4011
Non-contrast Portal Venous 4D Flow MRI in an Obese Cohort Undergoing Weight Loss Surgery: Feasibility and Correlations with BMI and MASH1Department of Radiology, University of Wisconsin-Madison, Madison, WI, United States, 2Department of Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 3University of California San Diego, San Diego, CA, United States, 4University of Wisconsin-Madison, Madison, WI, United States, 5Pfizer, Cambridge, MA, United States
Synopsis
Keywords: Liver, Velocity & Flow
Motivation: To evaluate the potential of portal flow as a biomarker of metabolic-dysfunction associated steatohepatitis (MASH) in obese patients undergoing weight loss surgery (WLS).
Goal(s): Determine feasibility of portal non-contrast 4D Flow in obese patients, to assess whether flow is impacted by BMI and the presence of MASH.
Approach: Portal flow was quantified at 5 timepoints before and after WLS. Mass conservation and inter-observer agreement assessed validation. Results were correlated with BMI and presence/absence of biopsy-proven MASH.
Results: Non-contrast 4D Flow was successful in 339/382 exams (87%); BMI correlated with portal flow (p=0.010); flow was significantly higher in MASH (p=0.013, AUC=0.706)
Impact: Our work demonstrates the feasibility of
non-contrast 4D flow in individuals with obesity. Further, it indicates
possible effects of obesity on portal venous flow and demonstrates its
potential as a treatment monitoring tool in MASH.
Introduction
Individuals with obesity are responsible for ~50% of patients with metabolic-dysfunction associated steatotic liver disease (MASLD), which affects ~25-30% of the world's population1,2. MASLD, and its aggressive subtype, metabolic-dysfunction associated steatohepatitis (MASH), are emerging as the leading cause of cirrhosis3. Cirrhosis induces significant liver blood flow changes3,4 which, if proven in MASH or MASLD5, may serve as biomarker(s) for MASLD/MASH5.Weight loss surgery (WLS) is effective in reducing weight and treating MASLD in obese individuals6-9; however, concomitant effects on liver blood flow are relatively unexplored. Portal venous flow changes in cirrhosis have been quantified using contrast-enhanced 4D Flow MRI3,10 and may serve as a biomarker to monitor MASH treatment-response. However, imaging individuals with obesity is challenged by the presence of fat signal in adipose tissue and lower signal-to-noise ratio (SNR)11, which may confound results.
The purpose of this study was to demonstrate feasibility of non-contrast 4D flow in patients with obesity undergoing WLS. Secondary aims were to determine whether portal venous flow can identify patients with MASH and to investigate possible correlations between BMI and mean portal flow.
Methods
This ongoing, IRB-approved study included patients with BMI>35kg/m2 scheduled for WLS between 12/2020-9/2023 at the Universities of Wisconsin-Madison and California San Diego. Enrolled participants were imaged 5 times: before starting a 2-week low-calorie pre-surgery diet, 1-2 days before surgery with an intraoperative liver biopsy, and 12-, 26-, and 52-weeks post-surgery. Histologic MASLD/MASH diagnoses were made in consensus by two board-certified pathologists.Non-contrast 4D Flow MRI was acquired at 3.0T (GE Healthcare, Waukesha, WI) after 12 hours of fasting using a 5-point encoded radially under-sampled trajectory (PC-VIPR)12,13 covering the upper abdomen: imaging volume=48x48x24cm3; isotropic resolution=1.25mm14; flip=6˚; duration=11min; TR/TE=6.5ms/2.4ms; velocity encoding=60cm/s; fat saturation; retrospective ECG and respiratory gating.
