4013
Deep Learning Accelerated HASTE Sequence with denoising effect for the Evaluation of Pancreatic Cystic Lesions1Radiology, Korea University Guro Hospital, Seoul, Korea, Republic of, 2Korea University Guro Hospital, Seoul, Korea, Republic of
Synopsis
Keywords: Pancreas, Pancreas
Motivation: Single-shot technique such as HASTE with one breath-hold and thin section images reconstructed by DL may allow detection and detailed characterization of pancreas cystic lesions.
Goal(s): This study was aimed to assess the feasibility of single breath-hold HASTE using DLR with additional denoising effect for the evaluation of pancreas cystic lesions.
Approach: Four HASTE sequences with/without DLR were obtained. Two radiologists independently reviewed four image sets for qualitative and quantitative analyses of image quality.
Results: HASTE using DL with additional denoising showed higher image quality than conventional HASTE in both qualitative and quantitative analyses. It also showed lower variability in cyst size measurement.
Impact: DL-accelerated HASTE sequence with denoising effect may be useful for reducing acquisition time with one-breath hold without compromising image quality in the evaluation of pancreatic cystic lesions. It may be applied to abbreviated MRI for follow-up of pancreatic cystic lesions.
The aim of this study was to assess the feasibility of single breath-hold half-Fourier single-shot turbo spin echo (HASTE) using deep learning reconstruction (DLR) with additional denoising effect for the evaluation of pancreas cystic lesions.
Materials and Methods
Patients
A total 142 patients who underwent pancreas MRI were consecutively recruited from March 2021 and April 2021. Among these patients, 79 patients were excluded due to (a) cancer evaluation (n=48), (b) previous pancreatic surgery (n=22), and (c) severe atrophic change of pancreatic parenchyma (n=9). Finally, 63 patients who underwent pancreas MRI (34 men and 29 women; mean age, 63.16 ± 12.1 years; range, 35–88 years) were included.
MRI examinations
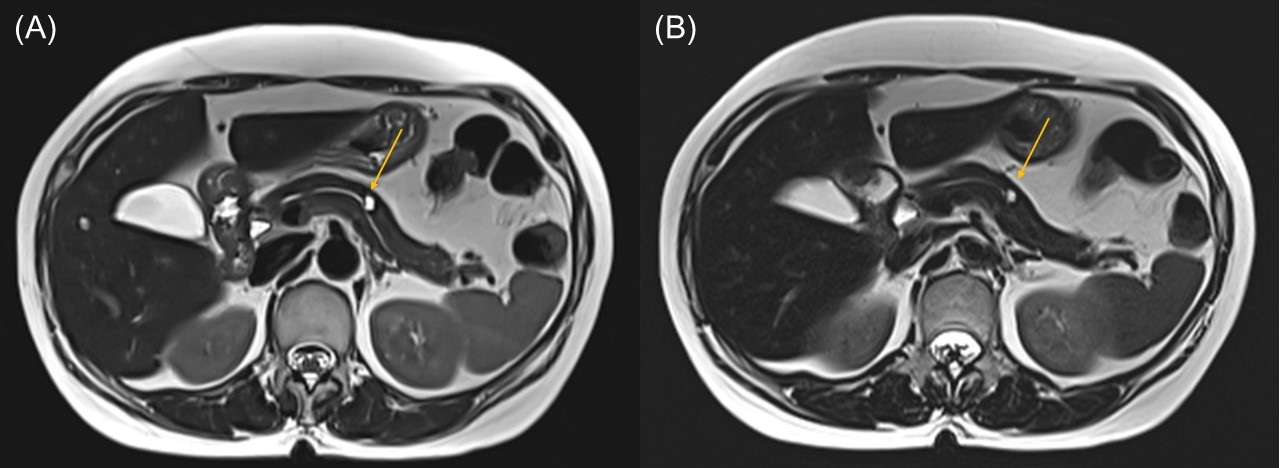
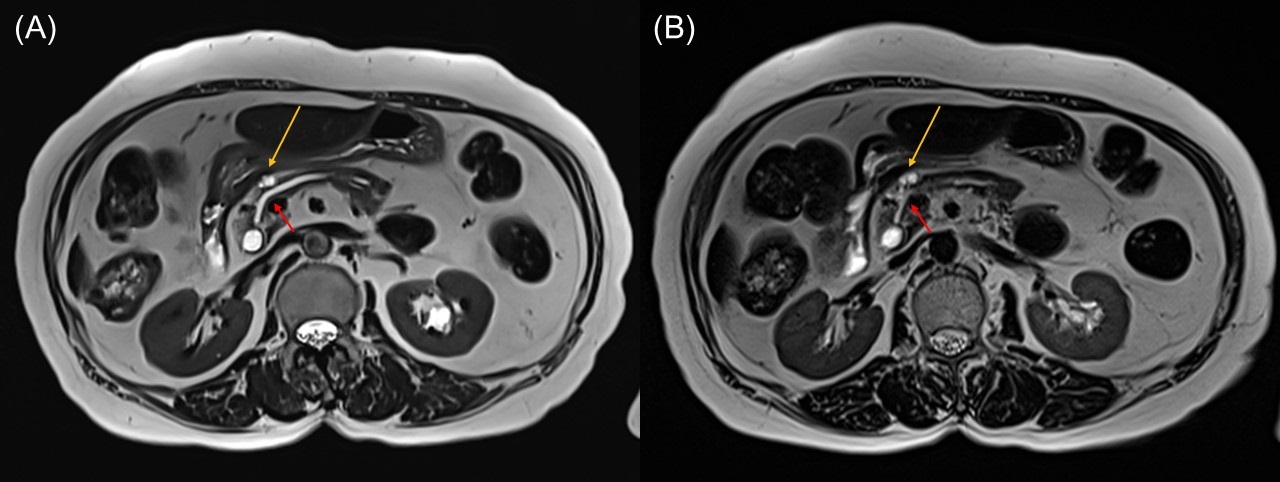
