Acknowledgements
No acknowledgement found.References
1. Webb AG, Collins CM. Parallel Transmit and Receive Technology in High-Field Magnetic Resonance Neuroimaging. Int J Imag Syst Tech 2010;20:2-13.
2. Gras V, Vignaud A, Amadon A, Le Bihan D, Boulant N. Universal pulses: A new concept for calibration-free parallel transmission. Magn Reson Med 2017;77:635-643.
3. Aigner CS, Dietrich S, Schaeffter T, Schmitter S. Calibration-free pTx of the human heart at 7T via 3D universal pulses. Magn Reson Med 2022;87:70-84.
4. Van de Moortele P-F, Ugurbil K. Very fast multi channel B1 calibration at high field in the small flip angle regime. In Proceedings of the 17th Annual Meeting of ISMRM, Honolulu, HI, 2009. p. 367.
5. Nagel AM, Laun FB, Weber MA, et al. Sodium MRI using a density-adapted 3D radial acquisition technique. Magn Reson Med 2009;62:1565-1573.
6. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging 2006;26:68-76.
7. Yarnykh VL. Actual flip-angle imaging in the pulsed steady state: a method for rapid three-dimensional mapping of the transmitted radiofrequency field. Magn Reson Med 2007;57:192-200.
8. Dietrich S, Aigner CS, Kolbitsch C, et al. 3D Free-breathing multichannel absolute B1+ Mapping in the human body at 7T. Magn Reson Med 2021;85:2552-2567.
9. Cloos M, Boulant N, Luong M, et al. kT‐points: short three‐dimensional tailored RF pulses for flip‐angle homogenization over an extended volume. Magn Reson Med 2012;67:72-80.
Figures