4012
Advancing Free-Breathing Liver MRI at 7T with Pseudo-Spiral Cartesian Sampling and Phase-Shimming1Electrical and Computer Engineering, McMaster University, Hamilton, ON, Canada, 2Imaging Research Centre, St. Joseph’s Healthcare Hamilton, Hamilton, ON, Canada, 3Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands, 4Spinoza Center for Neuroimaging, Amsterdam, Netherlands, 5Computational Cognitive Neuroscience and Neuroimaging, Netherlands Institute for Neuroscience, KNAW, Amsterdam, Netherlands, 6School of Biomedical Engineering, McMaster University, Hamilton, ON, Canada, 7Department of Radiology, McMaster University, Hamilton, ON, Canada, 8Biomedical Engineering and Physics, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
Synopsis
Keywords: Liver, Liver, Free-Breathing, Pseudo-Spiral, 7T, Phase-Shimming
Motivation: Ultra-high field (B0 ≥ 7T) MRI potentially offers high spatial resolution. However, 7T abdominal MRI is challenging due to B1+-inhomogeneities and patients’ breath-holding limits, especially for high-resolution scans.
Goal(s): To develop a high-quality, free-breathing liver scan at 7T.
Approach: We implemented a 3D-GRE with golden-angle pseudo-spiral sampling pattern at 7T, that allowed respiratory binning in a free-breathing acquisition followed by Compressed Sensing reconstruction. Phase-shimming was used to achieve a homogeneous signal intensity over the liver.