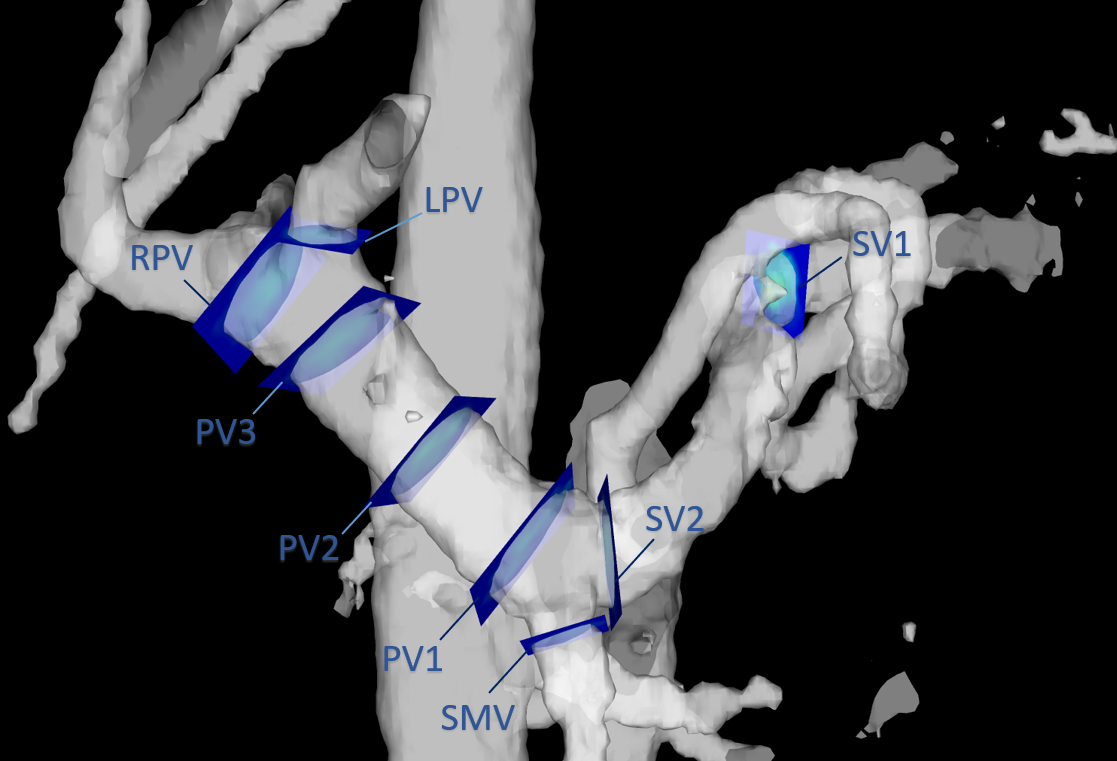
Offline CINE-reconstruction (conjugate gradient iterative SENSE15, 14 frames) was performed. Polynomial background phase correction16 was applied using a custom MATLAB (Mathworks, Natick, MA) tool. Measurements were obtained using EnSight (ANSYS, Canonsburg, PA). Mean flow was quantified by two observers in the following cross-sections: proximal (PV1), middle (PV2), and distal (PV3) portal vein; close to hilum (SV1) and confluence (SV2) of splenic vein; and right (RPV) and left (LPV) portal veins. (Fig.1, Fig.2). The analysts categorized image quality as ‘analyzable’, ‘marginally analyzable’, or ‘unanalyzable’.
