4014
Optimizing Temporal Resolution of Dynamic Contrast Enhanced Abdominal MRI Using Deep Learning Reconstruction1GE HealthCare, Boston, MA, United States, 2Department of Radiology, Massachusetts General Hospital, Boston, MA, United States, 3GE HealthCare, Houston, TX, United States
Synopsis
Keywords: Liver, DSC & DCE Perfusion, DISCO-Star, DL Stack-of-stars, Double Wash-in phase
Motivation: Free breathing DCE imaging is beneficial for patients who have difficulty holding their breath, but can be susceptible to artifacts and suboptimal contrast bolus timing, which may compromise diagnostic accuracy.
Goal(s): Our goal was to validate application of deep learning to 3D DISCO-Star imaging in the abdomen after doubling the number of wash-in phases via spoke reordering.
Approach: 8 and 16 wash-in phase images were assessed by two radiologists across different IQ attributes. Noise characteristics were evaluated and AUC was calculated.
Results: The radiologists preferred DL enhanced 16 wash-in phase across many of the IQ attributes, with higher SNR and decreased streaks.
Impact: The ability to double the wash-in phases in DISCO-Star DCE imaging without compromising image quality via deep learning will provide enhanced diagnostic quality, and has the potential to improve patient care.
Introduction
Dynamic contrast-enhanced (DCE) MRI is an essential imaging technique in the assessment of abdominal malignancies1,2. However, the traditional breath-hold approaches utilizing cartesian imaging, such as DISCO, have limitations in some patient populations3,4. Stack-of-stars/radial techniques, such as DSICO-Star and GRASP-VIBE, are motion and respiratory robust free breathing techniques that have become popular in routine DCE imaging2,4–7. However, these free-breathing techniques can be susceptible to artifacts and suboptimal contrast bolus timing, which may compromise diagnostic accuracy4. One advantage with these radial acquisitions is the ability to reorder the acquired spokes to artificially adjust the temporal resolution post-acquisition, although at the expense of increased streak artifacts4. This study aimed to evaluate the effectiveness of a deep learning (DL) reconstruction technique aimed at improving the temporal resolution of free-breathing DCE MRI without loss in image quality.Methods
Fourteen patients underwent free-breathing dynamic contrast-enhanced MRI (DISCO-Star) on a GE Signa Premier XT 3T MRI system (GE HealthCare, Waukesha, WI, USA) as part of a routine liver protocol exam. The scanning parameters were as follows: axial, FOV=38x38cm2, matrix size=256x256, slice thickness/resolution=3mm/50%, # of slices=80, TR/TE=2.9/1.3ms, FA=12 degrees, phase/slice acceleration=1.5/2, 13 total phases. This sequence used a stack-of-stars sampling pattern, which obtained eight sequential contrast wash-in phases spaced 8.3 seconds apart, plus 5 additional delayed phase samples with temporal resolution 37 seconds. Spoke reordering was used to double the number of wash-in temporal samples to 16 retrospectively, resulting in a temporal resolution of 4.2 seconds. A deep learning algorithm (Convolutional Neural Network), trained to denoise, dering, and destreak images, was then applied to the new 16 wash-in phase data8,9. See Figure 1 for overview doubling the wash-in phases and applying DL.Two radiologists independently assessed the image quality of the original 8 phase and 16 phase reconstructed images, with and without DL, in the arterial, portal venous, and transitional phases, using a 5-point Likert scale.
For both DL and non-DL reconstructions of the 16 phase data, the signal-to-noise ratio (SNR) and Total Variation (TV) were calculated10,11. The TV was calculated by computing the gradient across a representative slice with the imgradient function in MATLAB 2022b (MathWorks Inc., Natick, MA) and summing across the 21 total timepoints for that slice. Additionally, the area under the curve (AUC) was calculated for each voxel, as well as an ROI in the liver and kidneys, in the representative slice. Additionally, to assess the change in enhancement offered by the doubling the wash-in phases, the slope of the wash-in curve was compared between the original 8 phases and DL enhanced 16 phases data.
