4067
Effects of mild cognitive impairment and disorders of mineral metabolism on structural changes of brain in hemodialysis patients1Department of Medical Imaging, First Affiliated Hospital of Xi’an Jiaotong University, Xi'an, China, 2GE HealthCare MR Research, Beijing, China
Synopsis
Keywords: Dementia, Dementia
Motivation: Brain damage in end-stage renal disease patients with mild cognitive impairment (ESRD-MCI) has not yet been elucidated.
Goal(s): Our goal was to determine the characteristics of alterations in gray matter (GM) structure and the neurobiological mechanisms in ESRD-MCI patients.
Approach: We utilized voxel-based morphology to analyze GM volume alterations in ESRD-MCI patients.
Results: Results demonstrated that MCI in ESRD patients was predominantly impaired in the left middle temporal gyrus, completely mediating the effect of serum phosphorus on MCI.
Impact: Our demonstration of a detectable volume decline in the left middle temporal gyrus utilizing structural MRI provides a quantitative metric to be utilized within clinical therapy trials for intervention of MCI in ESRD patients.
Introduction
With the advancement of dialysis technology, the life cycle of End-stage renal disease (ESRD) patients is prolonged. However, cognitive impairment (CI), including mild cognitive impairment (MCI) and dementia, has merged as critical factor affecting the quality of life for ESRD patients1. While MCI doesn’t significantly affect patients' daily activities, it substantially elevates the risk of progressing to irreversible dementia. The underlying neurobiological mechanism for ESRD patients with MCI (ESRD-MCI) remains unclear. This study aimed to explore alterations in brain structure and identify clinical risk factors in ESRD- MCI patients.Methods