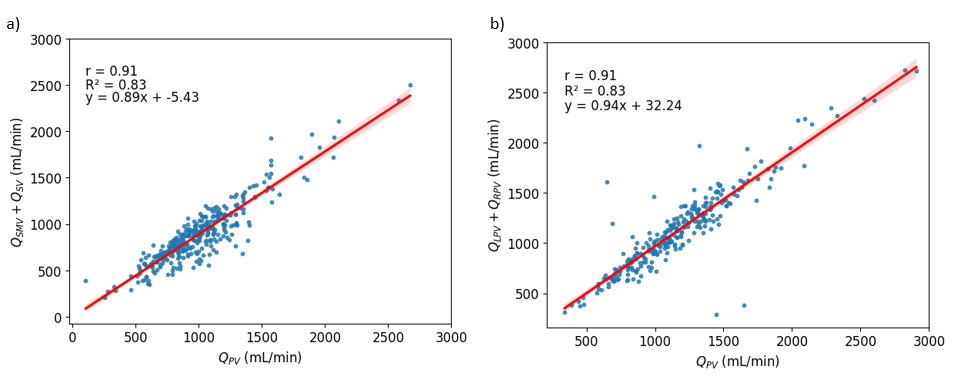
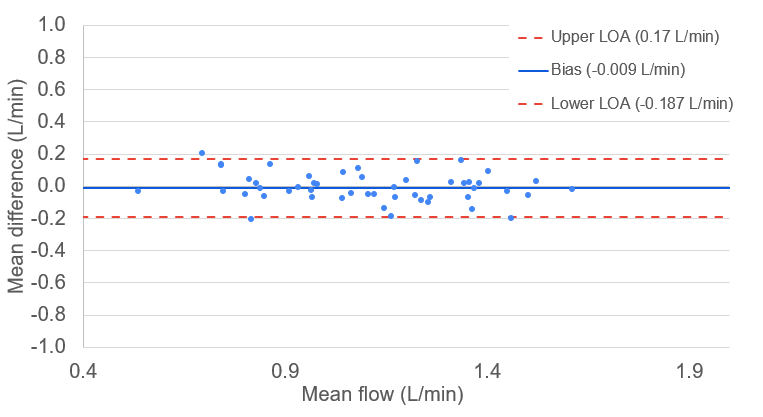
Mean portal venous flow was calculated from PV1, PV2, and PV3 planes. Internal consistency was based on conservation of mass, quantified by Pearson correlation coefficients across contiguous vessels: PV1 vs. (SMV+SV2); and PV3 vs. (LPV+RPV). Inter-observer agreement was assessed using Bland-Altman analysis.
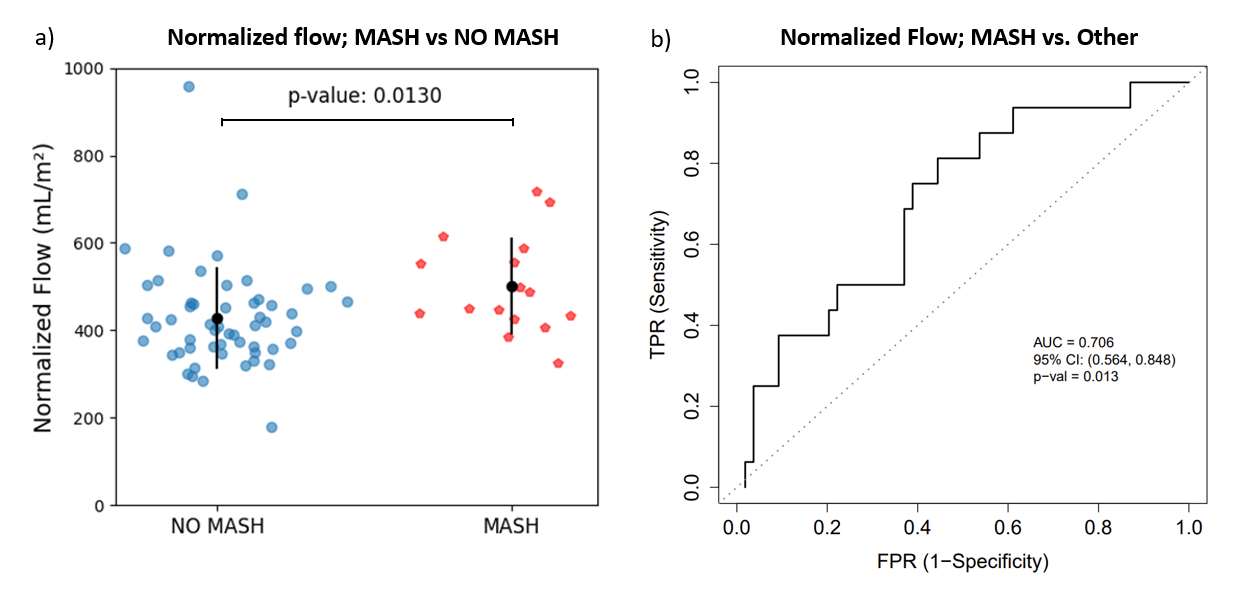
Cross-sectional Spearman's (rho) correlated flow with BMI at visit 1. Significance was computed using non-parametric bootstrap with per-patient resampling. Portal flow at Visit 2 normalized by body surface area (Du Bois formula17) was compared between subjects with MASH and ‘non-MASLD’ or ‘no MASH’ cross-sectionally. P-values were calculated using the Wilcoxon-Mann-Whitney test. Logistic regression was used to model MASH as a function of normalized flow. Predictive accuracy ROC assessment was based on the fitted model (Fig.5). Values are given as mean±SD. P-values<0.05 denoted significance.