Results: We successfully achieved 1.35x1.35x1.35mm3-resolution liver images with high image quality, including signal homogeneity over the entire liver, demonstrating the potential of free-breathing 7T liver MRI.
Impact: This study addresses breath-holding and B1+-inhomogeneity challenges associated with 7T abdominal MRI. It could further the development of non-invasive and detailed liver visualization. Ultimately, this would alter clinical pathways and offer patients a more comfortable imaging experience.
Introduction
Ultra-high field (UHF; B0 ≥ 7T) MRI has the potential to significantly improve abdominal imaging thanks to the higher SNR, which can be traded for higher spatial resolution. However, the B1+-inhomogeneities associated with 7T become particularly troublesome when imaging large Fields of View (FOVs), such as the human abdomen. Additionally, for high-resolution imaging, the scan durations quickly exceed the practical limits of patient breath-holding. Recent advancements have demonstrated that parallel transmission, using eight transmit channels, can substantially improve image homogeneity in the abdomen at UHF, provided that accurate B1+-maps are available1,2. To achieve high spatial resolution, and to ease the inconvenience of breath-holding techniques for patients, here we developed a phase-shimmed, free-breathing liver scan with a golden-angle pseudo-spiral acquisition that allows retrospective respiratory binning.Methods
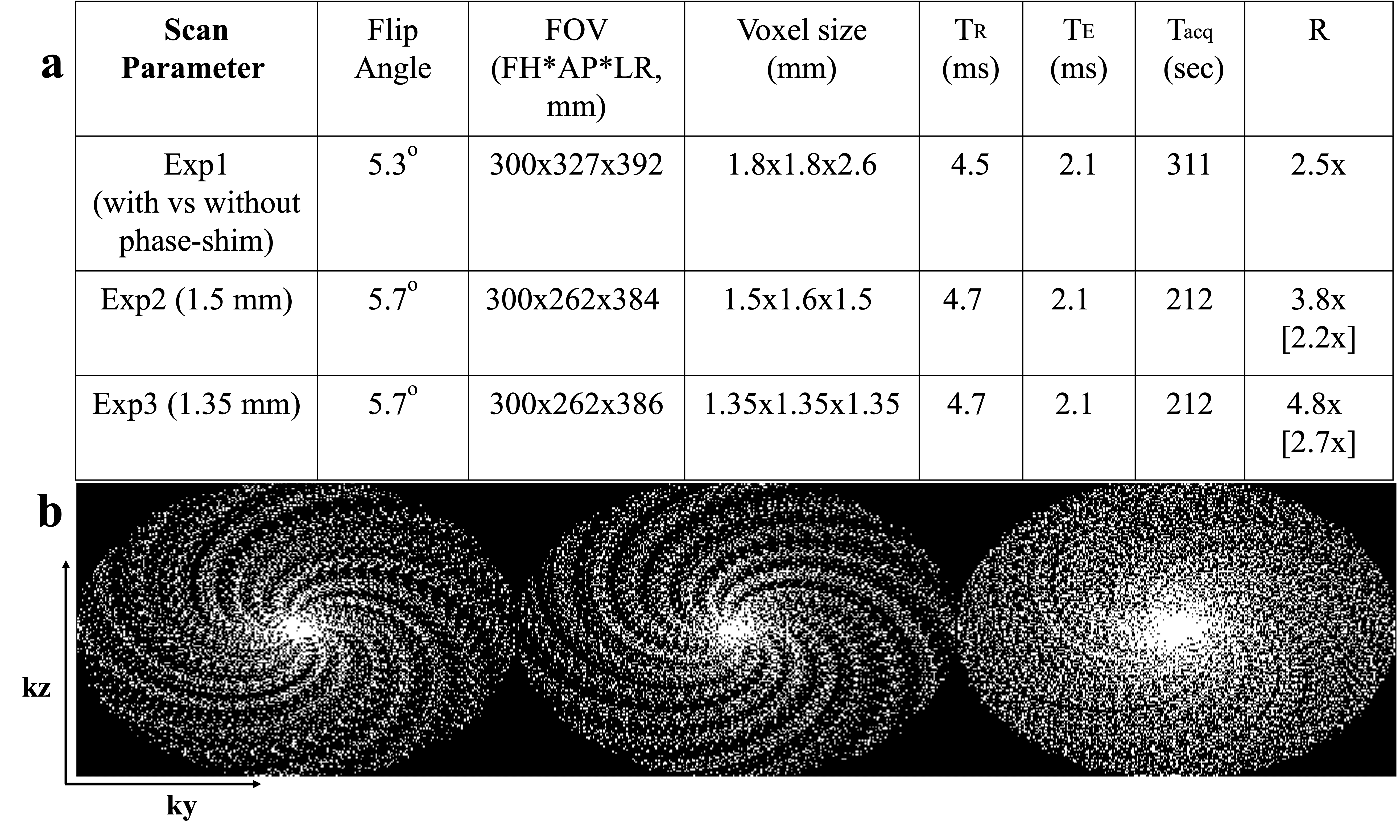
