4045
One year aerobic exercise improved fitness, cognition, reduced arterial stiffness and brain vascular reactivity to CO2 in amnestic MCI1Department of Biomedical Engineering, University of Texas at Dallas, Dallas, TX, United States, 2Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States, 3Institute for Exercise and Environmental Medicine, Texas Health Presbyterian Hospital, Dallas, TX, United States, 4National Institute of Advanced Industrial Science and Technology, Tsukuba, Japan, 5The Hospital for Sick Children, Toronto, ON, Canada, 6Department of Neurology and Neurotherapeutics, University of Texas Southwestern Medical Center, Dallas, TX, United States, 7Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, TX, United States, 8Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX, United States, 9Department of Radiology and Radiological Science, John Hopkins University School of Medicine, Baltimore, MD, United States, 10Department of Bioengineering, University of Texas at Arlington, Arlington, TX, United States
Synopsis
Keywords: Alzheimer's Disease, Alzheimer's Disease, Cerebrovascular Reactivity, Aerobic Exercise, Cardiorespiratory Fitness, Carotid Artery Stiffness
Motivation: The benefits of long-term aerobic exercise (AE) on brain function in amnestic mild cognitive
impairment (aMCI) patients is not fully understood.
Goal(s): This study assesses long-term benefits of AE on cerebrovascular reactivity (CVR) in aMCI in
relation to cognition, cardiorespiratory fitness and carotid arterial stiffness.
Approach: 27 aMCI patients were assigned randomly to either AE or stretching and toning (ST) groups.
CVR MRI, cardiorespiratory fitness, cognition, carotid arterial stiffness using ultrasound were
measured before and one-year after AE or ST intervention.
Results: One-year intervention improved fitness and cognition, decreased arterial stiffness and CVR in
the AE group, not different in the ST group.
Impact: Long-term aerobic exercise (AE) intervention in amnestic MCI patients improved cardiorespiratory fitness and cognition, reduced arterial stiffness and cerebrovascular reactivity(CVR), suggesting that long-term AE improves cognition and vasculature; CVR reduction is suggestive of vascular adaptations to long-term AE.
Background
Amnestic mild cognitive impairment (aMCI) is a precursor stage to Alzheimer’s disease (AD). Modest results of clinical trials to prevent decline from aMCI to AD have led investigators to search for alternatives. Aerobic exercise (AE) is a low-cost, potentially effective approach to stall or prevent