MRI imaging was performed with a 3.0-T MR scanner (MAGNETOM Skyra; Siemens Healthineers, Erlangen, Germany). Two non-fat-suppressed T2-weighted images were obtained: a conventional multiple breath-hold HASTE (non-FS conventional HASTE) and a single breath-hold HASTE using DLR with additional denoising effect (non-FS HASTEDL with denoising). In addition, two fat-suppressed T2-weighted images were acquired using DLR: a single breath-hold HASTE with additional denoising effect (FS HASTEDL with denoising) and HASTE without denoising effect (FS HASTEDL without denoising). Vendor-provided DL algorithms were used to reconstruct and denoise the HASTE images. The acquisition time of conventional HASTE was 65 seconds with multi-breath hold, and that of HASTEDL sequences was 18 seconds with one breath hold.
Image quality analysis
Two board-certified abdominal radiologists independently reviewed four image sets (non-FS conventional HASTE, non-FS HASTEDL with denoising, FS HASTEDL with denoising, and FS HASTEDL without denoising) for the evaluation of image quality.
For the quantitative image quality analysis, signal-to-noise ratio (SNR) of pancreatic cystic lesions and parenchyma, and contrast-to-noise ratio (CNR) between pancreatic cystic lesion and normal pancreas parenchyma were calculated for the four image sets.
For the qualitative image quality analysis, the reviewers independently evaluated sharpness of the pancreas edge, sharpness of pancreatic duct, pancreatic cystic lesion conspicuity, artifacts (blurring, respiratory motion, pulsation, or chemical shift artifacts), and overall image quality for two non-FS image sets (conventional HASTE vs. HASTEDL with denoising) using a 4-point Likert scale (1=poor; 2=fair or moderate; 3=good; 4=excellent).
Additional qualitative analyses were conducted for non-FS conventional HASTE and HASTEDL with denoising as follows: Patency of main pancreatic duct (MPD) using a 4-point Likert scale and degree of misregistration artifact using a 4-point scale.
Pancreatic cystic lesion assessment
The same two radiologists independently reviewed the four image sets for evaluation of characterization of pancreatic cystic lesions. Total number of pancreatic cystic lesions was counted. The size of the largest cyst was measured. In addition, the diameter of MPD was also measured.