Statistical analysis: separate ordinal logistic regression models summarized using odds ratios and unweighted Fleiss’ Kappa for reader evaluations; paired t-test for quantitative measures with a p-value ≤ 0.05 considered statistically significant.
Results
The study found that the retrospective 16 phase images had a temporal resolution of 4.2 seconds, which was an improvement compared to the prospective 8 phase images. From the radiologists’ perspective, the application of DL to the 16 phase data provided improved overall image quality, with noticeably reduced noise and reduced streaking compared to the 16 phase non-DL data. The 8 phase data generally outperformed the 16 phase non-DL as well. Compared to the 8 phase data, the 16 phase DL data actually matched up well, particularly for Reader 2, with noticeable improvement in the transitional phase. See Table 1 for a statistical breakdown in the reads. Figure 1 shows the timepoints from a representative slice of the liver.Quantitative analysis revealed statistically significant reduction in TV and increased SNR after application of DL (p < 0.001). Figure 2 shows the gradient images from 4/8 timepoints from Figure 1. The AUC within ROIs of the liver/kidney was not significantly different between the DL and non-DL reconstructions, indicating the application of the DL did not distort quantitative measurements. However, the AUC across the whole representative slice was significantly different (p < 0.005), although the mean AUC across the patients was only 1.5% different. See Figures 3 and 4 for the AUC maps and dynamic curves from an ROI in the liver/kidney, respectively. Noticeably, the wash-in phase slope (enhancement) was significantly higher after reducing the temporal resolution two-fold (p = 0.025).
Discussion and Conclusion
The study demonstrated that deep learning reconstruction can be an effective technique to increase the temporal resolution of free-breathing dynamic contrast-enhanced MRI sequences without sacrificing image quality. Future work will focus on evaluating the improved temporal resolution on better identifying focal lesions in the abdomen. The findings have the potential to improve the diagnostic accuracy of free-breathing DCE acquisitions.Acknowledgements
No acknowledgement found.References
1. Kaltenbach B, Roman A, Polkowski C, et al. Free-breathing dynamic liver examination using a radial 3D T1-weighted gradient echo sequence with moderate undersampling for patients with limited breath-holding capacity. European Journal of Radiology. 2017;86:26-32.
2. Yoon JH, Nickel MD, Peeters JM, Lee JM. Rapid Imaging: Recent Advances in Abdominal MRI for Reducing Acquisition Time and Its Clinical Applications. Korean Journal of Radiology. 2019;20(12):1597-1615.
3. Saranathan M, Rettmann DW, Hargreaves BA, Clarke E, Vasanawala SS. DIfferential Subsampling with Cartesian Ordering (DISCO): a High Spatio-temporal Resolution Dixon Imaging Sequence for Multiphasic Contrast Enhanced Abdominal Imaging. Journal of Magnetic Resonance Imaging. 2012;35(6):1484-1492.
4. Ichikawa S, Motosugi U, Wakayama T, et al. An Intra-individual Comparison between Free-breathing Dynamic MR Imaging of the Liver Using Stack-of-stars Acquisition and the Breath-holding Method Using Cartesian Sampling or View-sharing. Magnetic Resonance in Medical Sciences. 2023;22(2).
5. Ichikawa S, Motosugi U, Kromrey ML, et al. Utility of Stack-of-stars Acquisition for Hepatobiliary Phase Imaging without Breath-holding. Magnetic Resonance in Medical Sciences. 2020;19(2).
6. Zins M, Legou F. In pursuit of fast and consistent free-breathing abdominal MR exams. Signa Pulse of MR. 2020.
7. Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI: iGRASP: Iterative Golden-Angle RAdial Sparse Parallel MRI. Magn Reson Med. 2014;72(3):707-717. doi:10.1002/mrm.24980
8. Wang X, Lee Y, Lee J, et al. Convolutional Neural Network based Stack-of-Star Imaging with Noise and Artifacts Removal. In: Proceedings of the 31st Annual Meeting of the International Society for Magnetic Resonance in Medicine (ISMRM). Toronto, Ontario, Canada; 2023.
