4057
Topological disruption of freezing of gait in multiple system atrophy1China medical university, Shenyang, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Other Neurodegeneration, Degenerative, Multiple system atrophy
Motivation: Functional brain network studies of freezing of gait have been extensive in PD in recent years, but are still lacking in MSA, where the disease deteriorate more rapidly.
Goal(s): Investigate the disrupted topology of functional interactions in MSA-FOG. Extend our knowledge of the neurobiological basis of FOG in MSA.
Approach: We constructed and analysed functional network at global, node and modular levels when compared among MSA patients with and without freezing of gait and matched healthy controls.
Results: The aberrations of visual network, DAN and coupling changes between visual network and cerebellum were found in MSA-FOG compared to MSA-nFOG and HC.
Impact: Different from focusing on pairwise brain regions, our study proved MSA-FOG FC alterations in the visual network and the dorsal attention network as well as coupling pattern changes between visual network the other networks at the large-scale network level.
Introduction
Freezing of gait (FOG) has been recognized as a primary symptom of Parkinson's disease (PD)[1, 2]. However, it is more common in the atypical Parkinson's disease, such as multiple system atrophy (MSA)[3]. The consequences of FOG extend far beyond its motor symptoms, frequently leading to falls and related injuries, and seriously worsen the survival of patients[4]. Therefore, it is necessary to reveal the neuropathological mechanisms related to FOG, allowing for early management and intervention. Recent researches have unveiled the existence of the disconnection syndrome, indicating that FOG is not only a motor symptom, but rather a composite result of the interaction of movement, cognition and emotion[5]. Thalamus-based FC abnormalities in regions related to cognition and emotion[6] was found in MSA-FOG in Cheng’s study. However, this seed-based analyse can not fully capture and reflect the changes in functional connectivity from the perspective of the whole-brain networks. Adopted a novel approach by focusing on the perspective of brain network, this study aims to investigate the differences in rest functional network at global, node and modular levels when compared among MSA patients with and without freezing of gait and matched healthy controls (HC).Method
40 patients with MSA diagnosed with probable or possible MSA and 20 age-and gender matched healthy controls (HC) were enrolled. All participants underwent MRI examinations on a 3T system (MAGNETOM Trio a Tim System (Siemens Healthcare, Erlangen, Germany) including: 3D magnetization-prepared rapid gradient echo (MPRAGE) T1WI and functional imaging by echo-planar imaging (EPI) and a comprehensive assessment including Unified Multiple System Atrophy Rating Scale (UMSARS) , and the Hoehn and Yahr (H-Y) stage for measuring disease severity, and Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment(MoCA) for global cognitive function. 20 MSA-FOG patients were defined by the FOG episodes observed by neurologists observed, patients or their caregivers. The functional data were preprocessed using the Gretna toolbox(2.0) based on Statistical Parametric Mapping (SPM, version12, http://www.fil.ion.ucl.ac.uk/spm) in MATLAB software (version 2018a, MathWorks). The nodes for network construction were defined by brain regions that were segmented by the brainnetome atlas. The topological metrics of the constructed networks were analyzed.Results
For global topologic metrics, MSA-FOG showed decreased whole brain network global efficiency compared to the MSA-nFOG and decreased efficiency in default network (DMN) and dosal attention network (DAN).Regarding nodal metrics, MSA-FOG exhibited an increased degree centrality (DC) and nodal efficiency (NE) in superior parietal lobule (SPL) caudal area compared to MSA-nFOG and HC. MSA-FOG exhibited widely weak DC and NE in globus pallidus, nucleus accumbens, dorsolateral putamen, pre-motor thalamus (nodes of basal ganglia) and strong DC and NE in precuneus medial area (node of somatomotor network, SMN ), parietooccipital sulcus, occipital gyrus(nodes of visual network) and Precuneus area 31(node of DMN).