Results
101 participants (87 women; 44±10years) were successfully enrolled. BMI decreased from 46±7kg/m2 to 34±6kg/m2 over the year following surgery. Of 382 MRI exams, 29 (7.6%) were excluded as ‘unanalyzable’ and 14 (3.6%) due to reconstruction failure; 276 (72.3%) ‘analyzable’ and 63 (16.5%) ‘marginally analyzable’ MRI exams were included.Conservation of mass analysis yielded strong correlation (r=0.91, Fig.3). Inter-reader analysis showed minimal bias (0.009L/min) within narrow limits of agreement (-0.187L/min,0.17L/min; Fig.4)
Portal flow showed positive correlation with BMI at Visit 1 (rho=0.32; p=0.0103). At Visit 2, participants with MASH (n=16) showed higher normalized portal flow than those without MASH (n=54) (501±111mL/m2 vs. 427±116mL/m2; p=0.013). Normalized portal flow differentiated between MASH and no MASH with an area under the curve (AUC)=0.706 (95%CI:[0.564,0.848]. A threshold of 384mL/m² excluded MASH with high sensitivity (sensitivity=0.94; specificity=0.39) while normalized flow >552mL/m² detected MASH with high specificity (sensitivity=0.38; specificity=0.91), (Fig.5).
Discussion
Despite the lack of contrast, 4D Flow MRI was feasible, and notably consistent in this morbidly obese cohort. Conservation of mass was excellent and matched results from prior contrast-enhanced studies3, with lower inter-reader bias14,18.The observed correlation of normalized portal flow and BMI, albeit weak, suggests a possible role for portal flow in obesity. Additionally, a significant difference in normalized portal flow in those with and without MASH suggests that portal flow has potential as a biomarker, and may provide insight into pathophysiology of MASH. Despite overlap between groups, normalized portal flow shows potential to identify patients at high risk for MASH. Future studies should also explore its potential for treatment monitoring.
Acknowledgements
The authors wish to acknowledge the NIH (R01 DK088925, R01 DK125783) and Pfizer Inc. for supporting this study, as well as GE Healthcare who provides research support to the University of Wisconsin. Dr. Reeder is the John H. Juhl Endowed Chair in the Department of Radiology. Dr. Oechtering received funding from the German Research Foundation (OE 746/1-1).