This study protocol was registered at ClinicalTrials. gov (NCT03961724, https://clinicaltrials.gov/ct2/show/NCT03961724) and received local ethics committee approval (XJTU1AF-CRF-2018-006). Patients with ESRD who received regular hemodialysis were recruited from the Department of Nephrology at the local hospital. Health controls (HCs) were recruited by posting advertisements in the local community. All MR examinations were performed on a 3.0T MR scanner (Discovery MR750: GE Healthcare, Chicago, IL, USA) equipped with a 24-channel head-neck unite coil. Structural image data for each participant were obtained using a three-dimensional brain volume imaging sequence (3D-BRAVO) with the following parameters: echo time = 3.2 ms; repetition time = 8.2 ms; flip angle = 15°; slice thickness = 1 mm; matrix = 256 × 256; slices number = 140. All participants completed Montreal Cognitive Assessment (MoCA) assessment and were divided into three groups (MoCA scores ≥26, ESRD with non-CI (ESRD-NCI) group and HCs group; MoCA scores 18-26, ESRD-MCI group). Clinical blood indicators were collected for ESRD patients. T1 image data were processed using the Computational Anatomy Toolbox 12 software (CAT12, http://www.neuro.uni-jena.de/cat/) in MATLAB 2021a (MathWorks Inc., Natick, USA). General clinical data were analyzed using SPSS software (version 26.0; IBM Corp, Armonk, NY, USA). And grey matter (GM) volume differences among the three groups were analyzed using voxel-based morphometry (VBM) with CAT12. In addition, correlation analysis using SPSS software was performed to determine the association among GM volume changes, clinical risk factors, and MCI.Results
A total of 65 ESRD patients (34 ESRD-MCI and 31 ESRD-NCI) and 55 HCs were included (Figure 1). Compared with HCs, both ESRD-MCI and ESRD-NCI patients showed decline in multiple cognitive domains function (Table 1) and reduction in diffuse GM volume (p < 0.05 FWE-corrected) (Figure 2A-B). In addition, when compared with ESRD-NCI patients, ESRD-MCI patients showed