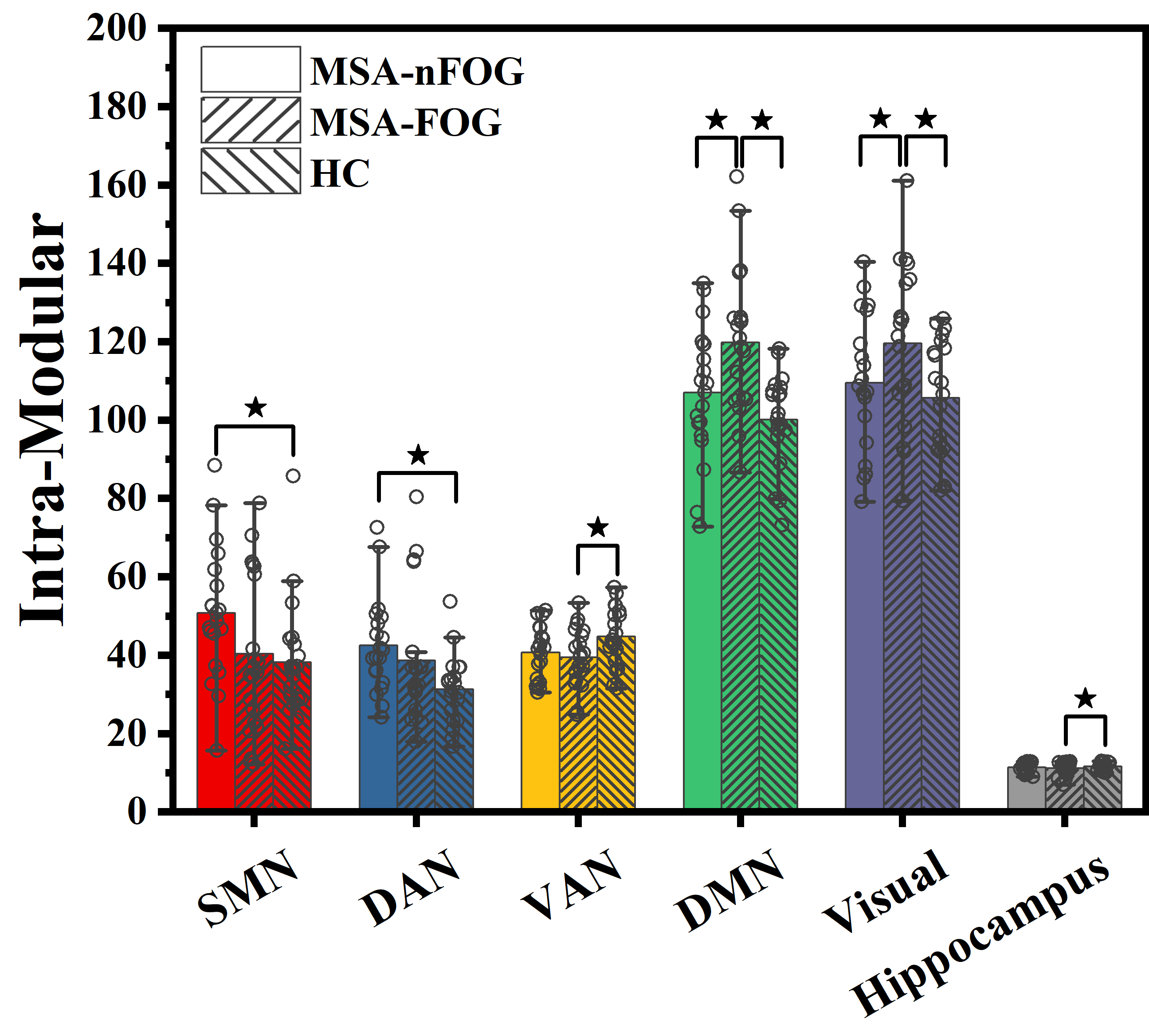
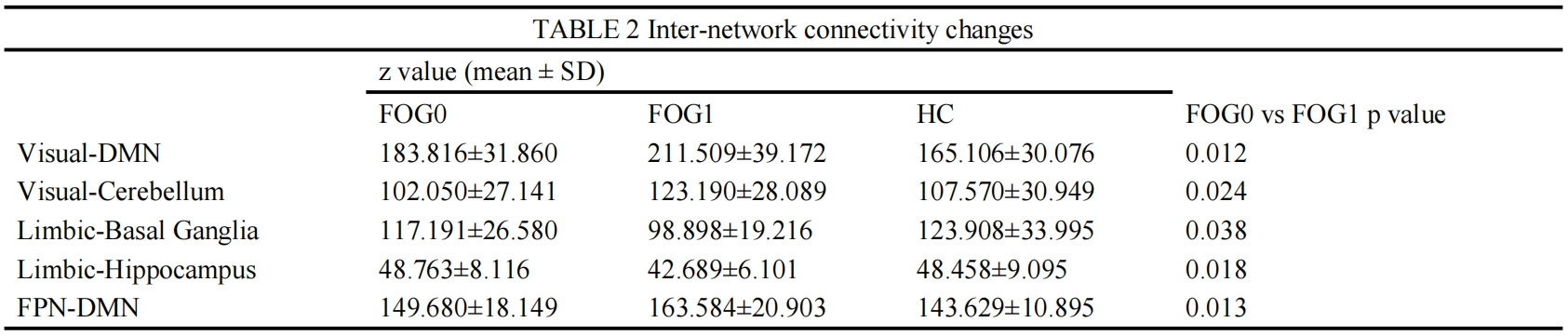
In modular analysis, MSA-FOG displayed reduced inter-modular functional connectivity (FC) between visual network and DMN, and between limbic area and basal ganglia and hippocampus compared to MSA-nFOG group. Additionally, they exhibited significantly greater FC between visual network and cerebellum, and between frontoparietal network (FPN) and DMN. Furthermore, MSA-FOG showed higher intramodular FC in visual, basal ganglia network and DMN compared with MSA-nFOG and HC.