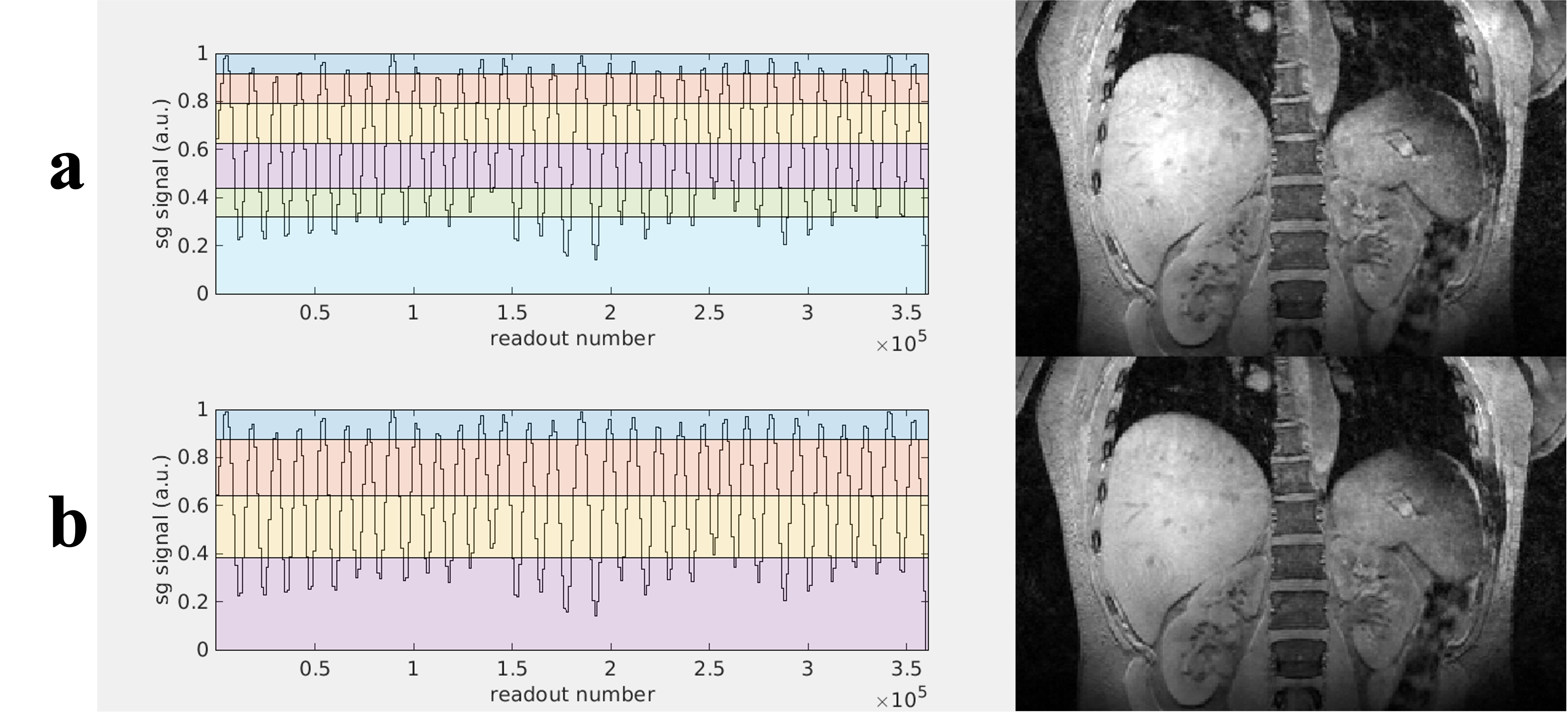
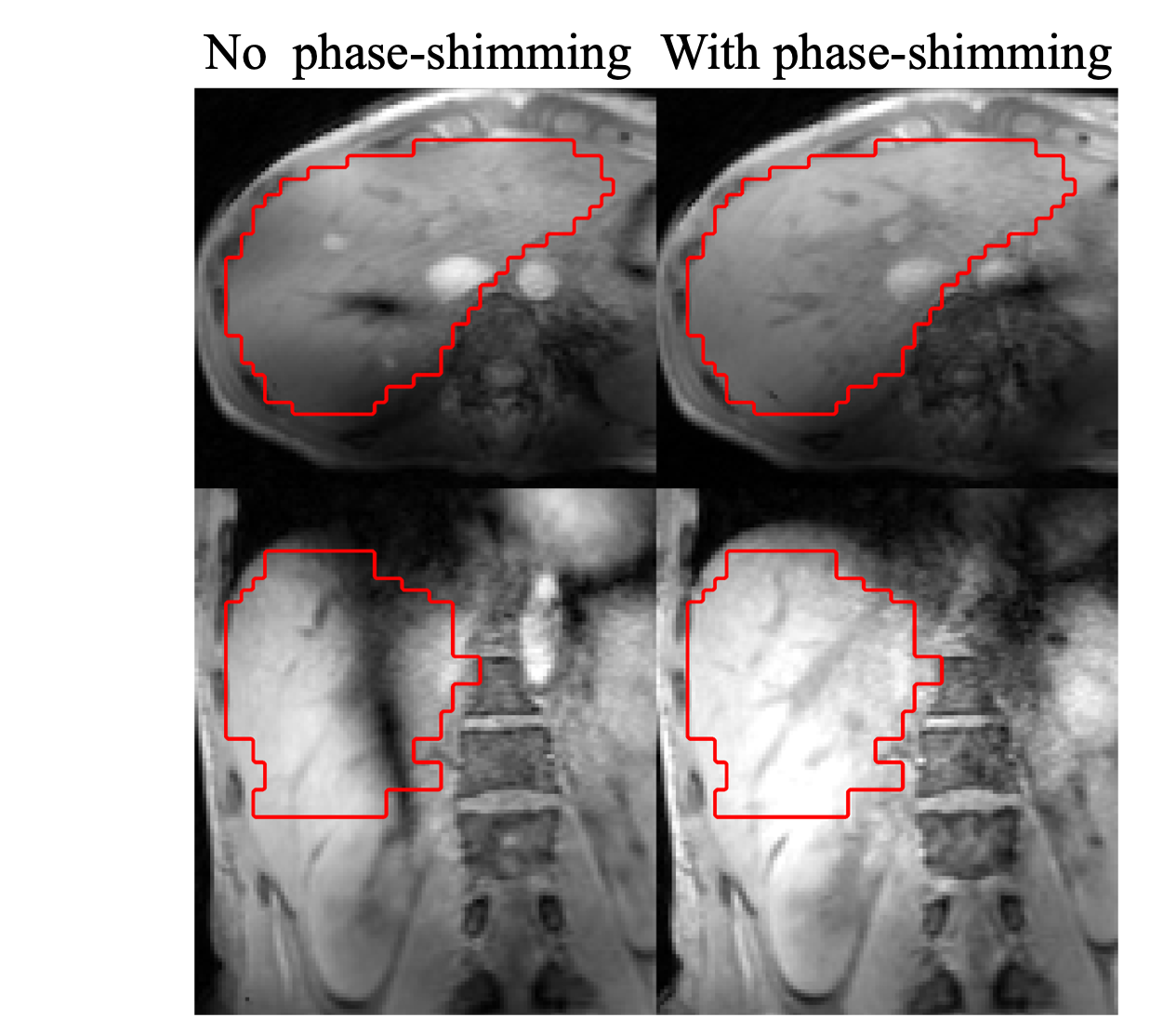
A 7T MRI scanner (Philips Healthcare, Best, The Netherlands) with the PROspective Undersampling in multiple Dimensions (PROUD) patch3 was used to acquire prospectively undersampled free-breathing liver data from two healthy participants, using a golden-angle pseudo-spiral sampling pattern with spiral arms of 25 points each (Figure 1). For respiratory binning, the k-space center was sampled every 150 lines, with the readout direction along the feet-head direction (z-axis). See Figure 1 for other sequence parameters. Gradient-echo images (GREs) were acquired using eight-channel parallel transmission. Phase offsets minimizing the flip-angle coefficient of variation were calculated based on Fourier PE-DREAM4 B1+-mapping with 13 phase-encoding steps acquired in separate breath-holds. Phase-shim and 2nd order B0-shim values were calculated in a manually drawn liver volume-of-interest. To illustrate phase-shimming efficacy, we acquired example GREs with and without phase-shimming. A respiratory binning technique using the profiles generated from repeatedly sampled center k-space lines5 was employed prior to Compressed Sensing (CS) reconstruction6. To reduce the raw data size per scan, we combined two separate acquisitions with complementary sampling patterns. Raw data were processed offline using ReconFrame (Gyrotools, Zurich, Switzerland) and BART7. To evaluate the effect of