decreased GM volume in the left middle temporal gyrus (MTG) (p < 0.05 FWE-corrected) (Figure 2C). In the ESRD-MCI group, significant correlations were found among GM volume, MoCA scores, and serum phosphorus levels. A further mediation analysis showed decreased GM volume in the left MTG completely mediates the effect of serum phosphorus levels on MCI (Figure 3).Discussion
MCI in ESRD encompasses impairment in multiple cognitive domains, including executive function, attention, memory, language, etc. MCI exhibits high heterogeneity with various underlying etiologies, such as Alzheimer’s disease and vascular cognitive impairment2. These distinct etiologies of MCI have different mechanisms and treatment strategies. Therefore, early identification of MCI in ESRD patients can provide a theoretical basis for precise clinical treatment such as TMS intervention targets. Neuroimaging techniques, particularly MRI, provide a simple, objective, and reproducible detection method for the identification of MCI. In comparison to HCs, a previous study has found extensive structural brain abnormalities in ESRD patients with MCI3. But few studies have compared brain structural differences between ESRD-MCI and ESRD-NCI patients. Our study found that ESRD-MCI patients showed decreased GM volume of the left MTG compared to ESRD-NCI. The left MTG is primarily responsible for storing semantic knowledge, a crucial component of our daily behaviors and communication4,5. Furthermore, our mediation analysis indicated that the decreased GM volume of the left MTG fully mediated the impact of serum phosphorus levels on MCI. Maintaining appropriate serum phosphorus levels is vital for cellular function. Elevated serum phosphate levels in dialysis patients can result from variation in varying dialytic removal, phosphate absorption, and phosphate binder efficacy6. Previous studies have shown that hyperphosphatemia is