Results
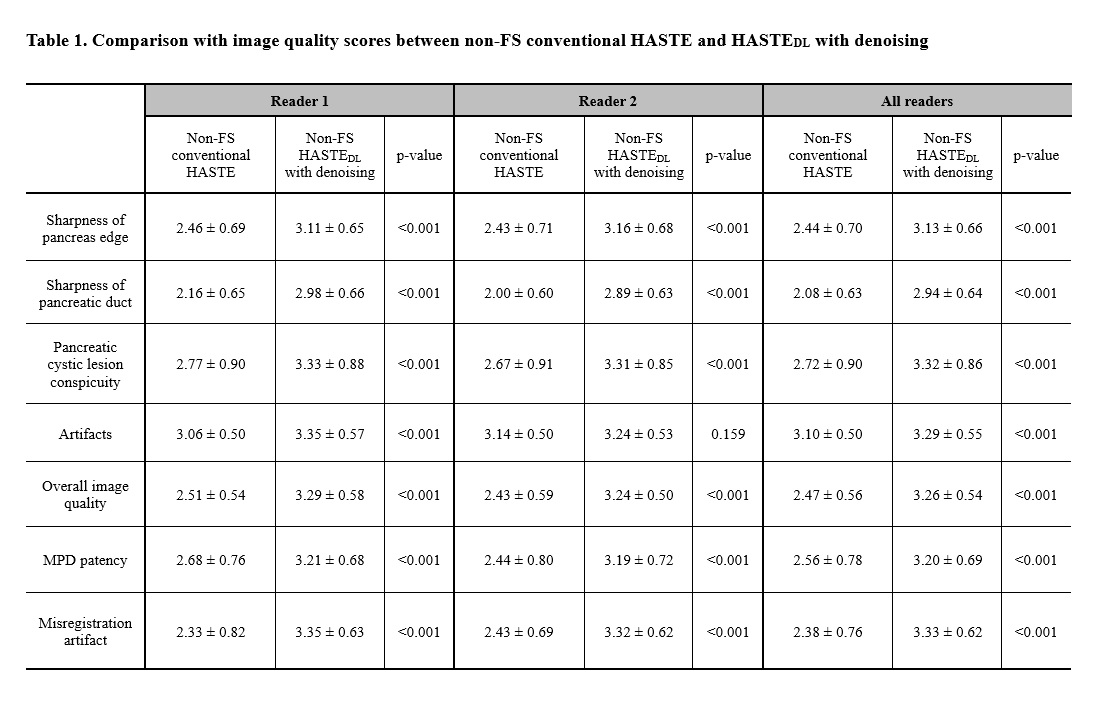
Inter-reader agreement between the two readers for the all image quality parameters was excellent for non-FS conventional HASTE sequence (ICC, range 0.762–0.956) and good to excellent for HASTEDL with denoising sequence (ICC, range 0.743–0.916). The qualitative analyses of image quality parameters for non-FS conventional HASTE and HASTEDL with denoising sequences by the two readers are summarized in Table 1 (Figure 3). The mean score for overall image quality of non-FS HASTEDL with denoising sequence was significantly higher than non-FS conventional HASTE sequence (3.26 ± 0.54 vs. 2.47 ± 0.56, p<0.001) (Figure 1 and Figure 2). In addition, HASTEDL with denoising sequence received higher scores from both readers in terms of MPD patency and misregistration artifact (Figure 3, Table 1).
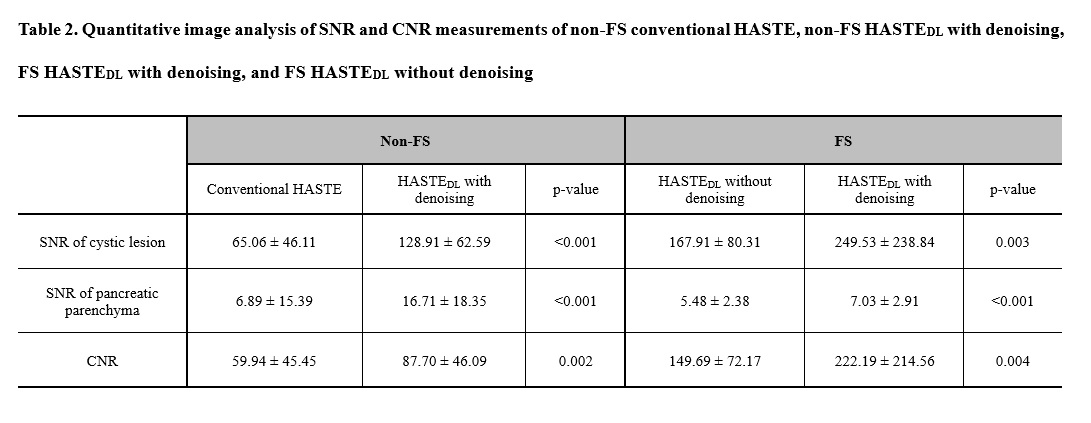
The quantitative analyses of image quality parameters are summarized in Table 2 (Figure 4). The SNR of the pancreatic cystic lesion and pancreatic parenchyma was significantly higher in non-FS HASTEDL with denoising sequence than in conventional HASTE sequence (128.91 ± 62.59 vs. 65.06 ± 46.11, p<0.001 and 16.71 ± 18.35 vs. 6.89 ± 15.39, p<0.001). Additional denoising effect also significantly increased the SNR of the pancreatic cystic lesion and pancreatic parenchyma in the FS HASTEDL sequence (249.53 ± 238.84 vs. 167.91 ± 80.31, p = 0.003 and 7.03 ± 2.91 vs. 5.48 ± 2.38, p <0.001).