9. Park EJ, Lee Y, Lee HJ, et al. De-streaking effect Deep Learning Reconstruction in free-breathing dynamic contrast enhanced Liver MRI. In: Proceedings of the 31st Annual Meeting of the International Society for Magnetic Resonance in Medicine (ISMRM). Toronto, Ontario, Canada; 2023.
10. Rudin LI, Osher S, Fatemi E. Nonlinear total variation based noise removal algorithms ☆. Physica D: Nonlinear Phenomena. 60(1-4).
11. Block KT, Uecker M, Frahm J. Suppression of MRI Truncation Artifacts Using Total Variation Constrained Data Extrapolation. International Journal of Biomedical Imaging. 2008;2008.
Figures
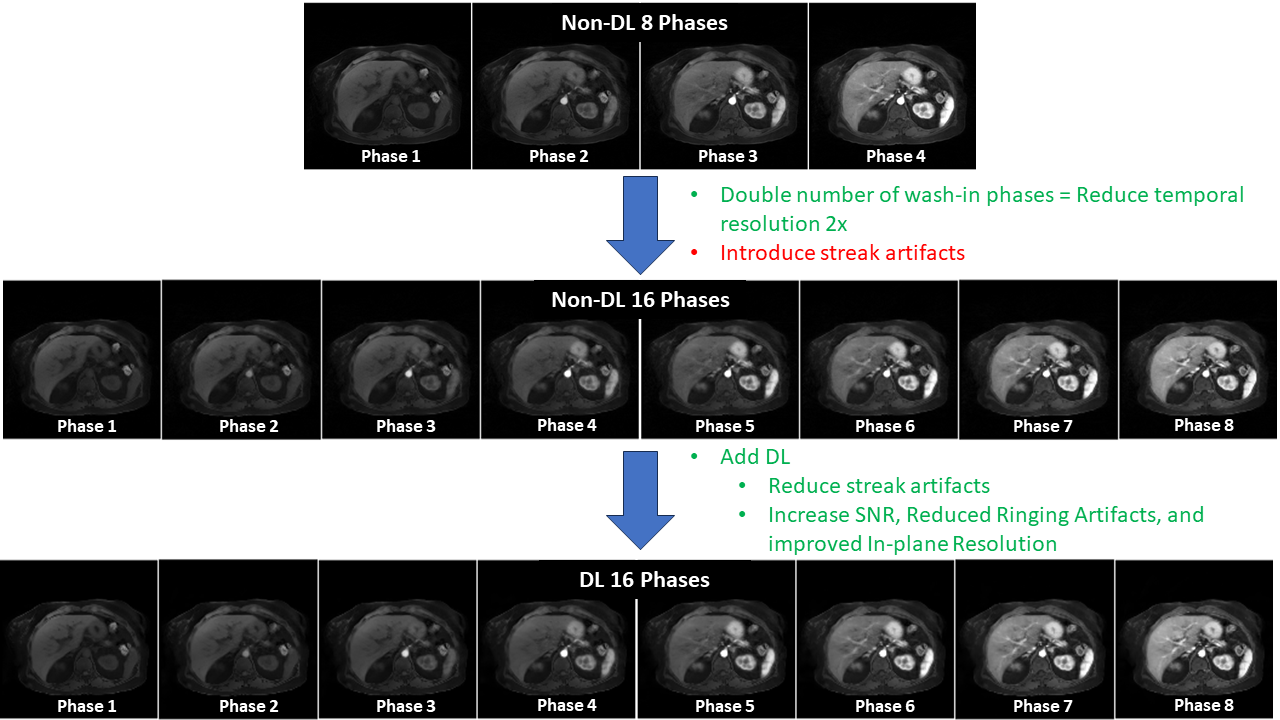
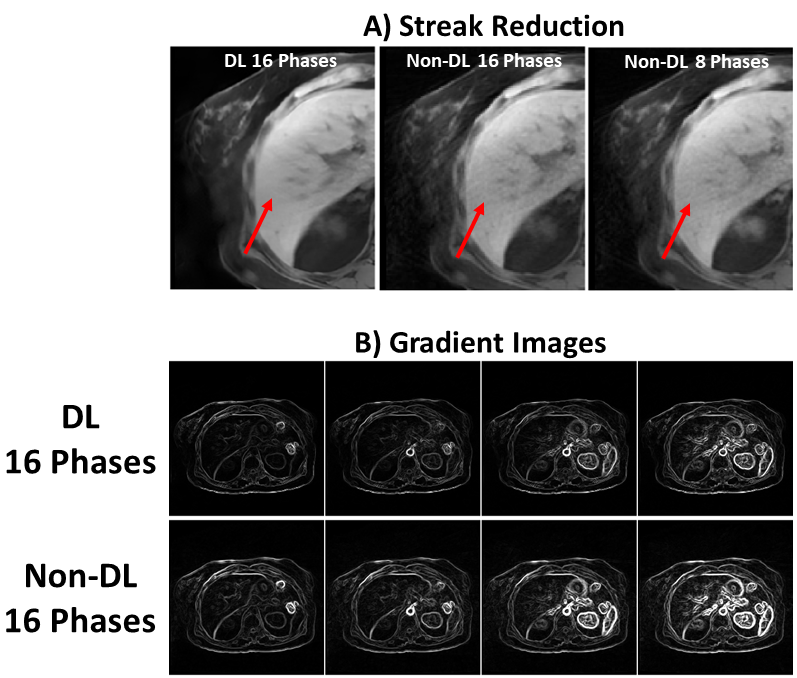
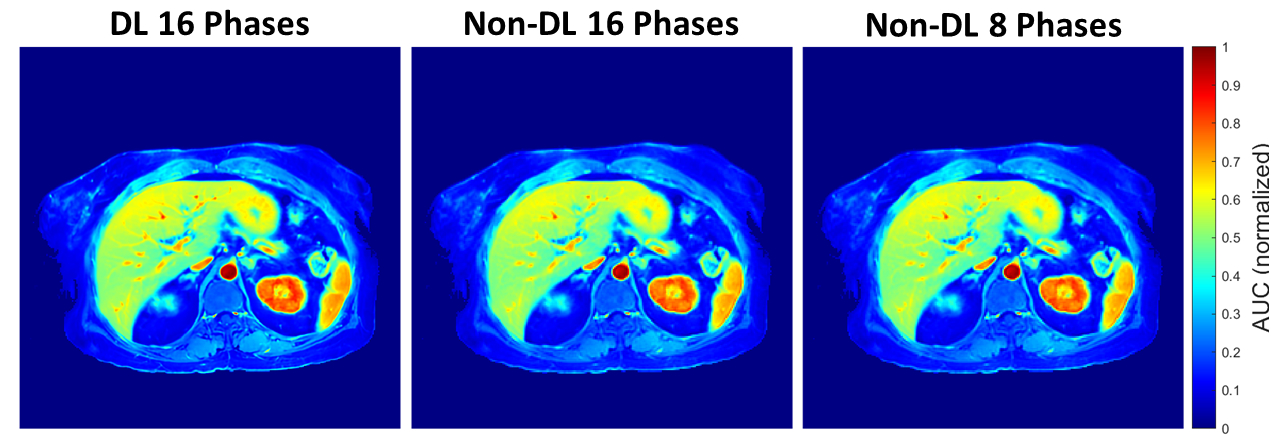
Figure 3: Example DL and non-DL (16 and original 8 phase) AUC maps from the patient in Figures 1 and 2. Visually, the AUC maps look very similar to each other, particularly in the liver and kidneys. The mean difference between the AUC across the whole images was 1.5%.