associated with CI, although the mechanism remains unclear. It may be related to elevated phosphate leading to medial calcification and endothelial dysfunction, which induces vascular injury, and then causes CI7. However, hypophosphatemia can also adversely affect the brain. Therefore, determining the appropriate range for serum phosphorus control in the clinical practice is essential for the prevention of MCI in ESRD patients.Conclusion
We found that the left MTG is a critical brain region for MCI and increased serum phosphate maybe a risk factor for MCI in ESRD patients. This result provides a theoretical basis for clinical intervention for MCI in ESRD patients.Acknowledgements
The authors wish to thank all the participants in this study. We owe our gratitude to the clinical and nursing teams of the first Affiliated Hospital of Xi'an Jiaotong University.References
1. Kurella Tamura M. and Yaffe K. Dementia and cognitive impairment in ESRD: diagnostic and therapeutic strategies. Kidney Int. 2011;79(1):14-22.2. Viggiano D, Wagner CA, Blankestijn PJ, et al. Mild cognitive impairment and kidney disease: clinical aspects. Nephrol Dial Transplant. 2020;35(1):10-17.
3. Zheng J, Jiao Z, Dai J, et al. Abnormal cerebral micro-structures in end-stage renal disease patients related to mild cognitive impairment. Eur J Radiol. 2022;157:110597.
4. Whitney C, Jefferies E, Kircher T. Heterogeneity of the left temporal lobe in semantic representation and control: priming multiple versus single meanings of ambiguous words. Cereb Cortex. 2011;21(4):831-844.
5. Tune S, Asaridou SS. Stimulating the Semantic Network: What Can TMS Tell Us about the Roles of the Posterior Middle Temporal Gyrus and Angular Gyrus? J Neurosci. 2016;36(16):4405-4407.
6. Sherman RA. Hyperphosphatemia in Dialysis Patients: Beyond Nonadherence to Diet and Binders. Am J Kidney Dis. 2016;67(2):182-186.