bin size on image quality, respiratory binning with 4 (reduction factor (R) = 4.8) and 6 (R=6.8) bins were compared for data with a resolution of 1.35 mm isotropic. Subsequently, ESPIRiT8 receive coil sensitivity maps were estimated using 20×20 k-space calibration lines. Finally, CS image reconstruction was conducted using BART’s ‘pics’ command, with the wavelet transform as the sparsifying operator. For optimization, the reconstruction results using 25 L1 regularization factor values logarithmically sampled between 0.00001 and 0.1 were compared. A regularization factor of 0.0068 for the separate dataset and 0.0032 for the combined dataset provided the best image quality upon visual inspection. This approach was exclusively applied to data acquired during the expiration phase, selected because B0- and phase-shimming were performed on data acquired during a breath hold at expiration.Results
Figure 2 illustrates the respiratory binning process. Here, binning over either 4 or 6 respiratory phases was compared. A binning factor of 4 resulted in slightly higher-quality reconstructed images (Figure 2b), making it the preferred option for subsequent comparisons.Figure 3 demonstrates the advantage of phase-shimming. Notably, phase-shimming addresses the artifacts associated with B1+-inhomogeneity in abdominal imaging at 7T by moving the signal voids outside the volume-of-interest. Hence, phase-shimming had a key role in enhancing image quality.