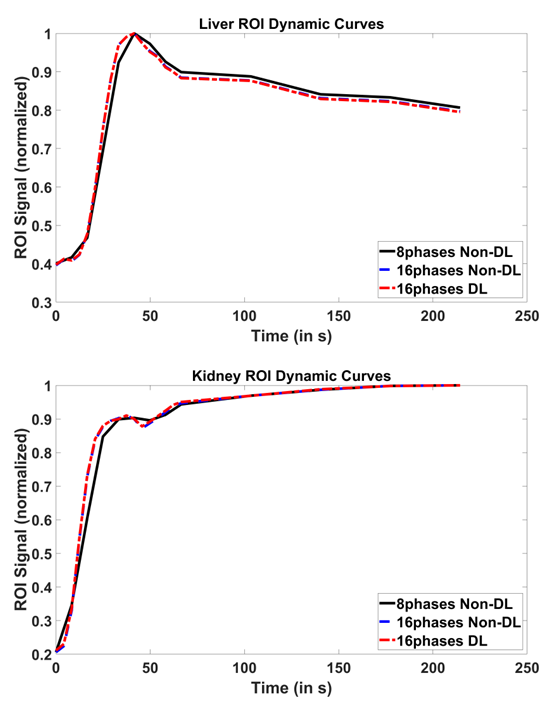
Figure 4: Example DL and non-DL dynamic curves from an ROI in the liver and kidneys of the patient in Figure 2. The curves match well across all timepoints, indicating application of DL does not distort quantitative analysis of DSICO-Star data. The 16 phase curves have higher slope than the original 8 phase curve, showing significant added information on enhancement in the ROI with the 2x improved temporal resolution.
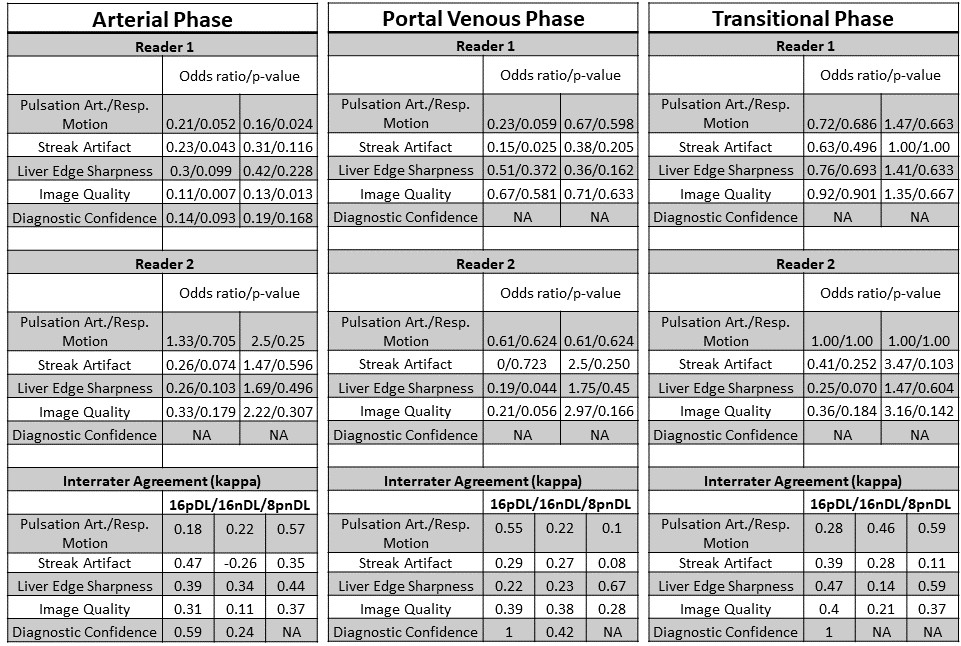
Table 1: Statistical analysis results for the radiologists’ reads. These values may be interpreted as the increase in odds when comparing 8 phases non-DL (reference) and 16 phase (non-DL and DL) (OR is > 1, 16 phase better than 8 phase). The left column under odds ratio/p-value is 16 phase non-DL vs. 8 phase. The right column under odds ratio/p-value is 16 phase DL vs. 8 phase. The 16 phase DL outperformed the 16 phase non-DL, but was comparable to the 8 phase data. Reader 2 appeared to prefer the DL more often than Reader 1 across the IQ characteristics and three different phases.