AD. We previously reported that one-year AE intervention in aMCI patients led to increased cerebral blood flow (CBF) that correlated with improved memory1. The purpose here is to assess if one-year AE improves cerebrovascular reactivity (CVR), i.e. vascular dilation capacity.Methods
Seventy patients with aMCI were randomly assigned to either the AE or the stretching and toning (ST) study arm. 34 patients withdrew from the study for medical reasons. Neuropsychological, cardiorespiratory, MRI and ultrasound measures were collected before and after a 12-month AE or ST intervention in 27 participants, 11 in the AE and 16 in the ST group. AE regimen: Each participant in the AE group was instructed to perform moderate-to-vigorous AE at 75-85% of their maximal heart rate, assessed by the maximal oxygen uptake (VO2max) test. AE training began with 3 exercise sessions per week for 25–30 minutes per session. AE frequency and duration were gradually increased over time. Any mode (jogging, cycling, etc.) of AE was allowed as long as the prescribed dose and intensity was maintained. ST regimen: ST was used as active control. The ST group performed stretch and toning routines focused on the upper and lower body, and were trained to maintain their heart rate below 50% of maximal heart rate. Training frequency and duration were the same across groups. MRI experiment: MRI experiments were performed on a 3T MRI scanner with an 8-ch head coil (Philips, Netherlands). The MRI protocol consisted of whole-brain T1-weighted MPRAGE and a CVR BOLD scan. MPRAGE images were acquired at 1×1×1mm3 resolution. CVR was measured using hypercapnia (inhalation of 5% CO2 mixed with 21% O2 and 74% N2). Room air (1 min) and hypercapnia (1 min) were inhaled by the patient alternatively while BOLD images were acquired continuously for 7 minutes at 3.0x3.0x5 mm3 resolution with typical imaging parameters. Linear regression between the end-tidal CO2 time-course and BOLD images was used to generate a CVR map. Relative CVR maps were calculated by normalizing each voxel's CVR value with the mean value from the cerebellum, to normalize differences due to intervention and allow comparison between groups. Cognition: Effect of AE in older adults was largest on executive function (EF) compared to other cognitive domains2. So, we mainly focused on EF. EF was assessed using the Delis-Kaplan-Executive-Function-System (DKEFS). We also assessed neuropsychiatric symptoms using the Neuropsychiatric Inventory questionnaire (NPI-Q) and measured activities of daily living using the Functional assessment questionnaire (FAQ). Carotid artery stiffness: Carotid artery stiffness was measured using ultrasound.Results and Discussions