Discussion
For the rapid deterioration of MSA and the difficulty of accurate identification, there are few studies on topological disruption of FOG in MSA. In our study, graph theory indicators of DAN, DMN,Visual network showed consistently elevation while a few basal ganglia nodes showed consistently reduction compared with MSA-nFOG. MSA-FOG showed increased intra-network FC of visual network and DMN. DAN mediated the top-down guided voluntary allocation of attention. The increased FC of visual network and aberration of coupling changes between DMN and cerebellum might play a compensatory role in overcoming the basal ganglia failure during walking[7]. The aberration of visusal network and DAN and coupling changes between networks was closely related with FOG in MSA.Conclusion
To sum up, our research illustrated topological disruption in MSA, with a specific focus on FOG, from a network perspective. There are extensive alterations in topological properties and disrupted topology of functional interactions in MSA-FOG. Our results extend our knowledge of pathological mechanisms with an eye towords sensitive diagnose and progression biomarkers for MSA.Acknowledgements
No acknowledgement found.References
[1] NUTT J G, BLOEM B R, GILADI N, et al. Freezing of gait: moving forward on a mysterious clinical phenomenon [J]. Lancet Neurol, 2011, 10(8): 734-744. [2] MANCINI M, BLOEM B R, HORAK F B, et al. Clinical and methodological challenges for assessing freezing of gait: Future perspectives [J]. Mov Disord, 2019, 34(6): 783-790. [3] POEWE W, STANKOVIC I, HALLIDAY G, et al. Multiple system atrophy [J]. Nat Rev Dis Primers, 2022, 8(1): 56. [4] GAO C, LIU J, TAN Y, et al. Freezing of gait in Parkinson's disease: pathophysiology, risk factors and treatments [J]. Transl Neurodegener, 2020, 9: 12. [5] WEISS D, SCHOELLMANN A, FOX M D, et al. Freezing of gait: understanding the complexity of an enigmatic phenomenon [J]. Brain, 2020, 143(1): 14-30. [6] CHENG Y, YANG H, LIU W V, et al. Alterations of brain activity in multiple system atrophy patients with freezing of gait: A resting-state fMRI study [J]. Front Neurosci, 2022, 16: 954332. [7] HUANG H-C, CHEN C-M, LU M-K, et al. Gait-Related Brain Activation During Motor Imagery of Complex and Simple Ambulation in Parkinson's Disease With Freezing of Gait [J]. Frontiers in Aging Neuroscience, 2021, 13.Figures
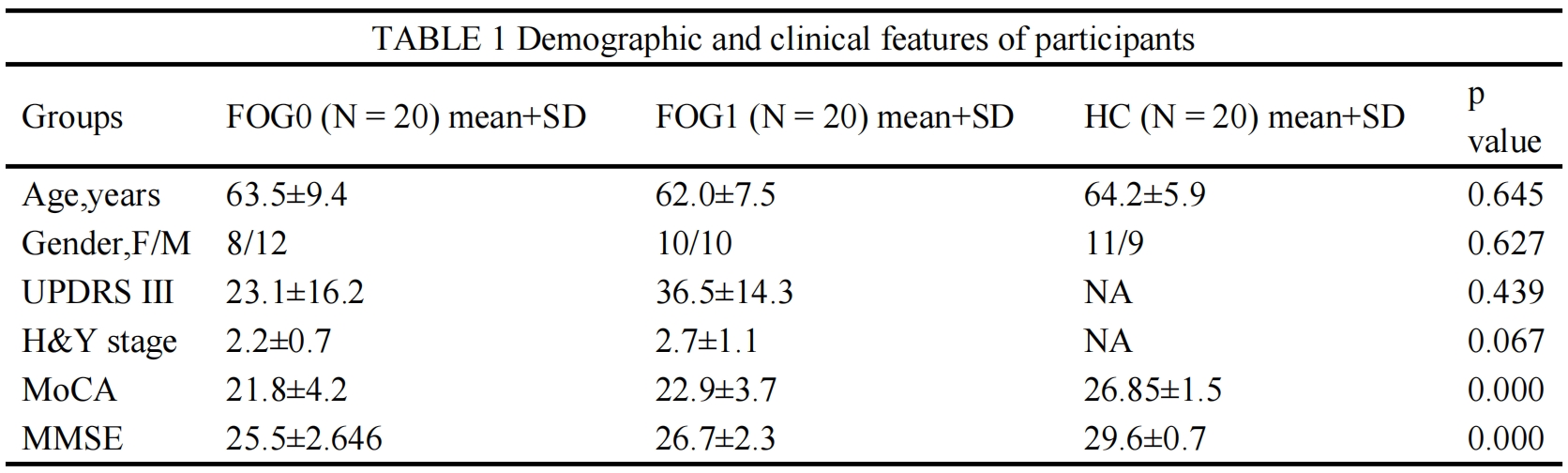
Note: Data was represented as mean ± SD; N/A indicates not applicable. Abbreviations: F, female; HC, healthy control; H-Y, Hoehn-Yahr; M, male; MMSE, Mini-mental State Examination; MoCA, Montreal Cognitive Assessment; UPDRS, Unified Parkinson's Disease Rating Scale.
A corrected threshold of p < 0.05 corrected by LSD.
z value represent the connection strength between two networks.