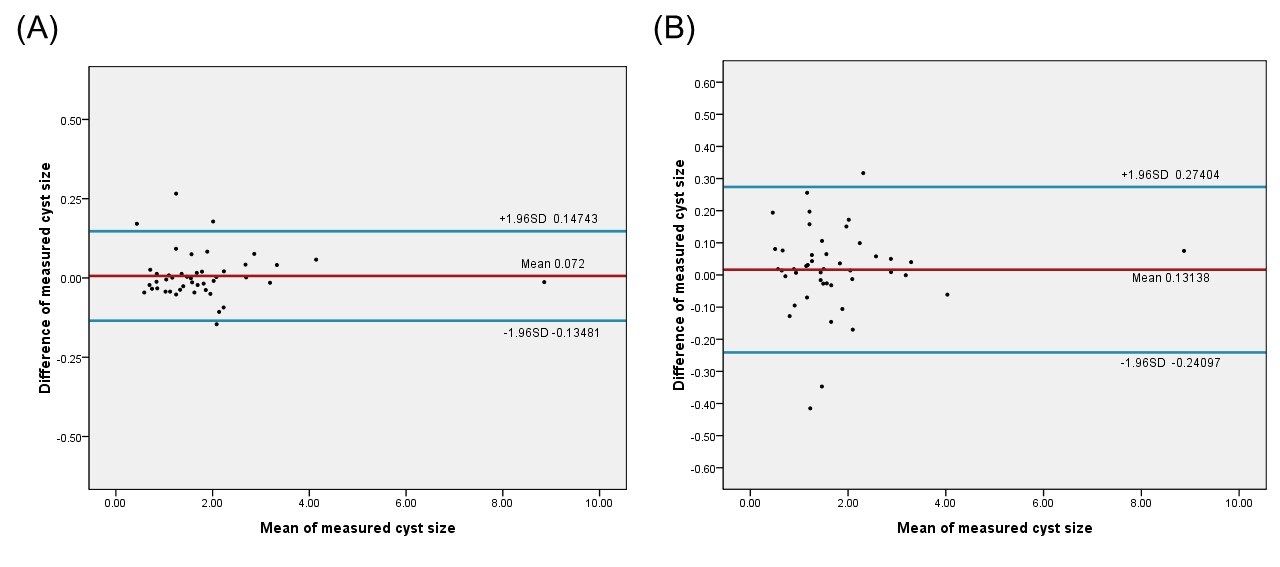
In the reproducibility analysis of cyst size, both conventional HASTE and HASTEDL with denoising showed almost perfect inter-reader agreement, but the ICC of conventional HASTE was lower than that of HASTEDL with denoising (0.995 vs. 0.999). The 95% limits of agreement (LoA) in the Bland-Altman analysis for HASTEDL with denoising was narrower in cyst size measurement than that for conventional HASTE (95% LoA, -0.13481 to 0.14743 vs. -0.24097 to 0.27404) (Figure 5).
Conclusion
Deep learning accelerated HASTE sequence with denoising effect may be useful for reducing acquisition time of pancreas MRI with one-breath hold without compromising image quality in the evaluation of pancreatic cystic lesions.
Acknowledgements
No acknowledgement found.References
1. Herrmann J, Gassenmaier S, Nickel D, Arberet S, Afat S, Lingg A, Kündel M, Othman AE. Diagnostic Confidence and Feasibility of a Deep Learning Accelerated HASTE Sequence of the Abdomen in a Single Breath-Hold. Invest Radiol. 2021;56(5):313-319.
2. Kalb B, Sarmiento JM, Kooby DA, Adsay NV, Martin DR. MR imaging of cystic lesions of the pancreas. Radiographics. 2009;29(6):1749-65.
3. Shanbhogue K, Tong A, Smereka P, Nickel D, Arberet S, Anthopolos R, Chandarana H. Accelerated single-shot T2-weighted fat-suppressed (FS) MRI of the liver with deep learning-based image reconstruction: qualitative and quantitative comparison of image quality with conventional T2-weighted FS sequence. Eur Radiol. 2021;31(11):8447-8457.
Figures