References
1. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatol Baltim Md. 2016;64(1):73-84. doi:10.1002/hep.284312. Ahmed A, Wong RJ, Harrison SA. Nonalcoholic Fatty Liver Disease Review: Diagnosis, Treatment, and Outcomes. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2015;13(12):2062-2070. doi:10.1016/j.cgh.2015.07.029
3. Oechtering TH, Roberts GS, Panagiotopoulos N, Wieben O, Reeder SB, Roldán-Alzate A. Clinical Applications of 4D Flow MRI in the Portal Venous System. Magn Reson Med Sci MRMS Off J Jpn Soc Magn Reson Med. 2022;21(2):340-353. doi:10.2463/mrms.rev.2021-0105
4. Stankovic Z, Csatari Z, Deibert P, et al. Normal and altered three-dimensional portal venous hemodynamics in patients with liver cirrhosis. Radiology. 2012;262(3):862-873. doi:10.1148/radiol.11110127
5. Balasubramanian P, Boopathy V, Govindasamy E, Venkatesh BP. Assessment of Portal Venous and Hepatic Artery Haemodynamic Variation in Non-Alcoholic Fatty Liver Disease (NAFLD) Patients. J Clin Diagn Res JCDR. 2016;10(8):TC07-TC10. doi:10.7860/JCDR/2016/20697.8267
6. Yeo SC, Ong WM, Cheng KSA, Tan CH. Weight Loss After Bariatric Surgery Predicts an Improvement in the Non-alcoholic Fatty Liver Disease (NAFLD) Fibrosis Score. Obes Surg. 2019;29(4):1295-1300. doi:10.1007/s11695-018-03676-5
7. Theel WB, Klerk BMB de, Dirksmeier-Harinck F, et al. Effect of bariatric surgery on NAFLD/NASH: a single-centre observational prospective cohort study. BMJ Open. 2023;13(7):e070431. doi:10.1136/bmjopen-2022-070431
8. Subichin M, Clanton J, Makuszewski M, Bohon A, Zografakis JG, Dan A. Liver disease in the morbidly obese: a review of 1000 consecutive patients undergoing weight loss surgery. Surg Obes Relat Dis. 2015;11(1):137-141. doi:10.1016/j.soard.2014.06.015
9. Głuszyńska P, Lemancewicz D, Dzięcioł JB, Razak Hady H. Non-Alcoholic Fatty Liver Disease (NAFLD) and Bariatric/Metabolic Surgery as Its Treatment Option: A Review. J Clin Med. 2021;10(24):5721. doi:10.3390/jcm10245721
10. Oechtering TH, Roberts GS, Panagiotopoulos N, Wieben O, Roldán-Alzate A, Reeder SB. Abdominal applications of quantitative 4D flow MRI. Abdom Radiol N Y. 2022;47(9):3229-3250. doi:10.1007/s00261-021-03352-w
11. Shamim AMKM, Panagiotopoulos N, Spahic A, et al. Fat mitigation strategies to improve image quality of radial 4D flow MRI in obese subjects. Magn Reson Med. 2023;90(2):444-457. doi:10.1002/mrm.29652
12. Johnson KM, Lum DP, Turski PA, Block WF, Mistretta CA, Wieben O. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. Magn Reson Med. 2008;60(6):1329-1336. doi:10.1002/mrm.21763
13. Johnson KM, Markl M. Improved SNR in Phase Contrast Velocimetry with 5-Point Balanced Flow Encoding. Magn Reson Med Off J Soc Magn Reson Med Soc Magn Reson Med. 2010;63(2):349-355. doi:10.1002/mrm.22202
14. Roldán-Alzate A, Frydrychowicz A, Said A, et al. Impaired regulation of portal venous flow in response to a meal challenge as quantified by 4D flow MRI. J Magn Reson Imaging JMRI. 2015;42(4):1009-1017. doi:10.1002/jmri.24886
15. Qu P, Zhong K, Zhang B, Wang J, Shen GX. Convergence behavior of iterative SENSE reconstruction with non-Cartesian trajectories. Magn Reson Med. 2005;54(4):1040-1045. doi:10.1002/mrm.20648
16. Walker PG, Cranney GB, Scheidegger MB, Waseleski G, Pohost GM, Yoganathan AP. Semiautomated method for noise reduction and background phase error correction in MR phase velocity data. J Magn Reson Imaging. 1993;3(3):521-530. doi:10.1002/jmri.1880030315
17. Du BOIS D, Du BOIS EF. CLINICAL CALORIMETRY: TENTH PAPER A FORMULA TO ESTIMATE THE APPROXIMATE SURFACE AREA IF HEIGHT AND WEIGHT BE KNOWN. Arch Intern Med. 1916;XVII(6_2):863-871. doi:10.1001/archinte.1916.00080130010002
18. Brunsing RL, Brown D, Almahoud H, et al. Quantification of the Hemodynamic Changes of Cirrhosis with Free-Breathing Self-Navigated MRI. J Magn Reson Imaging JMRI. 2021;53(5):1410-1421. doi:10.1002/jmri.27488
Figures