7. Rroji M, Figurek A, Viggiano D, et al. Phosphate in the Context of Cognitive Impairment and Other Neurological Disorders Occurrence in Chronic Kidney Disease. Int J Mol Sci. 2022;23(13):7362.
Figures
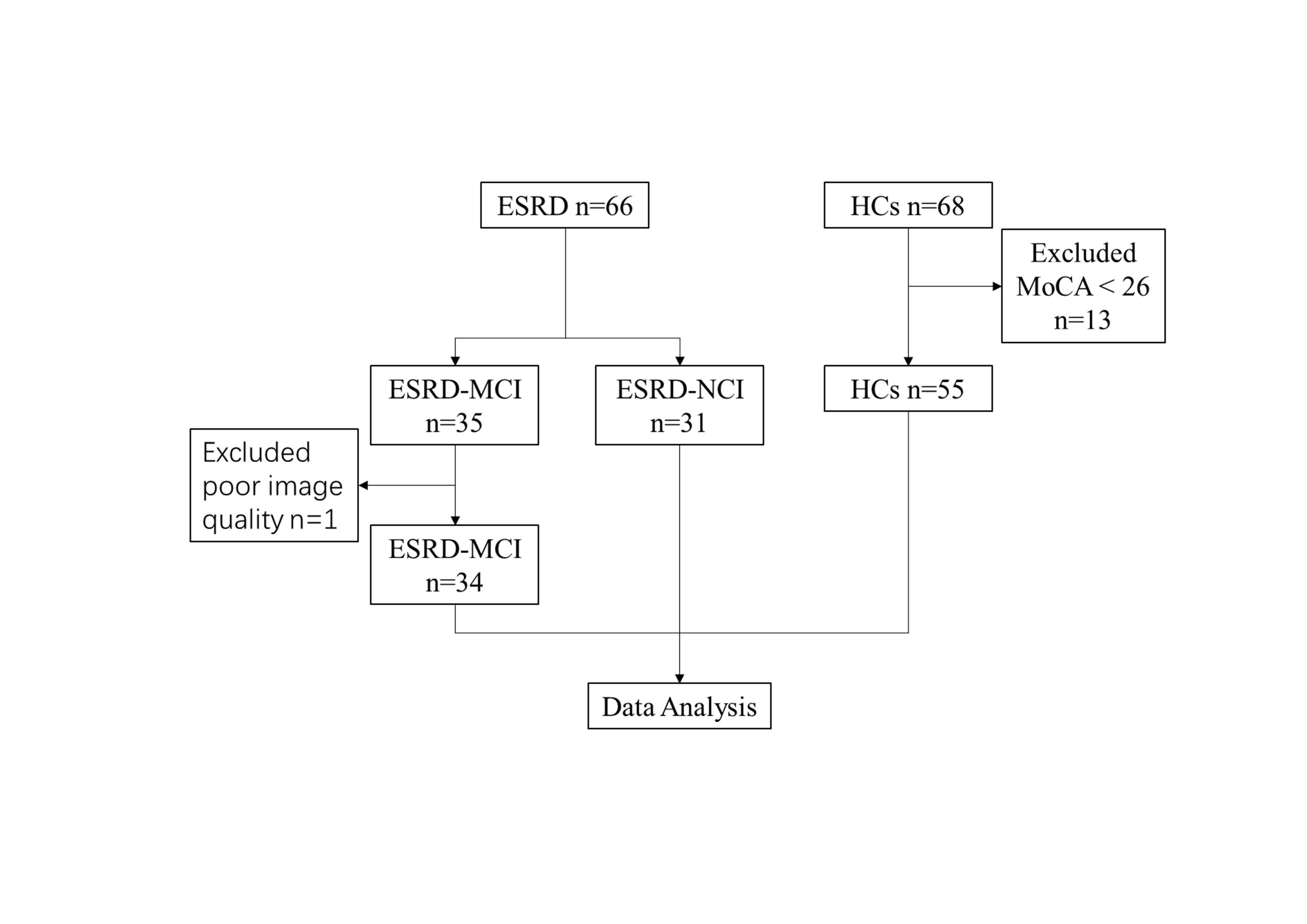
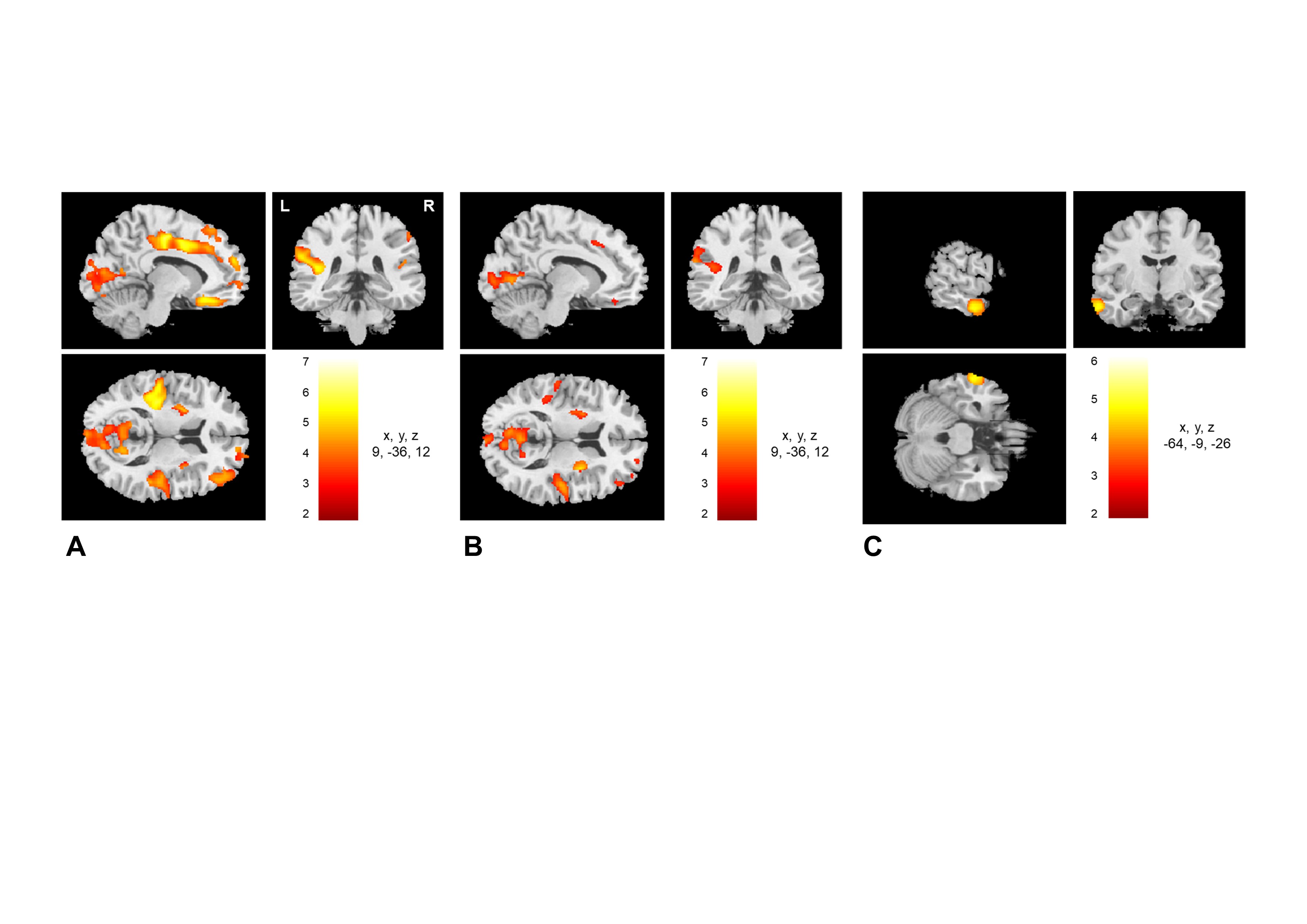
FIGURE 2. Spatial maps of GM volume changes in the ESRD-MCI, ESRD-NCI, and HCs group. ESRD-MCI and ESRD-NCI patients showed diffuse damage of brain areas on images compared to HCs (p < 0.05 family-wise error-corrected). Compared to ESRD-NCI patients, ESRD-MCI patients showed decreased GM volume in the left middle temporal gyrus (p < 0.05 family-wise error-corrected). GM: grey matter; ESRD: end-stage renal disease; MCI: mild cognitive impairment; NCI: non-cognitive impairment; HCs: healthy controls.
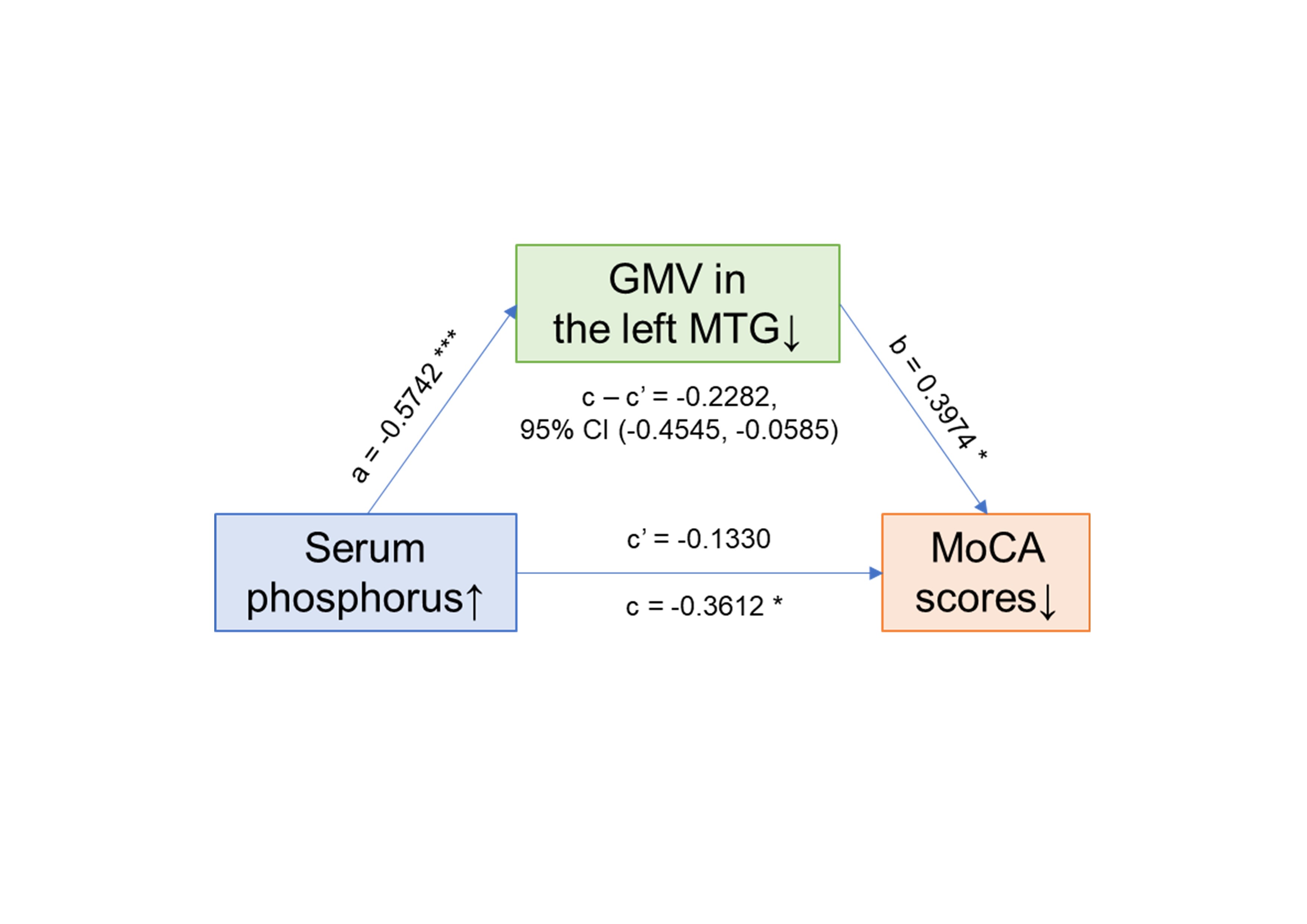
FIGURE 3. Mediation analysis. The independent factor was serum phosphorus level and the dependent variable was Montreal Cognitive Assessment (MoCA) scores, with the GMV (grey matter volume) coefficient in the left middle temporal gyrus (MTG) as the proposed mediator. The mediation analysis indicated that decreased grey matter volume in the left MTG completely mediates the effect of serum phosphorus levels on global cognitive impairment in end-stage renal disease patients with mild cognitive impairment. * p < 0.05, ** p < 0.01, *** p < 0.001.
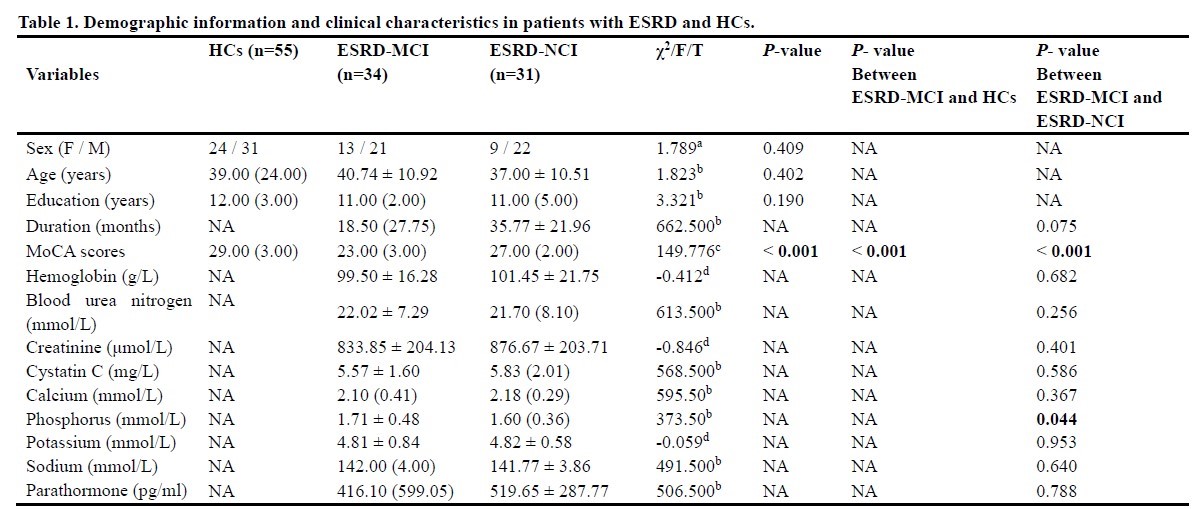
TABLE 1. Sex is reported as frequencies. Mean ± standard deviation is reported. Medians and interquartile ranges are reported.
ESRD: end-stage renal disease; HCs: health controls; MCI: mild cognitive impairment; NCI: non-cognitive impairment; F: female; M: male; MoCA: Montreal cognitive assessment.
aAnalyzed using chi-square test; bAnalyzed using Mann-Whitney U test; cAnalyzed using one-way analysis of covariance (ANCOVA) adjusted for sex, age, and education level; dAnalyzed using independent two-sample t-test.