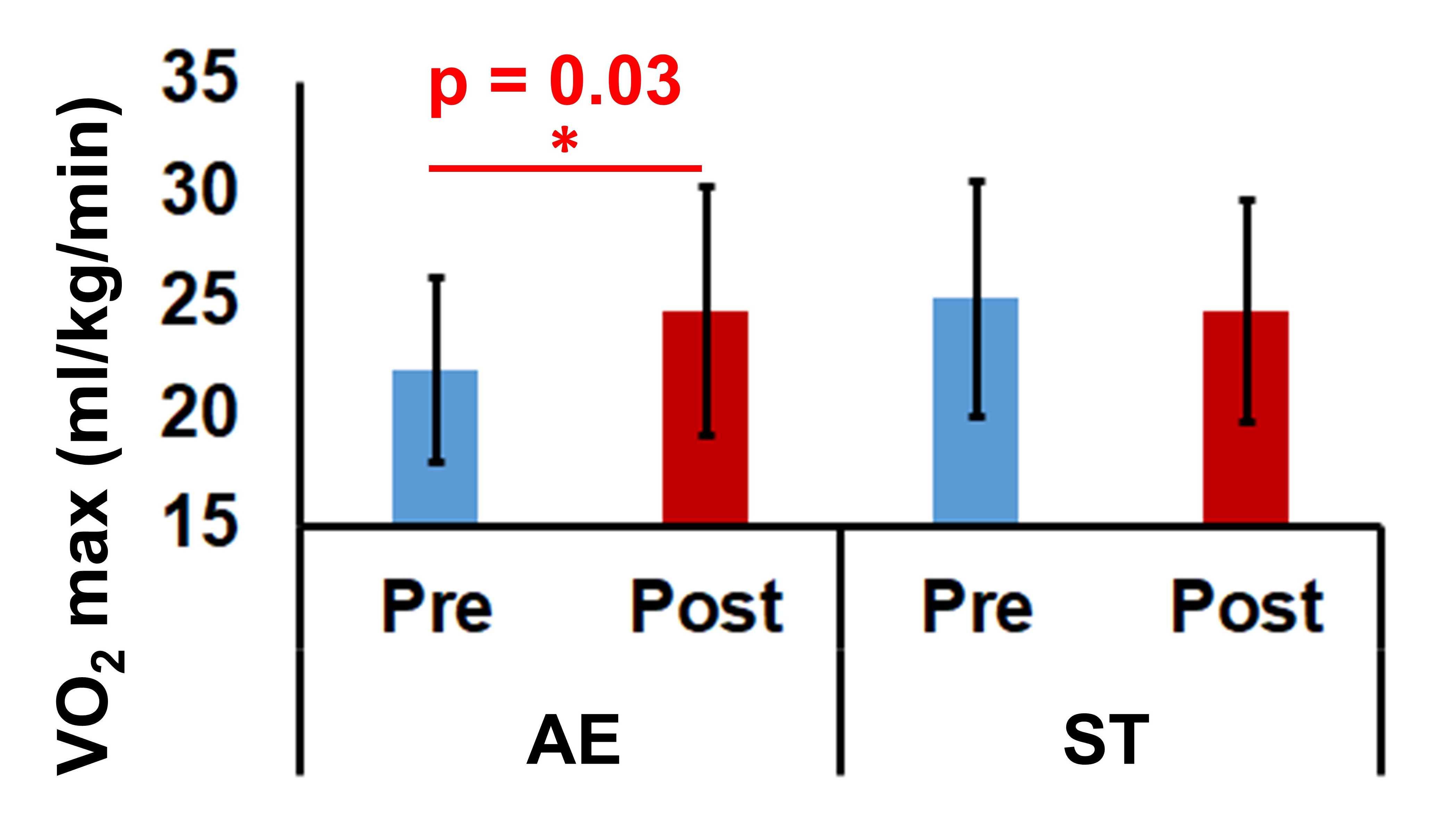
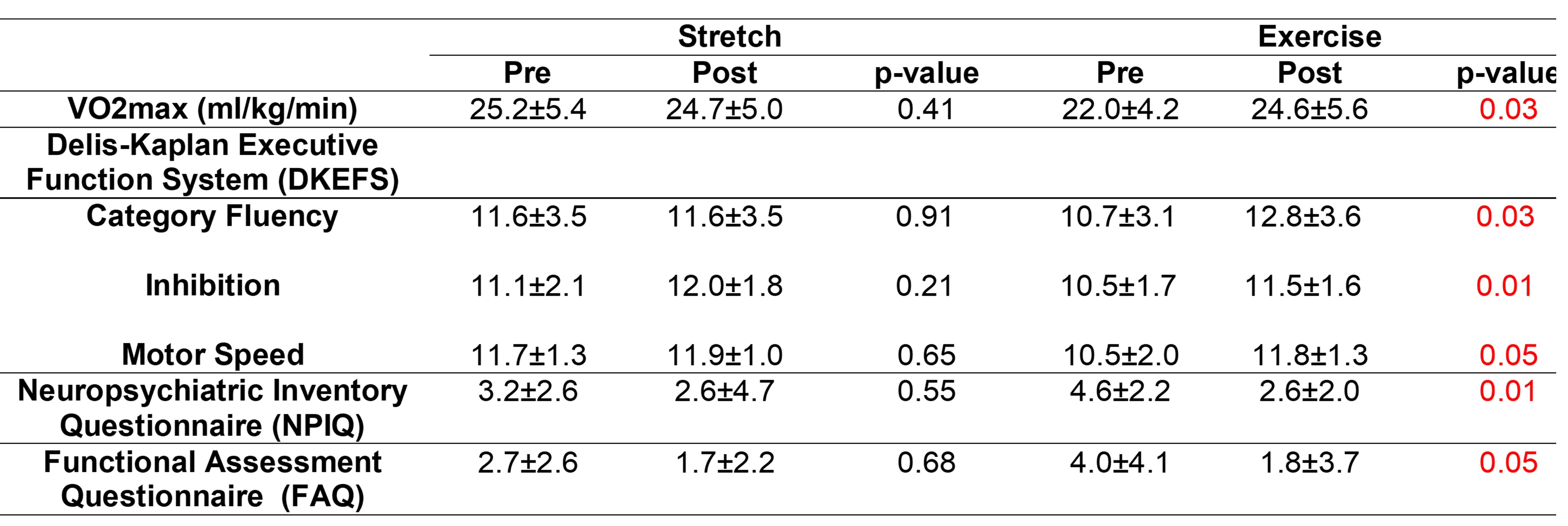
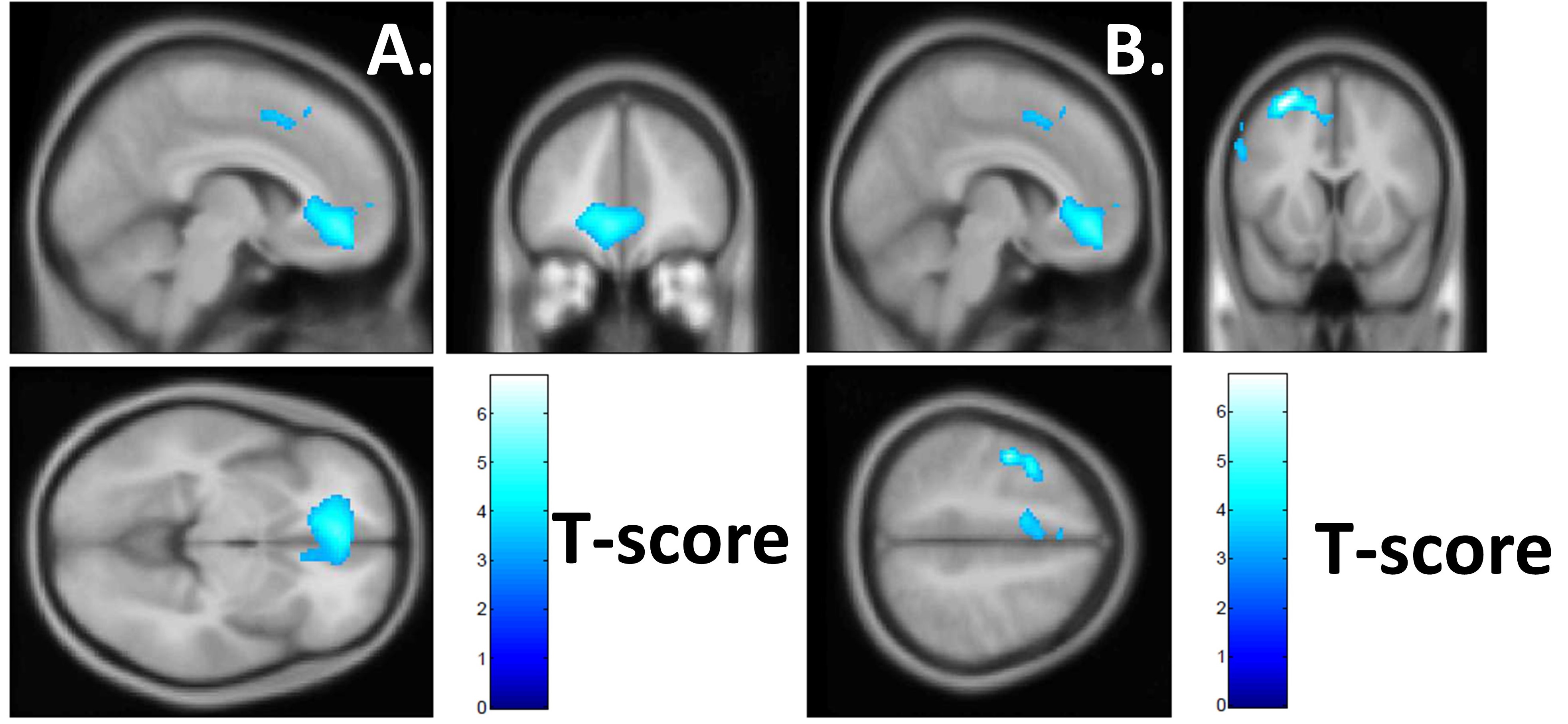
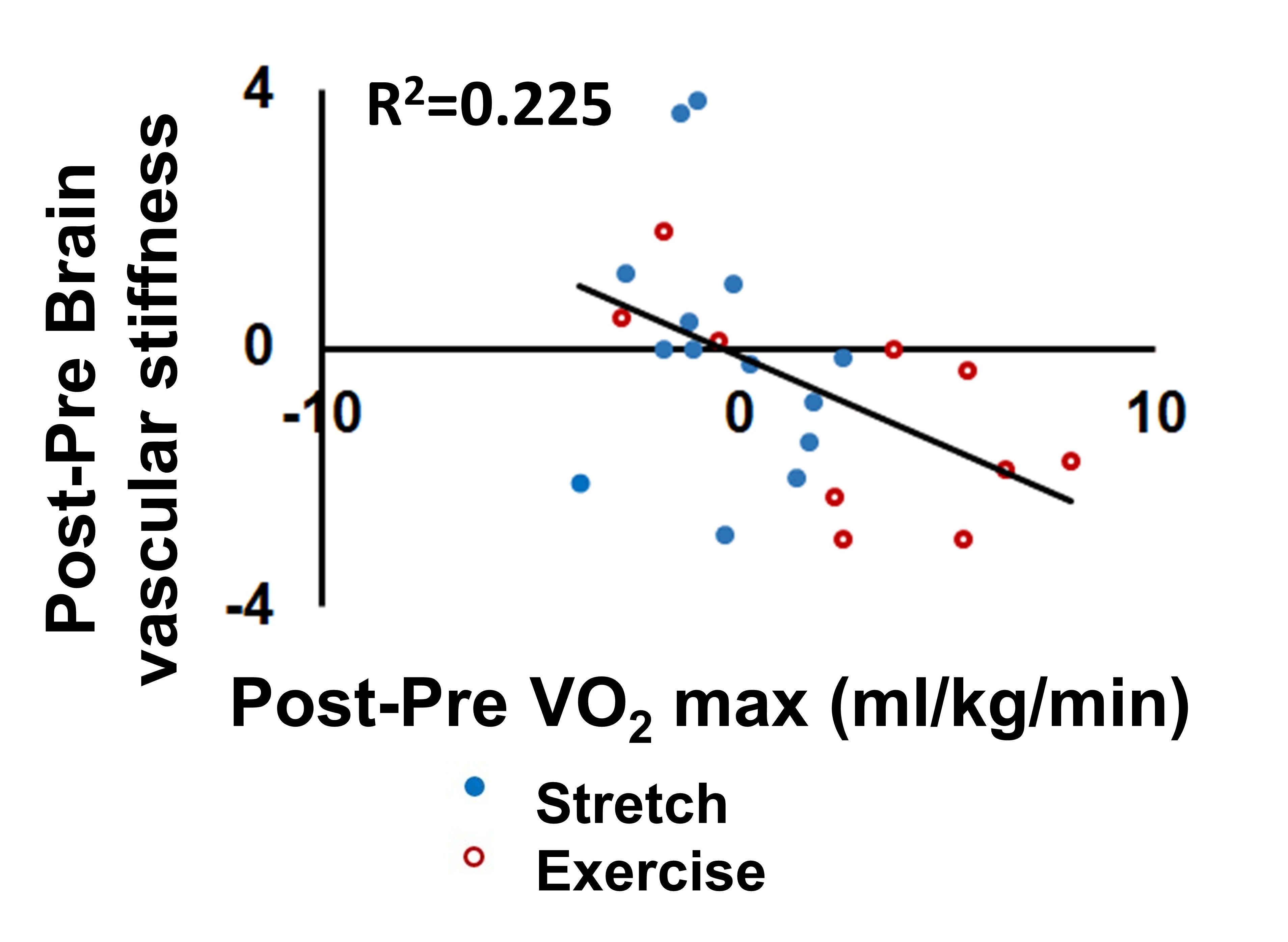
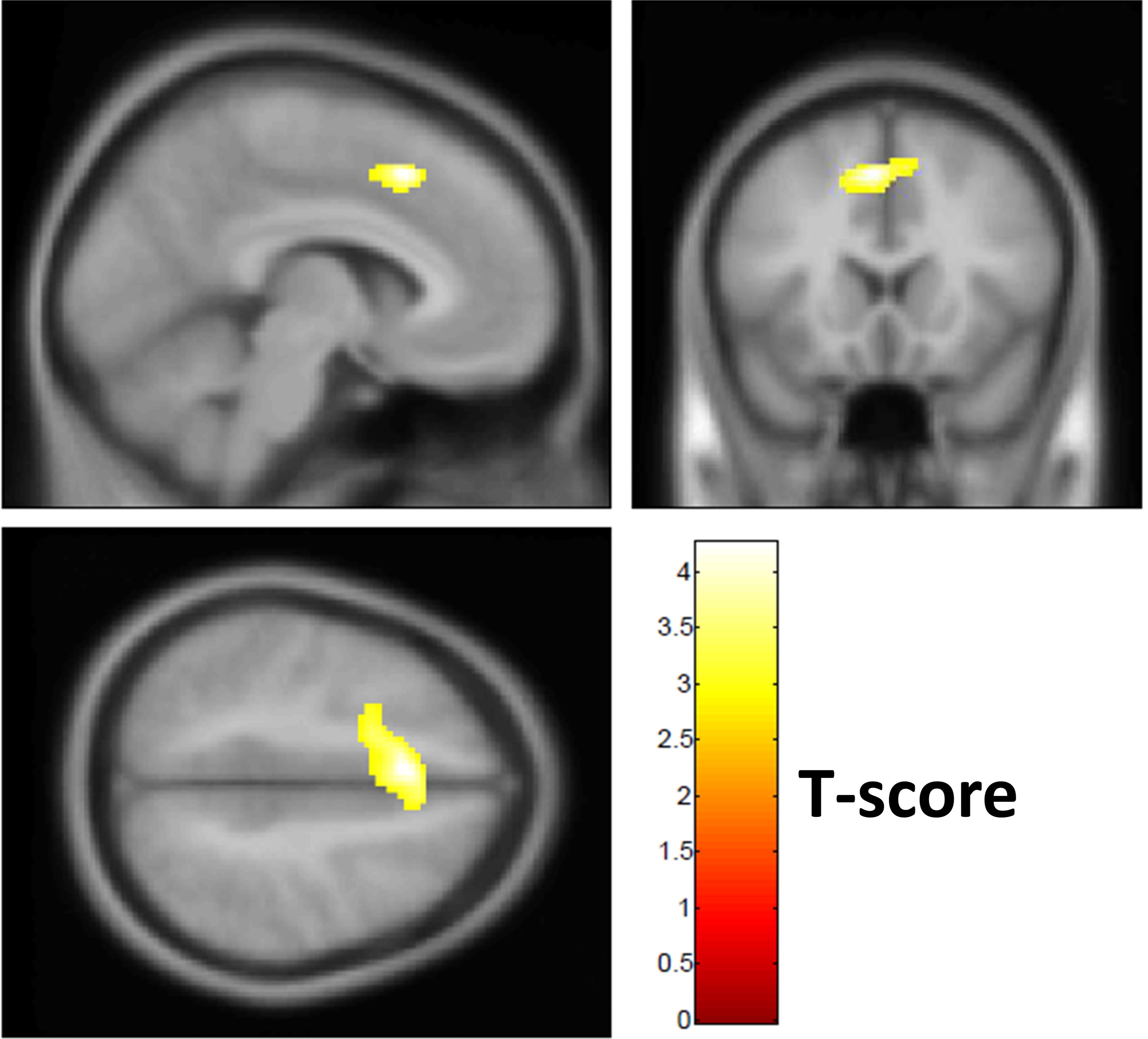
VO2max, an index of cardiorespiratory fitness, increased in the AE group (p=0.03) after one-year, which was unchanged in the ST group (Figure1). Mild improvements in cognitive function, neuropsychiatric symptoms, and ratings of daily activities were observed in the AE group after one-year intervention, whereas no significant changes were observed in the ST group (Table1). Cognitive changes in both groups were minimal, though several reached significance in the AE group. One-year AE led to CVR reduction in the anterior cingulate cortex and adjacent frontal regions (FWE corr. p<0.05) (Figure2) in the AE group, whereas no change was observed in the ST group. VO2max change (Post-Pre) was negatively correlated with change in carotid artery stiffness i.e. a larger increase in VO2max post intervention, was associated with a larger decrease in carotid artery stiffness (Figure3). Positive correlation was observed in all participants between CVR change (Post-Pre) and change in carotid artery stiffness in similar frontal regions, where CVR reduced in the AE group, suggesting that reduction in CVR may be associated with carotid artery stiffness reduction.Conclusions
Cardiorespiratory fitness (VO2max) improved in the AE group that probably led to mild improvements in cognition, neuropsychiatric symptoms and function on daily activities in the AE group. Moderate to vigorous AE intervention for one-year reduced CVR in the anterior cingulate and frontal lobe regions. Interestingly, the very same region revealed an increase in CBF after AE1. Therefore, it may be that AE helped elevate basal perfusion, but in doing that the brain’s ability to further dilate blood vessels in response to CO2 has been diminished. It is also interesting to note that similar observations have been observed in master athletes3. The observed dampening of CO2 reactivity requires further investigation. AE-induced fitness improvement and CVR reduction are associated with lower carotid artery stiffness.Acknowledgements
We would like to thank our funding source: National Institute on Aging - R01 AG033106References
1. Thomas et al. 2020 J. of Alzheimer’s Disease.
2. Hillman et al. 2008 Nat. Rev. Neuroscience.
3. Thomas et al. 2013 JMRI
Figures