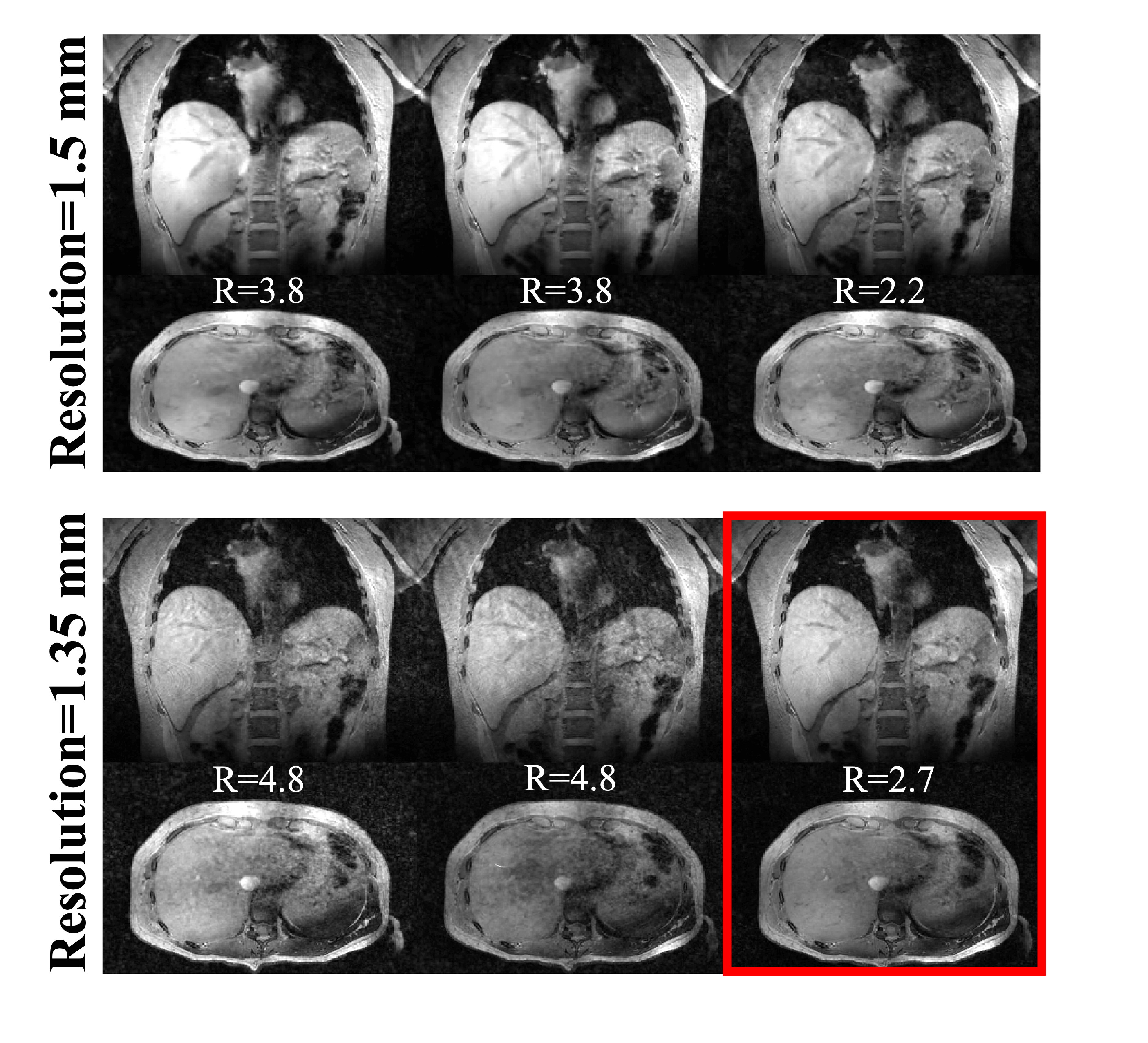
In Figure 4, data acquired at spatial resolutions of 1.5 and 1.35 mm isotropic are compared. Both datasets are shown before (left, middle) and after (right) combinations of the two distinct acquisitions. SNR is already acceptable in a single 3-minute scan for 1.5 mm-isotropic resolution, while the combination of the two leads to image blurring. In contrast, a clear improvement in image quality is noticeable for the 1.35 mm isotropic resolution data, where fine details of the liver are more discernible in the combined dataset.
Finally, Figure 5 showcases the image quality achieved in this free-running, free-breathing 1.35 mm isotropic resolution 7T abdominal acquisition, reconstructed in four bins, cycling through all slices.
Discussion and Conclusion
In this work, a free-running, free-breathing, high-resolution, prospectively undersampled 3D GRE sequence was proposed for 7T liver imaging. The combination of phase-shimming, golden-angle pseudo-spiral undersampling, and compressed sensing reconstruction allowed 1.35 mm isotropic resolution acquisitions with high image quality of the entire liver at 7T. Combining multiple scans, each with a unique sampling pattern, allowed sampling of large data matrices within database capacity. The results of this study improve the feasibility of abdominal imaging at UHF and pave the way for future explorations aimed at utilizing this technique in a more clinical setting. For example, the visualization of small liver metastases could benefit from enhanced spatial resolution in a patient-friendly, free-breathing acquisition such as that described here.Acknowledgements
We gratefully acknowledge the support of the ISMRM through the ISMRM Research Exchange Program. This grant has been instrumental in facilitating our research and enabling us to present our findings within the esteemed community of ISMRM.References
1. Runderkamp BA, Roos T, van der Zwaag W, Strijkers GJ, Caan MW, Nederveen AJ. Whole‐liver flip‐angle shimming at 7 T using parallel‐transmit k T‐point pulses and Fourier phase‐encoded DREAM B1+ mapping. Magnetic resonance in medicine. 2023 Oct 5.
2. Rietsch SH, Orzada S, Maderwald S, Brunheim S, Philips BW, Scheenen TW, Ladd ME, Quick HH. 7T ultra‐high field body MR imaging with an 8‐channel transmit/32‐channel receive radiofrequency coil array. Medical physics. 2018 Jul;45(7):2978-90.
3. Gottwald LM, Peper ES, Zhang Q, Coolen BF, Strijkers GJ, Nederveen AJ, van Ooij P. Pseudo‐spiral sampling and compressed sensing reconstruction provides flexibility of temporal resolution in accelerated aortic 4D flow MRI: A comparison with k‐t principal component analysis. NMR in Biomedicine. 2020 Apr;33(4):e4255.
4. Tse DH, Poole MS, Magill AW, Felder J, Brenner D, Shah J. Encoding methods for B1+ mapping in parallel transmit systems at ultra high field. Journal of Magnetic Resonance (San Diego, Calif.: 1997). 2014 Jun 28;245:125-32.
5. Merton R, Bosshardt D, Strijkers GJ, Nederveen AJ, Schrauben EM, van Ooij P. Reproducibility of 3D thoracic aortic displacement from 3D cine balanced SSFP at 3 T without contrast enhancement. Magnetic resonance in medicine. 2023 Oct 13.
6. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2007 Dec;58(6):1182-95.
7. Uecker M, Ong F, Tamir JI, Bahri D, Virtue P, Cheng JY, Zhang T, Lustig M. Berkeley advanced reconstruction toolbox. InProc. Intl. Soc. Mag. Reson. Med 2015 May 30 (Vol. 23, No. 2486).
8. Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT—an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magnetic resonance in medicine. 2014 Mar;71(3):990-1001.
Figures